J Korean Soc Transplant
2008;22:135-137 □ 증 례 □
135
책임저자:나현희, 서울시 중구 저동 2가 85번지 서울백병원 내과, 100-032
Tel: 02-2270-0945, Fax: 02-2265-6875 E-mail: [email protected]
이식신과 이식신 주위에 발생한 침습성 아스페르길루스증 1예
인제대학교 의과대학 서울백병원 내과학교실, 1외과학교실, 2마취과학교실, 3해부병리학교실,
4부산백병원 흉부외과학교실
나현희ㆍ홍성우1ㆍ김문철2ㆍ강윤경3ㆍ윤영철4ㆍ고행일
A Case of Invasive Aspergillosis in Transplanted Kidney and Perirenal Area
Hyun Hee Na, M.D., Seong Woo Hong, M.D.
1, Mun CheolKim, M.D.
2, Yun Kyung Kang, M.D.3, Young Chul Yoon, M.D.4 and Haeng Il Koh, M.D.Departments of Internal Medicine, 1General Surgery, 2Anesthesio- logy and 3Pathology, Seoul Paik Hospital, Seoul, 4Department of Thoracic and Cardiovascular Surgery, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea
Recently, the incidence of fungal infection increases because of immunosuppressive therapy and chemotherapy. In immu- nosuppressed transplant recipients, Aspergillus can be a dangerous pathogen, capable of inducing fulminant clinical disease. Invasive fungal infections are life-threatening com- plications in solid-organ transplantation. Although the rate of fungal infections in transplant recipients is lower than that of other infections, the mortality rate is higher. A 34 year-old male was admitted to our hospital with fever and gross hematuria. He had received renal transplantation 2 years ago and had been transferred the other hospital 1 month ago.
Initial laboratory data evaluation showed a pancytopenia and azotemia. We thought that pancytopenia was caused by immunosuppressive agents and infection. The patient was treated with antibiotics but fever was not subsided. After 4 days, he complained of transplant site pain and tenderness to percussion. A percutaneous renal biopsy was performed.
Microscopic examination showed invasive aspergillosis in transplanted kidney and perirenal area. We removed the transplanted kidney and perirenal tissue, and prescribed antifungal agents for 3 months. (J Korean Soc Transplant
2008;22:135-137)
Key Words: Aspergillus, Invasive aspersillosis, Kidney
transplantation중심 단어: 아스페르길루스, 침습성 아스페르길루 스증, 신이식
서 론
최근 장기이식으로 면역억제제 사용의 증가와 악성종양 의 화학적 치료 요법의 증가로 인해 진균의 감염률이 증가 하고 있다. 그 중에 Aspergillus는 주위에 널리 존재하는 진 균으로 면역력이 정상인 경우 심각한 병원균은 아니지만 이식을 한 경우 면역억제제를 복용해야 함으로 심각한 병 원균으로 작용하여 이식신의 생존률을 감소시키고 환자의 사망률을 증가시킨다. 국내에서 Aspergillus 감염은 이식환 자에서 여러 보고가 있었으나 신이식 후 이식신 및 이식신 주위에 발생한 증례가 없어 보고하는 바이다.
증 례
환자: 34세 남자
주소: 5일 전부터 발생한 고열과 혈뇨
과거력 및 현병력: 통풍과 진통제인성 신병증으로 인한 말기 신부전으로 2년 전 중국에서 혈연관계가 없는 공여자 로부터 생체 신이식을 시행한 후 외래에서 추적관찰을 하 다 1달 전 타병원으로 전원된 환자였다. 2년 전 귀국당시 수술부위 감염으로 입원하여 항균제 치료를 받았고 1년 6 개월 전 급성 거부반응으로 스테로이드 충격요법을 받은 병력이 있었다. 4개월 전에는 요로폐색으로 인해 요로성형 술을 시행받고 수술부위의 감염으로 인해 1달간 항균제 치 료를 받았다. 전원 전에는 면역억제제를 하루에 tacrolimus 4 mg, mycophenolic acid 1,440 mg, solondo 5 mg을 복용하였 고 전원 후에는 하루에 cyclosporine 400 mg, azathioprine 200 mg, solondo 5 mg로 바꿔 복용하고 있었고 통풍이 심해 하 루에 allopurinol 100 mg과 colchicine을 간간이 복용하였다 고 한다.
신체검사: 혈압은 140/80 mmHg, 맥박은 92/분, 호흡수는 20/분, 체온은 38.5도이었다. 이식 수술 부위에 통증이나 압 통은 없었다.
검사소견: 혈액검사에서 혈색소 4.4 g/dL, 백혈구 190
136
대한이식학회지:제 22 권 제 1 호 2008
Fig. 1. Abdominopelvic CT shows perirenal hematoma or abscess with parenchymal defect of transplanted kidney.
Fig. 2. There is a cluster of Aspergillus hyphae on perirenal tissue (H&E stain, ×200).
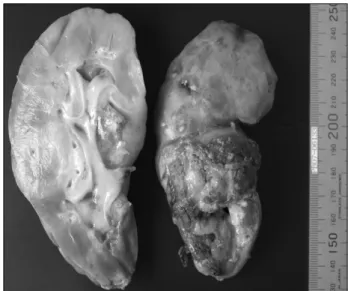
Fig. 3. This is the nephrectomy specimen of the transplanted kidney. At the lower pole and the mid portion, cavitary abscess measured 6.5×4.8×4.0 cm, markedly necrotic to hemorrhagic abscess.
Fig. 4. Abdominopelvic CT shows small multiple lesion suggested microabscess in liver and spleen (black arrow).
mm3 (과립구 7.2%, 임파구 85.7%), 혈소판 27,000 mm3으로 범혈구 감소증이 있었고 혈청 요소질소 및 크레아티닌은 103/5.0 mg/dL이었고 혈중 cyclosporine 농도는 193 ng/mL이 었다. 한 달 전 혈청 요소질소 및 크레아티닌은 57/3.8 mg/dL이었다. 소변검사는 단백 +3, 적혈구 시야 1/2 이상/
HPF이었다.
방사선 소견: 응급으로 시행한 신초음파 검사에서 신피질 의 음영이 전반적으로 증가되어 있었고 이식신의 크기와 수신증은 요로 성형술 이후 시행한 신초음파와 비교했을 때 변화는 없었다.
치료 및 경과: 소변감염 및 호중구 감소성 발열로 생각하 고 항균제와 과립구-대식구 집락자극인자를 투여하였으나 열은 지속되었고 범혈구 감소증도 호전되지 않았다. 내원 4일째 이식수술 부위의 발적을 동반한 통증 및 압통이 발생
하여 복부 전산화 단층촬영을 시행하였고 이식신 주위조직 과 이식신을 침범하는 혈종 및 농양이 의심되는 병변을 발 견하였다(Fig. 1). 당시 소변 및 혈액 배양검사에서 세균 및 진균은 분리되지 않았다. 복부 전산화 단층촬영에서 발견 한 이식신 주위조직에 대해 미세침 흡입 생검술을 시행하 였고 조직검사 결과 Aspergillus의 균사가 관찰되어 침습성 아스페르길루스증으로 생각하고 항진균제인 ambisome (liposomal amphotericin B)를 3 mg/kg/day로 투여하였다(Fig.
2). 이식신 제거 및 주위조직 제거를 위한 수술을 권하였으
나현희 외:이식신과 이식신 주위에 발생한 침습성 아스페르길루스증 1예
137
나 환자가 이식신 제거를 원하지 않아 면역억제제를 하루 에 cyclosporine 200 mg, solondo 15 mg을 유지하고 주위 조 직 제거술만 시행하였다. 조직 제거술 후 ambisome을 투여 하는 동안 열은 없었으며 범혈구감소증도 호전되었다.
Ambisome 투여 3주째 수술 부위에서 소변이 누출되며 혈청 크레아티닌이 상승하여 이식신을 제거하고 혈액투석을 하 였다(Fig. 3). 수술 후 시행한 복부 전산화 단층촬영에서 간 과 비장에 파종성 병변이 보여(Fig. 4) 경제적인 이유로 amphotericin B로 바꿔 2주 더 정맥주사하였고 이후 경구용 항진균제 itraconazole을 하루에 200 mg로 2달간 투여하였 다. 수술 3개월 후 시행한 복부 전산화 단층촬영에서 간과 비장에 보였던 파종성 병변은 보이지 않았다.
고 찰
신이식 환자의 경우 1년 이내에 80% 이상에서 적어도 한 번의 감염을 경험하며 급성 거부반응 등의 치료를 위해 면 역억제제의 용량을 증량할 경우 기회감염의 확률은 높아진 다.(1-3) Aspergillus 감염의 경우 신이식 후 0.6∼3.7% 정도 발생하는 것으로 보고되고 있다.(4) 발병 기전으로는 공기 로 흡입된 Aspergillus에 대한 알러지 반응이나 공동내에서 집락을 형성하는 경우, 직접 조직내로 침범하는 경우가 있 다.(5) 이외에도 신이식 환자에서 드물게 감염된 장기에 의 해서 발생하거나(6) 타인에게서 전염될 수도 있으며(7) 원 발병소없이 이식신에 감염된 경우도 보고가 되었다.(8,9) Aspergillus 감염이 의심되는 경우 배양검사와 조직검사를 시행하게 되는데 신이식 환자에서 Aspergillus 배양율이 3%
미만으로 배양을 통해서 알기가 어렵고 의심이 되는 병변 의 조직검사를 통해 확진을 할 수 있으므로 진단에 어려움 이 있다.(10)
침습성 아스페르길루스증의 치료를 보면 일반적으로 항 진균제인 amphotericin B를 투여하는데(11) 최근에는 이식환자 에서 itraconazole, voriconazole, flucytosine 등의 다른 항진균 제의 단독요법 또는 amphotericin B와의 병합요법을 보고하 고 있다.(12-15) Linden E 등(9)은 이식신에 발생한 아스페르 길루스증을 이식신 제거없이 배농과 항진균제 투여로 치료 를 한 증례를 보고하고 있다.
본 증례는 소변, 혈액배양검사를 여러 번 시행하였으나 Aspergillus가 분리되지 않았고 결국 조직검사를 통해 확진 을 하였으며 호흡기 감염이나 혈액으로의 파종성 전파경로 없이 이식신과 이식신 주위로 침범하여 Aspergillus의 감염 경로 또한 알기가 어려웠다. 치료는 amphoterin B를 투여한 후 경구 항진균제인 itraconazole을 2달간 유지하였다. 본 증 례의 경우 범혈구 감소증이 약제로 인한 것으로 생각되며 이처럼 면역력 저하가 심한 상태에서 Aspergillus가 이식신 을 침범한 경우 이식신을 포기해야 할 뿐만 아니라 환자의 생명도 위태롭게 만드는 일이 생길 수 있으므로 면역억제
제의 선택 및 용량조절, 병용약물의 선택에 더 많은 주의가 필요할 것으로 생각된다.
REFERENCES
1) Peterson PK, Balfour HH, Fryd DS, Ferguson RM, Simmons RL. Fever in Renal transplant recipients: cause, prognostic significance and changing patterns at the University of Minnesota Hospital. Am J Med 1981;71:345-51.
2) Chugh KS, Sakhuja V, Jain S, Talwar P, Minz M, Joshi K, Indudhara R. High mortality in systemic fungal infections following renal transplantation in third world contries. Nephrol Dial Transplant 1993;8:168-72.
3) 마명신, 김원, 강석귀, 유희철, 조백환, 김영곤, 구자홍, 박 성광. 신이식 후 발생한 거대세포바이러스와 아스페르길 루스에 의한 폐렴 1예. 대한이식학회지 1999;13:337-43.
4) Chugh KS, Sakhuja V, Jain S, Singh V, Tarafdar A, Gupta KL, Minz M. Fungal infections in renal allograft recipients.
Transplant Proc 1992;24:1940-2.
5) 박재형, 이윤정, 박상현, 최선영, 이미숙, 김지훈, 박수길.
신장이식 환자에서 피부 Aspergillosis 와 Aspergillus 갑상 염을 보인 파급성 Aspergilosis 1예. 대한내과학회지 2001;
60:86-91.
6) Keating MR, Guerrero MA, Daly RC, Walker RC, Davies SF.
Transmission of invasive Aspergillosis from a subclinically infected donor to three different organ transplant recip ients.
Chest 1996;109:1119-24.
7) Polkey M, Rees PJ, Ogg C. Possible person-to-person trans- mission of Aspergillus. Lancet 1993;342:435.
8) Maranes A, Portoles J, Blanco. Aspergillus infection of a renal allograft without evidence of a site of origin. Nephrol Dial Transplant 1996;11:1639-42.
9) Linden E, Restrepo D, Dikman S, Murphy B, Huprikar S.
Aspergillus infection limited to renal allograft: case report and review of literature. Transpl Infect Dis 2006;8:177-81.
10) Brown RS Jr, Lake JR, Katzman BA, Ascher NL, Somberg KA, Emond JC, Roberts JP. Incidence and signif icance of Aspergillus cultures following liver and kidney transplantation.
Transplantation 1996;61:666-9.
11) Dennig DW. Therapeutic outcome in invasive aspergillosis.
Clin Inf ect Dis 1996;23:608-15.
12) Tsiodras S, Zafiropoulou R, Giotakis J, Imbrios G, Antoniades A, Manesis EK. Deep sinus aspergillosis in a liver transplant recipient successfully treated with a combination of caspo- fungin and voriconazole. Transpl Infect Dis 2004;6:37-40.
13) Baden LR, Katz JT, Fishman JA. Salvage therapy with vorico- nazole for invasive fungal infections in patients failing or intolerant to standard antifungal therapy. Transplantation 2003;
76:1632-7.
14) Fortun J, Martin-Davila P, Sanchez MA. Voriconazole in the treatment of invasive mold infections in transplant recipients.
Eur J Clin Microbiol Infect Dis 2003;7:408-13.
15) Herbrecht R, Denningdw, Pattersontf. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis.
N Engl J Med 2002;347:408-15.