This work was supported by the Korea Research Foundation Grant funded by the Korean Government (MOEHRD) (KRF-2006-331- E00122).
Address for correspondence: Kyung Ho Kang, M.D., Ph.D.
Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Korea University Guro Hospital, 80, Guro 2-dong, Guro-gu, Seoul 152-703, Korea
Phone: 82-2-2626-3028, Fax: 82-2-865-9670, E-mail: [email protected] Received: May. 20, 2009
Accepted: Jul. 2, 2009
ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2009;67:95-104
CopyrightⒸ2009. The Korean Academy of Tuberculosis and Respiratory Diseases. All rights reserved.
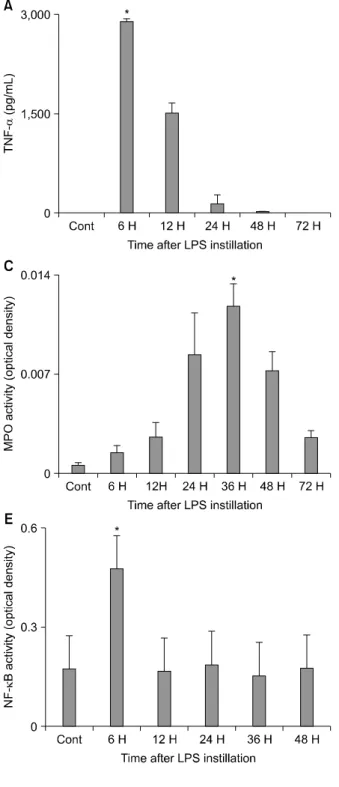
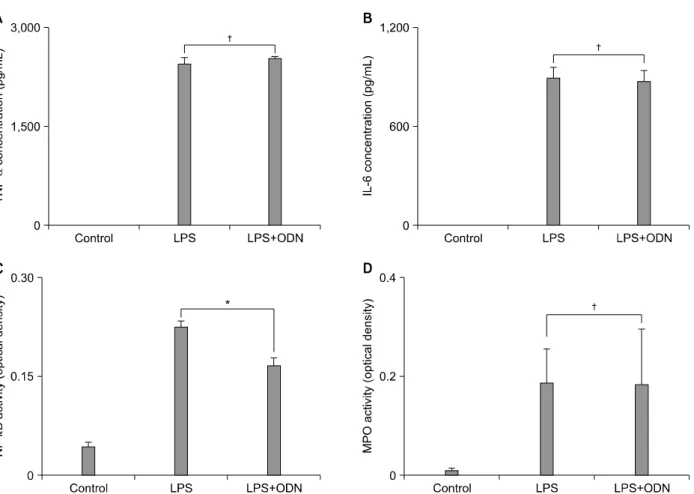
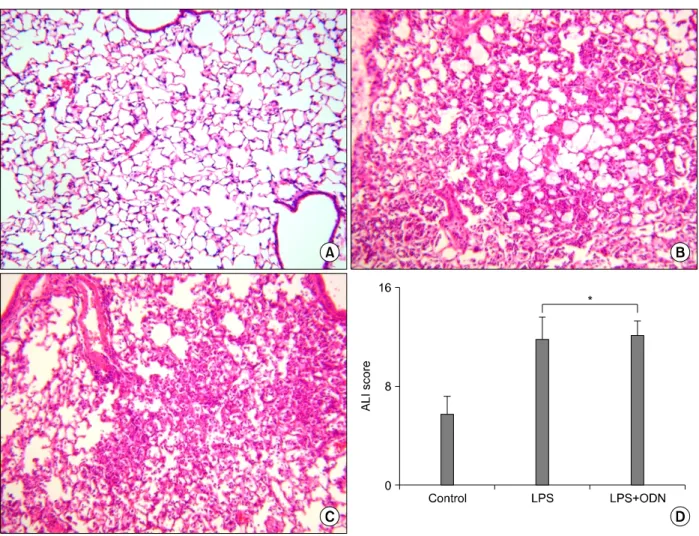
The Effects of Nuclear Factor-κB Decoy Oligodeoxynucleotide on Lipopolysaccharide-Induced Direct Acute Lung Injury
1
Division of Pulmonary, Sleep and Critical Care Medicine, Department of Internal Medicine, Korea University Ansan Hospital, Ansan,
2Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Korea University Guro Hospital,
3Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Korea University Anam Hospital, Seoul, Korea
Je Hyeong Kim, M.D., Ph.D.
1, Dae Wui Yoon, M.S.
1, Ki Hwan Jung, M.D.
1, Hye Ok Kim, M.D.
2, Eun Sil Ha, M.D.
3, Kyoung Ju Lee, M.D., Ph.D.
2, Gyu Young Hur, M.D., Ph.D.
2, Sung Yong Lee, M.D., Ph.D.
2, Sang Yeub Lee, M.D., Ph.D.
3, Chol Shin, M.D., Ph.D.
1, Jae Jeong Shim, M.D., Ph.D.
2, Kwang Ho In, M.D., Ph.D.
3, Se Hwa Yoo, M.D., Ph.D.
3, Kyung Ho Kang, M.D., Ph.D.
2리포다당질로 인한 직접성 급성폐손상에서 Nuclear Factor-κB Decoy Oligodeoxynucleotide의 효과