http://dx.doi.org/10.12671/jkfs.2016.29.1.55
55
Copyright ⓒ 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received September 7, 2015 Revised October 20, 2015 Accepted November 17, 2015
Address reprint requests to: Joon Yub Kim, M.D., Ph.D.
Department of Orthopaedic Surgery, Myongji Hospital, Seonam University School of Medicine, 55 Hwasu-ro 14beon-gil, Deokyang- gu, Goyang 10475, Korea
Tel: 82-31-810-6530ㆍFax: 82-31-969-0500 E-mail: [email protected]
Financial support: None. Conflict of interest: None.
Neer 제II형 원위 쇄골 골절에서 갈고리형 금속판 고정술 후 발생한 금속판 주위 골절
- 3예 보고 -
김경용⋅김준엽* ⋅이원복⋅정명곤*⋅유정현*⋅김주학*
중앙대학교 의과대학 해부학교실, 서남대학교 의과대학 명지병원 정형외과학교실*
Periprosthetic Fracture after Hook Plate Fixation in Neer Type II Distal Clavicle Fracture
- A Report of 3 Cases -
Kyung Yong Kim, M.D., Ph.D., Joon Yub Kim, M.D., Ph.D.* , Won Bok Lee, M.D., Ph.D., Myong Gon Jung, M.D.*, Jeong Hyun Yoo, M.D., Ph.D.*, Joo Hak Kim, M.D., Ph.D.*
Department of Anatomy, Chung-Ang University College of Medicine, Seoul,
Department of Orthopaedic Surgery, Myongji Hospital, Seonam University School of Medicine*, Goyang, Korea
Hook plate fixation is a treatment method for the displaced distal clavicle fracture with favorable results regarding bone union and shoulder function, however possible complications include impingement syndromes, subacrormial erosions, acro- mial fractures, and periprosthetic fractures. In this report, we observed 3 cases of periprosthetic fracture after hook plate fixation. All cases of periprosthetic fractures were initiated at the medial end screw holes. The causes of these periprosthetic fractures appeared to be the off centered fixation of medial end screws near the anterior or posterior cortex which were specific during operations with hook plates with more than 6 holes and the increased stress on the medial end screw by over-reduced or inferiorly reduced position of the distal end of the clavicle by the hook plate.
Key Words: Clavicle, Fracture, Periprosthetic fracture, Hook plate
Neer 제II형 골절은 불유합, 지연유합 및 부정유합이 발 생될 확률이 높은 골절로 수술적 치료가 대부분에서 필요
하게 된다.1-4) 외측 1/3이 전위된 원위 쇄골 골절의 수술적 치료로 다양한 술식이 있으나 갈고리형 금속판(hook plate) 을 이용한 수술방법도 만족할 만한 골유합 및 기능적 향상 을 가져온다고 보고되고 있다.5) 그러나 갈고리형 금속판과 관련된 합병증으로 충돌증후군, 견봉 미란, 견봉 골절 등이 잘 알려져 있으며,5,6) 드문 합병증으로 금속판 주변부 골절 이 몇몇 저자들에 의해 보고되고 있다.7-10) 저자들은 Neer 제II형 골절의 갈고리형 금속판을 이용한 관혈적 정복술 및 내고정술 후 발생한 금속판 주변부 골절 3예를 경험할 수 있었으며, 이 3예를 컴퓨터 단층촬영, 수술 중 소견과 갈고
56 Kyung Yong Kim, et al.
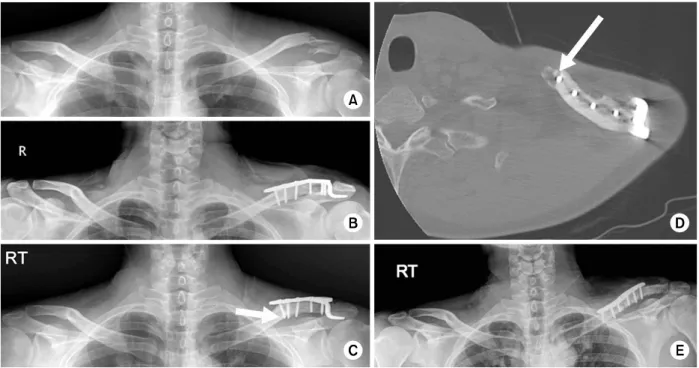
Fig. 1. (A) Neer type IIa distal clavicle fracture. (B) Open reduction and internal fixation with clavicular hook plate. (C) Medial end of the clavicular hook plate had migrated superiorly and medial end screw lost the fixation to inferior cortex (white arrow). (D) Axial cut of 2-dimensional computed tomography. The medial end fracture at the medial screw of the hook plate was observed (white arrow). (E) Open reduction and internal fixation with clavicular anatomical plate for newly onset fracture after removal of the hook plate.
리형 금속판의 사체 적용을 통해 갈고리형 금속판의 형태 학적 문제 및 술식의 문제를 고찰해 보았다.
증례 보고
1. 증례 1
49세 회사원인 남자 환자로 축구 경기중 좌측 어깨를 바 닥에 부딪치는 손상으로 내원하여 Neer IIa 원위 쇄골골절 진단하에 6홀의 갈고리형 금속판(clavicular hook plate;
Synthes, Bettlach, Switzerland)을 이용한 관혈적 정복술 및 내고정술을 시행하였다(Fig. 1A, B). 수술 후 5개월째 벽에 부딪치는 수상 후 수술 부위의 어깨 통증이 지속되어 촬영 한 단순 방사선 검사에서 갈고리형 금속판 내측단의 상방 전위가 관찰되었으며, 2차원 컴퓨터 단층촬영 영상(2-dime- nsional computed tomography, 2D CT)에서 갈고리형 금 속판의 내측단 나사못 전하방 삽입부에서 시작되는 골절을 발견할 수 있었다(Fig. 1C, D). 기존의 골절은 유합되었다 는 판단하에 새로 생긴 쇄골 간부 골절에 대해 3.5 mm 상부 쇄골용 잠금압박 금속판(3.5 mm LCP superior clav- icular plate; Synthes, Oberdorf, Switzerland)을 이용하여,
관혈적 정복술 및 내고정술을 시행하였다(Fig. 1E).
2. 증례 2
61세의 남자 환자로 내원 직전 자전거를 타다가 넘어지 면서 수상하였으며, 단순 방사선 검사상 좌측 견관절 Neer type IIa의 원위 쇄골 골절로 진단되었다(Fig. 2A). 6홀의 갈고리형 금속판을 이용한 관혈적 정복술 및 내고정술을 시행하였고(Fig. 2B), 수술 후 7주째 수면중 자세변경 시 갑작스런 어깨 통증이 발생하여 응급실로 내원하였으며, 갈고리형 금속판 내측단 나사못 삽입부에서 시작되는 금속 판 주변부 골절 및 내측단의 상방 전위를 단순 방사선 검 사상 확인할 수 있었다(Fig. 2C). 수술 전 2D CT에서 내 측단 나사못 삽입부 하방 및 근접한 외측 나사못 삽입부 하방의 골절선을 확인할 수 있었다(Fig. 2D). 수술시에도 동일 소견을 관찰할 수 있었으며(Fig. 2E), 3.5 mm 상부 쇄골용 잠금 압박 금속판(Synthes, Oberdorf)을 이용하여 관혈적 정복술 및 내고정술과 오구돌기와 간부에 2호의 Fiber wire (Arthrex, Naples, FL, USA)를 이용한 원형 결 찰(cerclage) 방법으로 추가적인 보강술을 시행하였다(Fig.
2F).
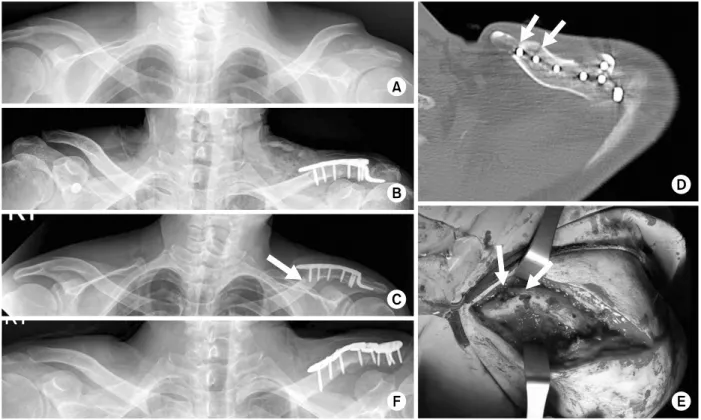
Fig. 3. (A) Neer type IIb distal clavicle fracture. (B) Open reduction and internal fixation with clavicular hook plate. (C) Medial end of the plate had migrated superiorly (white arrow). (D) Axial cut of 2-dimensional computed tomography of the medial end fracture. The fracture started from inferior portion of medial end screw to the unused drill hole which was located anterolaterally to the medial end screw (2 white arrows). (E) Open reduction and internal fixation with clavicular anatomical plate and reconstruction plate as well as K-wires was performed for the revision surgery.
Fig. 2. (A) Neer type IIa distal clavicle fracture. (B) Open reduction and internal fixation with clavicular hook plate. (C) Fracture at the medial screw of the hook plate was observed and medial end screw lost the fixation to inferior cortex (white arrow). (D) Axial cut of 2-dimensional computed tomography (CT) showed the fracture line communicating the medial two holes of the hook plate (2 white arrows). (E) Clinical photo corresponded to the CT findings (2 white arrows). (F) Open reduction and internal fixation with clavicular plate with cerclage wiring with No. 2 fiber wire between coracoid process and clavicular shaft.
58 Kyung Yong Kim, et al.
Fig. 4. (A) A 4-hole clavicular hook plate was applied and all holes were in appropriate position on the clavicle. (B) A 5-hole clavicular hook plate was applied and all holes were in appropriate position on the clavicle. (C, D) A 6-hole clavicular hook plate was applied and the most medial hole was slightly off centered and anteriorly positioned to the clavicle (C: from cranial to caudal view, D: from caudal to cranial view). (E, F) A 7-hole clavicular hook plate was applied and the most medial hole was definitely off centered and anteriorly positioned to the clavicle (E: from cranial to caudal view, F: from caudal to cranial view).
3. 증례 3
54세의 노동자인 남자 환자가 자전거를 타다가 넘어지면 서 우측 어깨를 바닥에 부딪쳐 내원하였다. 단순 방사선 검사상 Neer type IIb의 골절 양상을 확인할 수 있었으며, 갈고리형 금속판을 이용하여 관혈적 정복술 및 내고정술을 시행하였다(Fig. 3A, B). 수술 후 4주째 우측 손으로 바닥 을 짚고 일어나다가 갑작스런 어깨 통증이 시작되어 다시 내원하였고, X-ray 검사상 갈고리형 금속판의 내측단이 상 방 전위되는 양상이 관찰되었으며, 2D CT 검사상 후방 피 질골 근처로 삽입된 내측 나사못 삽입부 하방에서 시작되 는 골절선이 나사못이 삽입되지 않았던 드릴 천공부로 이 어지는 것을 확인할 수 있었다(Fig. 3C, D). 3.5 mm 상부 쇄골용 잠금 압박 금속판(Synthes, Oberdorf)을 쇄골 상방에 3.5 mm 재건 금속판(reconstruction plate; Synthes, Oberdorf) 을 쇄골 전방에 위치시켜 고정술을 시행하였고, 2개의 K- 강선을 이용하여 견봉에서 원위부 쇄골 골절 관혈적으로 통과시켜 정복되도록 하였다(Fig. 3E). K-강선은 3주 후에 제거하였다.
고 찰
불안정성 원위 쇄골골절에서 갈고리형 금속판은 술기의 편리함, 정복의 유지, K-강선에 비해 고정물의 이동 및 파 손을 피할 수 있다는 장점이 있으나 충돌 증후군, 회전근 개 손상 및 견봉의 미란, 견봉 골절 등의 합병증이 발생할 수 있으며 드물기는 하나 금속판 주변부 골절도 보고되고
있다.7-10) 금속판 주변부 골절이 발생한 대부분의 경우 선
행 외상 병력이 있으나,7-9) Ding 등10)의 경우 및 이번 증례 보고와 같이 동측의 팔에 약간의 힘이 가해지는 동작에도 골절이 발생할 수 있음을 알 수 있다. 금속판 주변부 골절 의 원인으로 전반적인 골다공증, 응력 차단 효과(stress shielding effect)에 의한 내측 나사못 삽입부의 부분적 골 다공증, 견봉-쇄골 관절의 움직임에 따른 내측단 나사못의 응력 유발자(stress riser)로서의 역할, 내측단 나사못 하방 부의 취약함 등이 원인으로 유추되고 있다.8,10)
Charity 등9)은 그들의 갈고리형 금속판 고정술 후 발생 한 금속판 내측단의 골절에 대해 보전적 치료로 만족할 만 한 결과를 얻었다고 하였다. 그들의 환자는 비록 금속판
내측 단의 돌출이 피부에서 만져지긴 하였으나, 팔을 90도 거상 시에도 통증이 거의 없어 보전적 치료를 결정하였다 고 하였다. Nadarajah 등8)과 Ding 등10)은 골절의 부정유 합, 불유합 가능성을 피하기 위해 수술적 치료를 시행하였 으며, 저자들의 경우 골절 후의 통증과 직업으로 인한 활 동성을 보장받기 원하는 환자들에게 이차 수술을 계획하였 다. 또한 저자들이 경험한 모든 예에서 갈고리형 금속판의 내측 단이 상방으로 전위된 양상이 방사선 검사상 관찰되 었고, 활동성을 원하는 환자들의 금속판에 의한 자극 및 보전적 치료를 통한 골절의 유합을 보장할 수 없어 수술적 치료를 결정하였다.
저자들이 3예의 금속판 주변부 골절에서 확인된 공통된 특징으로 첫째, 내측단 나사못 삽입부 하방에서 골절이 시 작된 양상이었으며 둘째, 전체 예에서 6홀의 갈고리형 금 속판에 의한 고정술 후 발생하였고, 내측단 나사못이 쇄골 의 전방 또는 후방에 치우쳐(off center) 삽입된 경향이 있 었다. 셋째, 골절이 작은 에너지에 의해 발생하였고, 마지 막으로 수술 후 쇄골의 방사선 검사상, 갈고리형 금속판에 의해 정복된 쇄골의 원위 말단부 위치가 견봉의 위치보다 하방에 위치할 정도로 과정복(over-reduction)되는 양상을 확인할 수 있었다(Fig. 1B, 2B, 3B).
저자들은 견봉-쇄골 관절의 과정복 또는 쇄골의 원위 말 단부의 견봉에 대한 상대적인 하방 위치가 갈고리형 금속 판의 내측 나사못의 스트레스 유발 역할에 기여하였을 것 으로 생각하였다. 또한 시제품인 갈고리형 금속판의 만곡 과 쇄골 만곡 모양이 일치하지 않아 내측 말단부의 나사못 의 전후방 피질골에 가깝게 치우쳐 삽입한 후 견봉-쇄골 관절이 움직이면서 내측 나사못 주변에 스트레스를 야기하 여 골절이 발생하는 가능성을 염두에 두었다. 실제로 한 구의 사체(여성, 나이 81세, 키 163 cm, 쇄골의 장축 길이 28 cm)를 이용하여 갈고리형 금속판을 외측에서 내측의 순서로 나사못의 구멍을 쇄골의 중앙에 위치시켰을 때 6홀 및 7홀의 갈고리형 금속판에서 가장 내측 홀이 전방 또는 후방으로 과도하게 향하게 되어 쇄골 위에 적절히 위치하 지 못하는 것을 확인하였다(Fig. 4). 이는 신체 크기가 작 은 동양인에게 기존 형태의 갈고리형 금속판이 적합하지 않음을 제시하는 것일 수 있다고 생각되고, 6홀 이상의 갈 고리형 금속판에서 만곡의 정도를 동양인에 적절한 해부학 적 변형이 필요하며, 이에 대해 추가적인 해부학적 연구가 필요하리라 생각하였다. 결론적으로 불안정성 쇄골 원위부 골절에서 갈고리형 금속판을 이용한 관혈적 정복술 및 내
고정술 시 금속판 주변부 골절의 가능성을 고려하여 금속 판의 해부학적 만곡을 고려한 적절한 대상 환자 선정 및 술식에 주의를 기울이는 노력이 필요하리라 생각된다.
References
1) Neer CS 2nd: Fracture of the distal clavicle with detach- ment of the coracoclavicular ligaments in adults. J Trauma, 3: 99-110, 1963.
2) Oh JH, Kim SH, Lee JH, Shin SH, Gong HS: Treat- ment of distal clavicle fracture: a systematic review of treatment modalities in 425 fractures. Arch Orthop Trauma Surg, 131: 525-533, 2011.
3) Tambe AD, Motkur P, Qamar A, Drew S, Turner SM:
Fractures of the distal third of the clavicle treated by hook plating. Int Orthop, 30: 7-10, 2006.
4) Fann CY, Chiu FY, Chuang TY, Chen CM, Chen TH:
Transacromial Knowles pin in the treatment of Neer type 2 distal clavicle fractures. A prospective evaluation of 32 cases. J Trauma, 56: 1102-1105, 2004.
5) Good DW, Lui DF, Leonard M, Morris S, McElwain JP: Clavicle hook plate fixation for displaced lateral-third clavicle fractures (Neer type II): a functional outcome study. J Shoulder Elbow Surg, 21: 1045-1048, 2012.
6) Meda PV, Machani B, Sinopidis C, Braithwaite I, Brownson P, Frostick SP: Clavicular hook plate for lat- eral end fractures:- a prospective study. Injury, 37: 277- 283, 2006.
7) Flinkkilä T, Ristiniemi J, Hyvönen P, Hämäläinen M:
Surgical treatment of unstable fractures of the distal clavi- cle: a comparative study of Kirschner wire and clavicular hook plate fixation. Acta Orthop Scand, 73: 50-53, 2002.
8) Nadarajah R, Mahaluxmivala J, Amin A, Goodier DW:
Clavicular hook-plate: complications of retaining the implant.
Injury, 36: 681-683, 2005.
9) Charity RM, Haidar SG, Ghosh S, Tillu AB: Fixation failure of the clavicular hook plate: a report of three cases.
J Orthop Surg (Hong Kong), 14: 333-335, 2006.
10) Ding M, Ni J, Hu J, Song D: Rare complication of clav- icular hook plate: clavicle fracture at the medial end of the plate. J Shoulder Elbow Surg, 20: e18-e20, 2011.
Copyright ⓒ 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ISSN 1225-1682 (Print)⋅ISSN 2287-9293 (Online) 대한골절학회지 제 29 권, 제 1 호, 2016년 1월
J Korean Fract Soc 2016;29(1):55-60 http://dx.doi.org/10.12671/jkfs.2016.29.1.55
■ Case Report ■
Neer 제II형 원위 쇄골 골절에서 갈고리형 금속판 고정술 후 발생한 금속판 주위 골절
- 3예 보고 -
김경용⋅김준엽* ⋅이원복⋅정명곤*⋅유정현*⋅김주학*
중앙대학교 의과대학 해부학교실, 서남대학교 의과대학 명지병원 정형외과학교실*
전위된 원위 쇄골 골절에서 갈고리형 금속판을 이용한 정복 및 고정술은 골절의 유합 및 기능적 측면에서 만족할만한 결과를 나타내는 것으로 알려져 있다. 그러나 갈고리형 금속판과 관련된 잘 알려진 합병증으로 충돌증후군, 견봉의 미란 및 골절 등이 알려져 있으며, 금속판 주변부 골절도 드물게 발생한다. 저자들은 Neer 제II형의 원위 쇄골 골절의 갈고리형 금속판 고정술 후, 3예의 금속판 주변부 골절의 발생을 경험하였다. 전체 예에서 금속판 내측단의 나사못 삽입부에서 기시된 골절을 확인하였으 며, 이의 원인으로 6홀 이상의 갈고리형 금속판의 내측단 나사못이 전방 또는 후방 피질골 면에 가깝게 삽입되는 문제와 쇄골 외측 말단부의 과도한 정복 또는 하방 정복으로 인한 내측단 나사못 부위의 스트레스 증가인 것으로 판단되어 이에 대해 기술하 고자 하였다.
색인 단어: 쇄골, 골절, 금속판 주변부 골절, 갈고리형 금속판
접수일 2015. 9. 7 수정일 2015. 10. 20 게재확정 2015. 11. 17 교신저자 김준엽
10475, 고양시 덕양구 화수로 14번길 55, 서남대학교 의과대학 명지병원 정형외과학교실 Tel 031-810-6530, Fax 031-969-0500, E-mail [email protected]
60