人~!f.liX Mi'hl 뽑깐"'tI誌 第 23 짤 ~ 2 싸 pp. 273 - 276, 1987 Journal of Korean Radiological Society, 23(2) 273-2761987
위에서 발생한 펑활근 아세포종 - 1 예 보고 -
고려영원 방사선과
함 소 희·박 해 원·우 원 형
- Abstract-
Leiomyoblastoma of the Stomach - A Case Report -
50 Hie Ham, M.D., Hae Won Park, M.D. and Won Hyung Woo, M.D.
Department of Radiology, Koryo General Hospital
Leiomyoblastomas are radiologically and grossly indistinguishable from the leiomyoma or leiomyosarcoma.
They tend to occur later in life, but attain the same size and shape and have the same sex attribution as the
。 thersmooth muscle tumors
The major difference is their histologic appearance. Leiomyoblastomas are composed primarily of rounded or polygonal cells with a clear space surrounding the nucleus instead of spindle cell mainly found in leiomyoma
。rleiomyosarcoma‘ Leiomyoblastomas are felt to have considerably more malignant potential than leiomyoma, but this has rarely been demonstrated. Exophytically growing tendency limits conventional barium studies. 50 recently CT is useful in depicting the origin, extend of these masses, and detection of distant metastasis. CT is an ideal imaging modality for study of this unusual neoplasm ‘
We report a case of exophytiç growing leiomyoblastoma from posterior wall of the stomach in 43 year old woman. We discussed with CT finding and reviewed the literature
1 .
서 론펑활근 아세포종응위에서 드물게 발생하는 종양이다.
세표질내 공포를자주 형성하는 원형세표로 보통 펑활 근종에서 보는 방추상 제 !t.대신 원형이나 다각형세포로 구성되고 대부분 핵 주위에 펑활근 섬유가 없다.
저자들은 최근 초음파 및 선산화단층촬영 (이하
CT
호 의빨)에서 위에서 발생해 소강내로 자란 종양이 뱅
이 논운응 1987년 2 월 28 일에 접수하여 1987년 3 월 28 얼에 채택되었음.
리조직학적으로 형활근 아세포종£로 증명되어 문헌 고 찰과 아울러 보고하는 바이 다.
n.
증 례주소 : 43 세 여자 환자로 수일깐 상복부 동통 및 압 통을 주소로 내원하였다.
과거력 : 24 세해 상훈부 동통이 7 개월간 있었으나,
특옐한 치료없이 증상이 없어졌다.
이학적 검사:상북부에서 약 5 x7cm 정도의 비교적 평탄한 표연을 가진 종괴가 촉지되었다.
- 273-
λM:!/;(~‘JJSt:협 l}~ttμ‘ 끼S23 if 껴~ 2 싸 1987 -
검사 소견 : 헬색소
369
만 Imm3• 백혈쿠6000/ mm
3’ 헤마토크리트(Hct) 33% .
소변검사상 정상, 기타 a-FP. CEA
모두 정상범위 였 냐.내시경 검사 :위대만곡 전체에 외부 앙박파 위체부에 앓은 궤양을 보였고 점악이 탈색되어 있었다.
방사선 소견 1. 단순 복부 촬영 ; 횡행결장을 아래호 전위시키는 연부조직 음영이 보였다.
2.
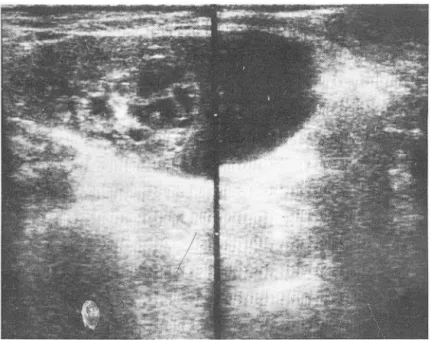
상부 위장판 조영술 ; 위체부 후벽과 위대만곡헤 외부압박만 있었다.3. 초음파 소견 ; 소강내 액체 성 저 류속에 고형 종괴가
A
닝k종성 변화로 격막을 형성한 것같이 보였다. 낭종속에 산재펀 저에코 부분이 있었다(Fig.
1).
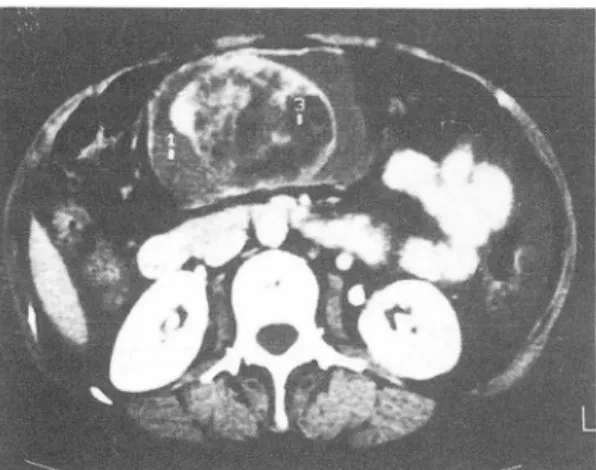
4. 복부 전산화 단층촬영 ;l1 X6.5X5cm의 크기로 추측되는 난형의 닝똥이 소강내 있 었으며 이는 위의 선 정부, 체부와 연속되어 보였다. 낭종내 고형종괴에서 초 음파소견과 일치하순 낭종성 변화를 볼 수 있었고 주변 의 저밀도 음영은 소강내 복수처럼 나타났다 그러나 조 영제 주업후 위 후벽을 따라 선상의 조영 증깅에 있어 소 캉내 복수보다 L8l종이 너 의섬되었다(Fig.2
and 3)
.수술 소견 :위 천정부와 체부의 후벽에 약간의 유착
Fig
1.Real-time ultrasonographic fin- dings of upp er abdomen.
transverse scan. A round mass in the left upper quadrant with both solid and cystic components was located between stomach and pancreas.
B
Fig 2. A & B: Cystic component of mass lesion is hardly differentiated from ascites in lesser sac. No metastases in liver and paraarotic lymph nodes.
- 274-
-함소회 외 : 위에서 딸생한 평활근아세포종-
Fig 3. Solid component of the mass lesion with surroun- ding cystic component. Multiple intema1
10w den-sities suggest tumoral necrosis
이 있고 혜장미부와도 어느 정도 유착된,앓은외막을 가 진 낭종이 소강내에 있었다. 박리하던중 파열되어 고형 종괴와 같이 출혈이 섞인 괴사물질이 나왔고 소강내 복 수는 확인할 수 없었다.
병리학적 소견 1. 육안적 소견 ;
10 x 7 x 6 cm
크기 의 진한 칼색 및 노란색의 연조직종괴로, 단연에는 중심 부로 자라난 돌기모양의 고형종괴가 주위 닝L종£로 싸여 있고 그 속에 불규칙하게 퍼진 출혈부위가 있었다. 종 괴는 위후벽에서 기시하였다.2.
현미경적 소견 ; 종괴는 불규칙한 유상jl.1 형 세포(epitheloid cell)
열파 출혈된 부위로 구성되어 있었 다. 큰 유상파형 세포블을 난형의 큰 핵과 호산성 세포 질을 가지고 있 었다. 위에서 기시된 비교적 두꺼운 펑 활근 섬유다발과 주변부에Auerbach
plexus 를 볼 수Fig 4. The epitheloid large cells have ovoid large nuclei and eosinophilic
gran비es.Scattered hemorrhages were seen.
있었다.
체세포 분열체 (Mitotic figure) 는 50HPF 당 5 개 미만이었다 (Fig.4).
m.
고 찰1960
년Martin
파 그 연구진이 위 벽에 서 생 기는 종 양으로 평활근 육종과 달리 특징적 S로clear zone
과 공포를 가진 둥글거냐 다각형의 세포들로 구성되어 있는 6 예의 평활근 아세포종을 보고했고, 2 년 뒤Stout
등 이 69 예의 연우에서 이 종양을bizarre leiomyobl-
astoma
(평활근 아세포종)로 처음 기술하였다 1- 시 지금까지 250 여예의 보고가 있는 비교적 드운 종양 이며 85% 가 40 셰 이상에서 냐타났으며 낭녀비는St-
out
에 의하연3 : 2
, Abranson 에 의하면9:7
정도호 낭자에 다소 많은 것으로 되어 있다 3 ,석주 증상은 상복부 동통 및 불쾌감, 종괴촉진, 체중감 소, 위궤양증세 등이 있고 궤양이 생긴부위에서 출혈이 심하게 일어날 수 있다 5 , 6). Abranson 에 의하연
27.3%
가 평소에 증상이 없었으며 우연히 수술 등에서 발견되 었다 7)
종양의 발생부위는 위장판 어느 부위에서냐 생걸 수 있다. 그러냐 다른 정악하 종양이나 간엽조직 (Mesenc
hymal
tissue)성 종양이 체부와 저부셰 잘 생기는데 비해 90% 이상이 위 천정부에서 호말한다. 대캐 단일 성으로 오지만 다발성도 6.8% 냐 보고되었마 2 , 5 , 6:종양은 대부분 위내강으로 자라냐 sess
ile
,Pedunc-
비 ated, 혹은 dumbell-shape 의 모양을 보여주는데,약 15~18% 에서 위 밖무로 자라나 복강내 종괴로 나 타난다. 냥상 변화가 있어 매우 커질 수 있고 고형성과 낭상이 혼합된 종양의 단연은 출혈파 괴사를 보여줄 수
있다 3 , 9-13:
본 예에서 닝」종속에 고형 종괴가 있어 CT와 초읍 파 소견상 마치 소강내 복수가 있고 고형 부우1 만01 종 양인 것으로 요인될 수 있 었다. 또 완전히 위 밖으로 자라났고 위 천정부와 체부만이 약간의 유착이 있는 것 무호 보여 주위 장기에서 기시한 종양과 감열을 요했다.
종종 뱅변이 땅사선고벼 A로 위와 판계가 없는 것 처 럼 보여 수술전 혜장닝l종S 로 진단된 경우도 보고되 었 다인
특히 이 종양을 진단하는데 중요한 조직 학적 소견은 펑활근종이냐 평활근육종에서 보는 '!J추형 세포대신 풍
- 275
-- 大합liX.射앓醫짱장誌 : 第23卷 第2 號 1987 -
부한 호산정 세 포질내 공포와 c1ear zone 을 갖는 유 상펴형 세포로 구성되어 있다.
대부분응 익양성이고 몇 예에서만 악성을 나타내었마 14.
15) 이 악성을 결정짓는 요소로 Stout 및 Levin등은 세포분열상을 주장하였다. 그 기준은 50/50 HPF 이상 일 해 악성 S로 보고 6/50HPF 이하시 양성으후 보았 지만 이에 대해서는 학자들 간에 이견이 있다 2 , 8).
생존율은 위 절제 술후 좋다고 기존운현에 보고되어 있 으냐 Lavin과 그 연구진은 사 0,)--율이 위벽 종양。l연 38
%. 위밖 종양이연 60%. lOcm 이상 크기연 80%. 1/
1 HPF 이상이연 31 %로 보고하였다6 , 8 , 16~
그러냐 Abranson보고에는 종양의 크기, 세포분열율,
악성정도는 연관이 없고 양성인 종%벼1 서도 수술 후 몇 년 뒤 전위가 된 경우도 있다7) 전이는 주로 간으로 되 며 인접장기로의 직접천이는 그보다 빈도가 떨어진다.
Castro등운 긴 기간의 추적조사로 원격장기의 천이의 유무어l 짜라 진정한 악성여부를 가릴 수 있다고 했다 16)
본 예에서는 5/50 HPF 미만으로 세포분열상이 있고 다른 장기로의 전이가 없었무으로 양성으로 판단되지만 충분한 추적조사가 필요하다.
종양 발견에 있어서도 위내벽 혹은 위내캉으로 자라 냐는 경우 위장관조영술에서 읍영결손이냐 궤양 등으호 찾을 수 있으냐, 위 밖으로 자라는 경우 종양 및 그기시 부를 보기가 힘들다. 이때 CT 와 초음파검사는 종양의 기시부와 침뱀부위, 인정장기와의 유착 및 전이, 원격전 이를 볼 수 있고 그것£로 악성여부를 강벌할 수 있는 단서를제공한다.
특히 CT에서는 양성보마 악성이 어 크고불규칙적이 며 조영제 주입시 머 다양한 응영증강을 보여준마 3)
N.
결 론위장관조영술에서는 정상이었£나 위체부에서 발생해 소캉내로 돌출된 평활근 아세포종 1예를 경험하고 운 헌적 고찰을 하였다. CT와 초음파검사에서 이 종양의 낭상 뱅 변부위 가 소강내 복수와의 감별이 힘들었으나 진 단과 전이에 의한 악성여부을 보는데는 이플이 가장 이 상적인 방법이다.
REFERENCES
1 권오상, 양운호, 박용철 : 위에 발생한 펑활근아세포 종. 대한방사선학회지 20: 855-858. 1978
2. 5tout AP: Bizarre smooth muscle tumors of the stomach Cancer 15:400-409, 1969
3. 51asky B5, Denese L, 5kolnick ML: Exogastric leiomyoblastoma diagnosis by CT and ultrasonography South Med
J
75:1275-1277, 19824. Bose B, Cancy J: Castric leiomyoblastoma. Cut 11:875-880, 1970
5. Tanghe W, Braeckman V, Noyez D’ The leiomyoblastoma of the stomach. Castro intest 13:244, 1970
6. Mann N5, 5achdev AJ, Agrawal AB, et al‘ Leiomyoblastoma of the stomach. South Med J 68:1350-1352, 1975 7. Ahranson DJ: Leiomyoblastoma of the stomach. Surg Cyu
Obst 136:118. 1973
8. Lavin P5, Hajdu F, Foote JR: Castic and extragastric leiomyoblastoma. Cancer 29:305, 1972
9 오승근 Leiomyoblastoma of the stoma
Ch .
대한외파학회지 15 : 37-42. 1973
10. Herrington J: Leiomyoblastoma of stomach. Br
J
Surg 52:928, 196511. Faegenhurg D, Farman
L
Dallemand 5, et al:Leiomyoblastoma of the stomach. Radiology 117:297-300, 1975
12. Gupta R, Chandler J: Leiomyoblastoma of the stomach Ann surg 161:562, 1965
13. 5innreich κ1, Friedman R, Dasco MR, et al: Bizarre gastric leiomyoblastoma simulating a pedunculated uterine fibromyoma. Obstet and Cynec 27:690-694, 1966 14. Kay 5, 5till WJ: A comparative electron microscopic study
of a leiomyosarcoma and biazrre leiomyoma (Ieiomyoblastoma) of the stomach. Am J Clin Pathol 52:403, 1969
15. Hajdu 51, Erlandson RA, Paglia MA: Light and electron microscopic studies of a gastric leiomyoblastoma. Arch pathol 93:36-41, 1972
16. Castro Fj, Olsen WR: Castric leiomyoblastoma in an adolescent. Am