[H한밤사선의학회지 1998; 39: 399-401
상완골골단을침범한고렵성 골낭종의 방사선학적 소견 : 1예 보고l
이 범 하 · 류 경 남· 박 용 구2. 한 정 수3
고립성 골낭종 (simple bone cyst 또는 unicameral bone cyst) 은 주로 소아, 청소년기에 발견되는 비교적 흔한 질환으로, 상완골의 근위부 및 대퇴골 근위부등의 골간단에서 가장 많이 발생한다. 낭종의 크기가 큰 경우 골간단에서 성장판의 반대방향으로 진행하여 골간까 지 침벙하는 양상을 보이며, 성장판을 침범하는 경우는 보고가 드물다. 저자들은 11세 여아 에서 상완골 성장판을 지나 골단까지 침범한 고립성 골낭종의 단순 촬영 및 자기공명영상 소견을 보고하고자 한다.
고립성 골낭종(simple bone cyst 또는 unicameral bone cyst)은 낭종성 질환중 가장 흔한 질환으로 정확한 발생 기전 은 알려져 있지 않고, 남아에서 여아보다 2-3배 더 많이 발생 된다(1). 고립성 골낭종의 골단 침범은 1942년 Jaffe 등(2) 이 최초로 보고한 이후 매우 드풀게 보고되고 있다.
증례보고
11세 여아가외상없이 발생한우상완동통으로내원하여 단 순 견관절 촬영을 시챙하였다. 우상완골의 근위부에 비교적 경 계가 좋은 낭종성 병변이 관찰되였으며 이 병변은 아직 융합되 지 않은 성장판을 지나 골단까지 침범하였다. 낭종의 근위부,
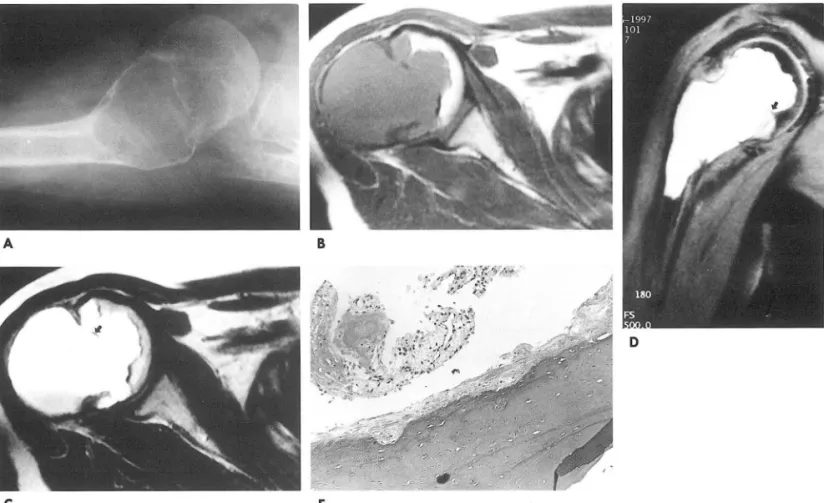
즉 콜단내에 있는 부분은 비교적 앓은 경화성 테에 의하여 주위 와 잘 구분되었고 분엽상을 보였다. 골간단에 위치한 낭종의 원 위부에서는 경화성 테두리는 보이지 않았으나 경계는 분명하였 고, 팽창하고 있는 골 피질의 병적 골절이나 낭종 내부의 중격 은 없었다 (Fig.1A).
자기공명영상에서 낭종은 Tl 강조영상 및 T2 강조영상에서 모두 저신호강도의 테를 보였으며 주변 골수의 신호강도는 정 상이었다. 냥종의 내용물은 Tl 강조영상에서는 중간신호강도 를 보이는 하층과 더 낮은 신호강도의 상층으로 나뉘어 있었고
T2 강조영상에서는 이들은 각각 고신호강도의 상층, 중간신호 강도의 하층으로 구분되어 출혈을 시사동}는 소견으로 보였다 (Fig. lB, lC). 낭종내의 중격은 보이지 않았으며 낭종내에서 일부 남아있는 성장판으로 생각되는 저신호강도의 부분만이 있 었다 (Fig. lB, lC, 1D). 조영증강후 실시한 지방포화 영상에서 낭종의 변연부에 불규칙한 연속적 조영증강을 보였으나 낭종의
l 경희대학교 의과대학 진단방사선과학 교실 z경희대학교의과대학 해부병리학교실
’경희대학교 의과대학 정형외과학교실
이 논푼은 1998년 4 월 6일 접수하여 1998년 6월 1일에 채택되였음.
내용물이나 주변 골수에는 조영증강되는 부분이 없었다.
환자는 소파술과 골이식술을 시행하였고 조직 소견상 여러층 의 섬유세포 및 섬유아세포와 혈관들로 구성된 냥종의 태가 약 간의 응고된 혈액과 함께 보였으며 섬유아세포의 낭종벽 조직 으로 고립성 골냥종임을 진단할 수 있었다 (Fig. 1E).
고 찰
고립성 골냥종은 골발달중인 장골의 골간단에서 발생하는 양 성 질환으로 대부분의 경우 성장판에 인접한 골간단에서 발생 하여 골간을 향하여 커진다(1). 남아에서 여아보다 2-3배 호 발하고 가장 호발하는 부분은 근위 상완골(55%) 이며 그 다음 으로 근위 대퇴골(26%) , 경골등이다(1 ). 고럽성 낭종의 발생 기전은 정확히 밝혀지지 않았으며 드물게 성인에서도 보고되고 있으나 이러한 경우는 상기 호발부위가 아닌 장골이나 요골, 늑 골등에서 보고되기도한다.
1942년 Jaffe 등(2) 이 고럽성 냥종의 골단 침범을 최초로 보 고한 이후로 골단 침범에 관한 증례보고가 드물게 있었다.
Malawer 등 (3) 의 증례보고 및 문헌 고찰에서 골단을 침범한 고립성 골낭종은 근위 대퇴골에 3예, 근위 상완골에 2예, 근위 경골에 2예 및 원위 대퇴골에 1예로 일반적인 고립성 골낭종이 상완골에서 호발하는것과는달리 대퇴골에서 골단을침벙하는 빈도가 높았다고 하였다.
일반적으로 골간단의 고립성 골낭종에서는 골절이 동반되지 않으면 침벙된 사지의 성장 장애는 거의 없다. 성장판을 지나 골단을 침벙한 고립성 골낭종의 경우에도, 침범된 사지의 길이 성장이 저해되는 경우는 많지 않다고 보고되어 있으며 (3, 4), Capanna 등 (4) 에 의한 보고에서는 골단에 고립성 골냥종이 있 었던 10예중 4예에서 성장 장애가 있였다고 하였으나 이들중 1
예는 병적 골절이 동반되어 있어 고립성 낭종의 성장판 침벙에
m m
의한 성장 장애인지 골절에 의한 성장 장애인지 분명하지 않다 고 하였다 본 증례에서는 병력상 뚜렷한 양측 상완의 차이는 보이지 않았으나 경과 추적이 필요할 것으로 보인다.
치료에 있어서, 성장판을 침범한 경우 소파술이나 steroid 치 료를 많이 시행하는데, Campanacci 등 (5) 은 고립성 골낭종의 성장판 침범이 있는 경우, 약 50% 에서 재발 없이 완전히 치유 된다고 보고하고 있다. 이는 성장판에 근접한 고립성 골낭종에
서의 steroid 치료가 50% 정도의 완치를 보이는 것과 비슷한
치료율이다.
고립성 골낭종이 골단을 침범한 경우, 진단이 어려운 경우가 있는데 소아나 청소년기에 흔히 골단에서 관찰되는 동맥류성 골냥 (aneurysmal bone cyst) 이나 연골모세포종 (chondrob lastoma), 또는 거대세포종 (giant cell tumor) 등과의 감별이
C E
이범하 오1: 상완골 골단을 칠범한 고립성 골낭종의 밤사선학적 소견
필요하다. 골단에서 낭성 병변이 관찰될 때, 장골의 일측에 치 우쳐져서 위치하고골피질의 팽창이 심하며 내부의 중격이 더 많은 경우 동맥류성 냥종의 가능성이 높으나 (6) , 고립성 골낭 종에서 출혈을 동반한 경우 감멸이 용이하지 않다. 연골모세포 종은 10대에 많이 발생하며 골간단과 골단을 침범하는데, 30- 50% 에서는 석회화를 동반하고 있고 자기공명영상에서 출혈성 낭종을 동반할 수도 있으나, 대부분 연골조직에 의한 신호강도 를(Tl 강조영상에서 저신호강도, T2강조영상에서 고신호강 도) 보이는 부분들이 섞여 있다 (7). 거대세포종도 골단을 침범 하는 냥성 질환이나 20대에서 30대에 호말하묘로 소아에서는 드물고, 대퇴골, 경골, 요골순으로 발생하며, 일측 피질에 치우 쳐서 위치하는 팽창성 낭종으로 보이는 것으로 감멸할 수 있다 (8).
Fig. 1. A. Right shoulder axillary view shows a well defined osteolytic lesion with bulging contour and thin sclerotic rim on the metaphysis and epiphysis of the humerus.
B. Tl(TR/TE=660/12) weighted axial image of right humerus shows a lobulating cystic lesion with intermediate signal intensity on the proximal metaphysis and epiphysis. A faint f1uid-fluid level is seen within the cystic lesion, indicating hemorrhage within the cyst.
c.
T2(TR!r
E=3500/98) weighted image shows high signal intensity fluid on the upper portion of the cystic lesion with slightly low signal intensity on the lower portion, due to cellular components of the hemorrhage. Epiphyseal extension is also noted with lobulating, irregular margin. Remained physis is noted as a curved, low signal line within the cyst (arrow).D. Proton weighted fat saturated image shows lobulting high signal intensity cyst from the epiphysis to proximal meta physis. Remnant peripheral portion of growth plate protrude into the cyst(arrow).
E. Microscopic examination shows multiple layers of fibroblasts with small vessels ad jacent to the curetted bone chip (x 400, Hematoxylin-Eosin stain).
- 400 -
J Korean Radi이 Soc 1998; 39: 403-406
A
c
This case showed that accelerated growth on the left side of the body in early childhood caused severe cos- metic and functional orthopaedic problems.
Macrodactyly is one of the more striking manifesta- tions of Proteus syndrome, involving true gigantism of any combination of digits in the hands, feet or both.
Stricker (2) stated that 54 of 61 patients showed macrodactyly of at least one hand or foot and that enlarged digits were not always located on the side of hemih ypertroph y.
Hemangioma, lymphangioma, fibroma, osteoma, osteochondroma and enchondroma have been de- scribed in Proteus syndrome(3, 5). The presence of hemangiomatosis and enchondromatosis in a few cases has led to a misdiagnosis of Maffucci’s syndrome(3, 5).
Wiedemann et a1. (1) noted that visceral abnormali- ties were a possible major feature ofProteus syndrome, while Eberhard (6) reported various abno야orma s있ubmucosa려1 vascular ma떠lformations in the colon, rec tum and urinary bladder ; a renal cavernous hemangi- oma; mesenteric lipomatosis; multiple cavernous hem- angiomas in the subcutaneous tissues, stomach, spleen and spermatic cord ; a mixed mesenchymal-bronchial
% B
Fig. 3. A and B. Tl W and T 2W sagittal images of the left foot and ankle show irregular round periarticular mixed signal in- tensity mass with peripherallow and central irregular high signal intensity in the left first metatarsophalangeal joint (thin arrow). and low signal intensity gyriform hyperplasia ofthe plantar surface ofskin(thick arrow).
C. Fat suppression Tl W sagittal image shows heterogenous low signal intensity ofperiarticular mass in the greater toe.
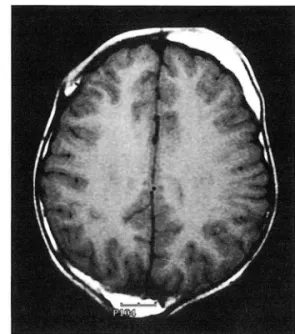
Fig. 4. TlνV axial brain MRI shows multiple skull bossings with widening and fat deposition of the diploic space and bulging ofthe outer table
hamartoma of the lung; cystiform lung lesion and se- rous ovarian cysts. It seems likely that visceral ham- artomatas are common in Proteus syndrome but may often be asymptomatic.
Viljoen DL et a1. (7) have emphasized that thicken- ing and gyrifrom skin hypertrophy in the palms and soles are a striking finding. Subcutaneous tumors are common and histologically represent lipomata, lymphangiomata, hemangiomata or a combination of these hamartoses. This patient had histologically prov- en fibromatosis in the sole.
Fig. 5. Abdominal CT reveals asymmetrical marked fat depositon in the abdominal wall and splenomegaly
Spinal deformity frequently develops in Proteus syndrome, and may include vertebral dysplasia with irregular and d ystrophic intervertebral disc and localiz- ed enlargement of the vertebrae ; “megalospond ylod ysplasia" was the term used by Stagnara and Fauchet (S). Scoliotic deformity ranges from mild to severe(l, S)
; this patient had megalospondylodysplasia in the cer- vical, thoracic and lumbar spine, with mild scoliosis of the last named.
Cranial anomalies are the least common major manifestation of this syndrome. Skull vault bossing seems to consist of congenital protuberances due to localized diploic thickening, rather than calcified hematomas(S). Skull vault bossing due to increased diploic fat was seen on postmortem examination in the patient reported by Haberland and Perou(8); this pres- ent case represented fat accumulation in the diploic space, with bulging of the outer table on MRI; there were no other brain abnormalities
Rare minor abnormalities in Proteus syndrome in- clude congenital cervical fusion, micrognathia, genito- urinary anomalies, dental anomalies, tonsillar hypert- rophy, congenital cardiac anomalies and conduction
Seon-Young Yoo : Proteus Syndrome
defects(2). This patient had dental anomalies.
In many hamartomatous conditions, malignancy is more frequent; mesothelioma ofthe tunica vaginalis of the testis has been reported in a child with Proteus syn- drome(9). Because of its variable phenotype and the fact that it shares many comrnon features with other hamartoses and phacomatoses. Proteus syndrome may be difficult to recognize. The disorder must be dis- tinguished from Klippel- Trenaunay-Weber, Bannay- an-Zonana, Sturge-Weber, Maffucci, and encephal- ocraniocutaneous syndromes, and from neurofibrom- atosis. Many reported cases ofProteus syndrome were initially misdiagnosed.
In conclusion, Proteus syndrome is characterized by multifocal overgrowth involving various parts of the body. MRI is useful for delineating the nature and extent ofhamartomatous lesions arising from it.
References
l. Wiedemann HR, Burgio GR, Aldenhoff P, Kunze ι Kaufmann HJ and Schirg E. The Proteus sy ndrome. Eur J Pediatr 1983;
140: 5-12
2. Stricker S. Musculoskeletal manifestation of Proteus syndrome Report of two cases with Iiterature review. J Pediatr Orthop 1992; 12: 667-674
3. Hotamisligil GS. Proteus syndrome and hamartoses with over- growth. Dysmorphol Clin Genet 1990; 4: 87-102
4. Samlaska CP, Levin SW, James WD et al. Proteus syndrome
Arch Dermatol 1989; 125: 1109-1114
5. Arouz EM, Costa T, Fitch N. Radiologic findings in the Proteus syndrome. Pediatr Radiol 1987; 17: 481-485
6. Eberhard DA. Two-year old boy with Proteus syndrome and fatal p비 monary thromboembolism. Pediatr Pathol 1994; 14 771-779
7. Viljoen DL. Nelson MM, de Jong G, Beighton P. Proteus syn- drome in Southern Africa: Natllral history and c1\nical manifes- tations in six individuals. Am J Med Genet 1987; 17: 87-97 8. Haberland C. Peroll M. Encephalocranioclltaneous lipomatosis
Arch Neurol 1970; 22: 144-155
9. Malamitsi-Pucher A, Dimitriadis D, Bartsocas C. Wiedemann HR. Protells syndrome: COllrse of a severe cases. Am J Med Gen et 1990; 35: 283-285
대한밤시선의학회지 1998; 39: 403-406
Proteus 증후군 1 예 보고1
l 한국보훈병원 방사선과 유 선 영
Proteus 증후군은 태생기 삼배엽에 비정상적인 이형성증이 나타나는 선천적인 질환으로 신체 일부분의 과성
장, 편측 비대증, 색소성 피부질환, 연부조직 종양, 두개골 이상, 외골종 및 기타 신체 기형을 특정으로 한다. 저 자는 12세된 남아에서 전형적인 Proteus 증후군 l 예를 경험하였기에 진단에 유용한 전산화단층 촬영소견 빛 자 기공명 촬영소견을 보고하고자 한다.
- 406 -