101
서 론
분화된 갑상선암은 완치율이 매우 높은 질환으로, 기본 적인 수술적 치료와 방사성요오드 치료만으로 10년 이상의 장기 생존율을 보인다.(1-3) 갑상선암의 기관식도 침범은 1∼7%의 발생률로 매우 드물게 나타나며,(4) 환자의 나이, 원격전이 여부, 치료 전 종양의 크기나 종양의 완전 제거 여부와 함께 생존율에 있어 나쁜 예후 인자이다.(1,5) 갑상 선암이 기관이나 식도를 침범한 경우에는 그 침습 정도에 따른 특이 증상이 발생하기도 하며, 사망률 증가의 원인이 되기도 한다. 애성, 협착음이나 호흡곤란 등이 종괴의 직접 적인 기도내강 침범으로 인한 기도협착에 의하거나 반회후 두신경 침범으로 인한 후두근 마비에 의해서 나타난다. 또 한 객혈이 종괴의 기도내강 침범과 미란의 결과로 나타난 다.(6) 또한 갑상선암을 대상으로 한 여러 연구에서 알 수 있듯이, 이러한 국소침습은 많은 환자들에서 직접적인 사 인이 되기도 한다. Tollefson등(5)의 연구에서는 47%의 환자 에서 국소침습과 관련된 기도출혈과 질식이 직접적인 사인이 었다. McConahey등(1,2)의 또 다른 연구에서는 질병의 국소 적인 제거의 실패로 사망한 환자와 원격전이로 사망한 환 자의 수가 비슷하다고 보고하고 있고, 이는 질병의 철저한 국소 제거가 환자의 사망률과 유병률을 낮추는 데 중요하 다는 것을 보여준다. 그러나 아직까지 수술의 범위에 대해 서는 논란의 여지가 있다.
이 논문에서는 기관식도를 침범한 침습적인 분화 갑상선 암의 임상양상과 치료 결과를 분석하여, 침습성 갑상선암의 치료에 있어서 국소 제어의 방법에 대해 논의해 보고자 한다.
방 법
1989년 7월부터 2002년 7월까지 서울대학교병원 이비인 후과에서 기관식도를 침범한 분화 갑상선암으로 치료 받은
기관식도 침범이 있는 분화 갑상선암의 치료
서울대학교 의과대학 이비인후과학교실
하정훈․정은정․노동환․권성근․성명훈․김광현
Treatment of Well-differentiated Thyroid Carci- noma with Aerodigestive Tract Invasion
Jeong-Hun Hah, M.D., Eun-jung Jung, M.D., Dong Hwan Roh, M.D., Seong Keun Kwon, M.D., Myung-Whun Sung, M.D. and Kwang Hyun Kim, M.D.
Purpose: Well differentiated thyroid carcinomas are mostly curable diseases. Invasion of aerodigestive tract by thyroid carcinoma is rare. However, it is considered as a poor prog- nostic indicator of survival. Some studies showed that local invasion of thyroid carcinoma was the cause of death in many patients. Therefore, adequate local control of the tumor is critical to avoid the mortality as well as the morbidity of the disease. To find proper and adequate treatment modality of locally invasive thyroid carcinoma, we evaluated treatment modalities and outcomes in the patients with thyroid carci- noma with invasion of aerodigestive tract.
Methods: Forty patients with thyroid carcinoma invading aerodigestive tract who were treated from July 1989 through July 2002 were reviewed retrospectively.
Results: Direct intraluminal invasion of the thyroid carcinoma requires definitive resection of the aerodigestive tract. In case that the extent of tumor was thought to be limited to perichon- drium or extraluminal invasion, tracheal shaving procedure was performed. Five-year and 10-year local control rates were 81.6%
and 57.4%, respectively. Disease-specific survival rates of 5-year and 10-year were 90.1% and 81.1%, respectively.
Conclusion: For the successful treatment of invasive thyroid carcinoma, the resection of the functional structures or the aerodigestive tract should be determined prudently according to the presence of the intraluminal invasion. (Korean J Endocrine Surg 2004;4:101-105)
Key Words: Thyroid carcinoma, Aerodigestive tract invasion 중심 단어: 갑상선암, 기관식도 침범
책임저자:김광현, 서울시 종로구 연건동 28번지
ꂕ 110-744, 서울대학교 의과대학 이비인후과학교실 Tel: 02-2072-2448, Fax: 02-745-2387
E-mail: [email protected] 게재승인일:2004년 12월 14일
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Department of Otorhinolaryngology-Head and Neck Surgery,
Seoul National University College of Medicine, Seoul, Korea
40명의 환자를 대상으로 후향적으로 연구하였다. 초기 진 단이 역형성 갑상선암인 경우는 제외하였고, 이번 연구에 포함된 환자들의 조직형은 모두 유두상 갑상선암이었다.
여성이 29예였고 남성이 11예였다. 환자들의 나이는 25세
에서 78세로 평균 나이는 60세였다. 추적관찰기간은 7개월 에서 175개월로 평균 77개월이었다. 갑상선암의 기관식도 침범을 진단 받고 치료받기 이전에 갑상선암에 대한 수술 을 시행 받았던 병력이 있는 환자는 40명 중 23명(57.5%)이 었다. 23명 가운데 갑상선전절제술을 시행 받은 경우는 8예 였고, 나머지 15예는 갑상선아전절제술 혹은 갑상선부분절 제술을 시행 받았다.
증상과 징후, 수술적 접근방법, 합병증 등의 여러 가지 임 상적 지표들을 분석하였고, 수술적 치료방법을 기준으로 환자군을 분리한 후 그 결과를 분석하였다. 생존율과 국소 재발률의 산출은 Kaplan-Meier 방법을 이용하였다.
결 과
환자들에서 나타난 가장 흔한 특이 증상은 애성으로 21
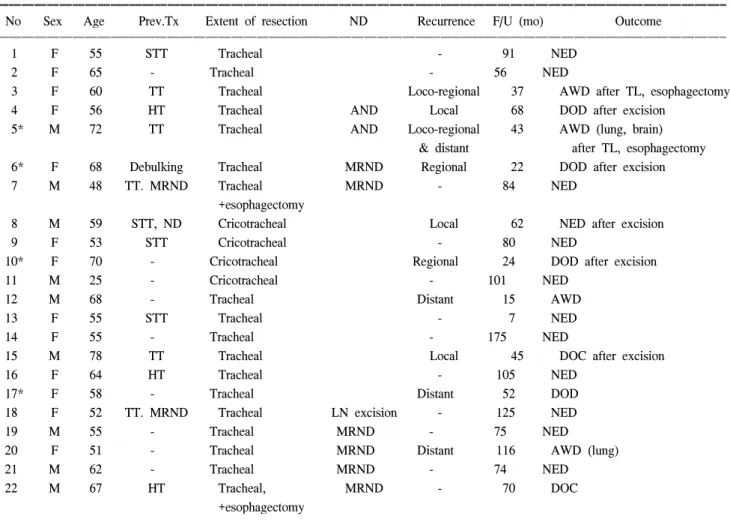
Table 2. Clinical outcome of the patients after tracheal resection (n=22)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
No Sex Age Prev.Tx Extent of resection ND Recurrence F/U (mo) Outcome
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
1 F 55 STT Tracheal - 91 NED
2 F 65 - Tracheal - 56 NED
3 F 60 TT Tracheal Loco-regional 37 AWD after TL, esophagectomy
4 F 56 HT Tracheal AND Local 68 DOD after excision
5* M 72 TT Tracheal AND Loco-regional 43 AWD (lung, brain)
& distant after TL, esophagectomy
6* F 68 Debulking Tracheal MRND Regional 22 DOD after excision
7 M 48 TT. MRND Tracheal MRND - 84 NED
+esophagectomy
8 M 59 STT, ND Cricotracheal Local 62 NED after excision
9 F 53 STT Cricotracheal - 80 NED
10* F 70 - Cricotracheal Regional 24 DOD after excision
11 M 25 - Cricotracheal - 101 NED
12 M 68 - Tracheal Distant 15 AWD
13 F 55 STT Tracheal - 7 NED
14 F 55 - Tracheal - 175 NED
15 M 78 TT Tracheal Local 45 DOC after excision
16 F 64 HT Tracheal - 105 NED
17* F 58 - Tracheal Distant 52 DOD
18 F 52 TT. MRND Tracheal LN excision - 125 NED
19 M 55 - Tracheal MRND - 75 NED
20 F 51 - Tracheal MRND Distant 116 AWD (lung)
21 M 62 - Tracheal MRND - 74 NED
22 M 67 HT Tracheal, MRND - 70 DOC
+esophagectomy
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
* = cases of anaplastic transformation; HT = hemithyroidectomy; ND = neck dissection; MRND = modified radical neck dissection; AND
= anterior neck dissection; LN = lymph node; NED = no evidence of disease; AWD = alive with disease; DOD = die of disease; DOC
= die of other cause; TL = total alryngectomy.
Table 1. Symptoms of the thyroid cancers invading aerodigestive tract
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ No. of patients (n=40)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Hoarseness 21 (52.5%)
Dyspnea 16 (40.0%)
Palpable neck mass 10 (25.0%)
Stridor 10 (25.0%)
Hemoptysis 3 (7.5%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Numbers are not mutually exclusive.
예(52.5%)에서 나타났고, 다음으로 호흡곤란 16예(40.0%), 협착음 10예(25.0%), 경부 종괴 10예(25.0%), 객혈 3예(7.5%) 의 순이었다(Table 1).
이학적 검진상 27예(67.5%)에서 경부 종괴가 촉진되었고, 27예(67.5%)에서 성대마비가 관찰되었다. 3예(7.5%)에서는 국소침습 진단 당시 폐의 원격전이가 발견되었는데, 그 중 1예에서는 뇌전이가 동시에 발견되었다.
1) 수술방법 및 임상경과
수술 전 전산화단층촬영과 내시경적 검사를 통해 종양의 침습범위를 확인하고 이에 따라 수술방법을 결정하였다.
전산화단층촬영에서 종양의 침습범위가 연골 외막은 침범 하였으나 내강은 침범하지 않은 경우에는 면도식 기관절제 술(tracheal shaving operation)을 시행하였다. 반면에 종양이 윤상연골이나 갑상연골을 깊게 침범하고 있고 기도협착을
유발한 경우에는 후두전적출술(total laryngectomy)을 시행 했고, 후두를 침범하지는 않았으나 기관연골을 깊게 침범 하고 있는 경우에 기관절제 후 단단문합술(tracheal resection and end-to-end anastomosis)을 시행하였다.
기관절제 후 단단문합술, 후두전적출술, 면도식 기관절제 술이 각각 22예, 9예, 8예에서 시행되었다. 나머지 1예에서 는 갑상선전절제술과 함께 면도식 식도절제술(esophageal shaving operation)이 시행되었다.
기관절제 후 단단문합술은 22명의 환자에서 시행하였다.
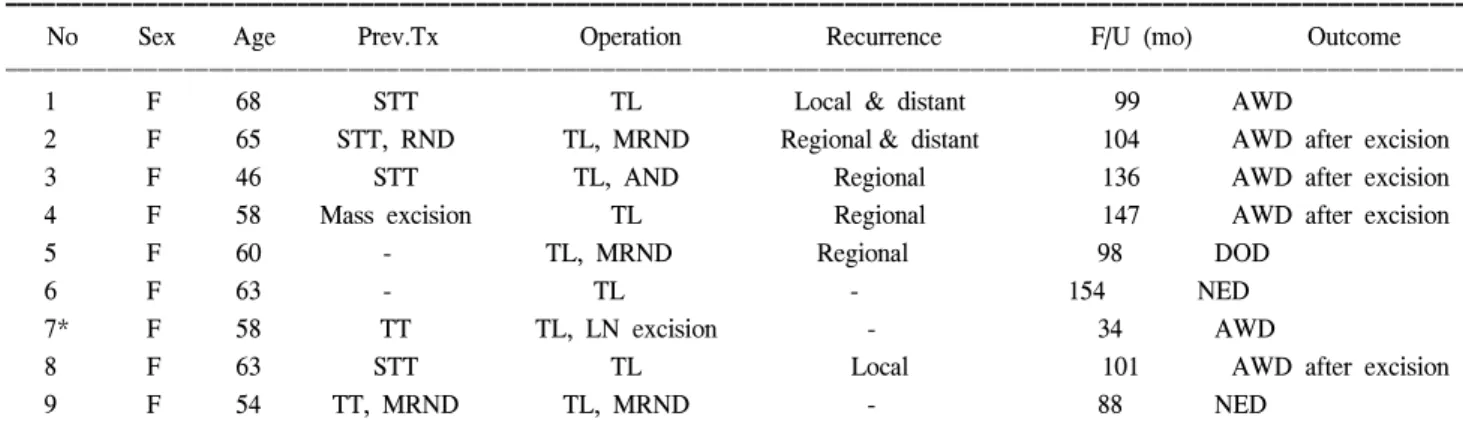
14명은 갑상선암으로 수술 받은 병력이 있었으나, 나머지 8명은 초치료로서 시행되었다. 16예(72.7%)에서 수술 전 성 대마비가 관찰되었다. 수술 후 11예에서 재발하였는데, 국 소(local) 재발 3예, 국소 및 부위림프절(loco-regional) 재발 2예로 국소 치료 실패는 22예 중 5예(22.7%)였다. 국소 재발 한 환자 가운데 2예에서는 국소 구제수술로서 후두전적출 Table 3. Clinical outcome of the patients after total laryngectomy (n=9)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
No Sex Age Prev.Tx Operation Recurrence F/U (mo) Outcome
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
1 F 68 STT TL Local & distant 99 AWD
2 F 65 STT, RND TL, MRND Regional & distant 104 AWD after excision
3 F 46 STT TL, AND Regional 136 AWD after excision
4 F 58 Mass excision TL Regional 147 AWD after excision
5 F 60 - TL, MRND Regional 98 DOD
6 F 63 - TL - 154 NED
7* F 58 TT TL, LN excision - 34 AWD
8 F 63 STT TL Local 101 AWD after excision
9 F 54 TT, MRND TL, MRND - 88 NED
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
* = Presence of lung metastasis at the time of initial diagnosis; STT = subtotal thyroidectomy; TT = total thyroidectomy; TL = total laryngectomy; RND = radical neck dissection; MRND = modified radical neck dissection; LN = lymph node; AWD = alive with disease;
DOD = die of disease; NED = no evidence of disease; Mets = metastasis.
Table 4. Clinical outcome of the patients after tracheal shaving operation (n=8)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
No Sex Age Prev.Tx Operation Recurrence F/U(mo) Outcome
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
1 F 53 - TT, Shaving - 22 NED
2 F 50 Lobectomy TT, Shaving - 84 NED
3 F 52 - TT c Shaving, AND - 91 NED
4 F 72 - TT, Shaving - 13 NED
5 M 62 - TT, Shaving Local 156 NED after TREE, MRND
6 F 61 - TT, Shaving - 28 NED
7 F 56 Lobectomy TT, Shaving Loco-regional 105 NED after TREE,
(trachea & esophagus) esophagectomy & LN excision
8 F 77 - TT, Shaving - 15 NED
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ TT = total thyroidectomy; AND = anterior neck dissection; NED = no evidence of disease; MRND = modified radical neck dissection;
TREE = tracheal resection and end-to-end anastomosis.
술과 식도절제술을 동시에 시행하였으며, 모두 잔존암을 가진 상태로 추적 관찰 중이다(Table 2).
후두전적출술을 시행 받은 환자는 9명이었는데, 이 중 7명은 이전의 갑상선전절제술 혹은 갑상선아전절제술을 시행 받은 병력이 있었고, 5명은 진단 당시 성대 마비가 있 었다. 후두전적출술 시행 후 7예에서 종양의 재발이 있었으 며, 이 가운데 2예는 국소 재발을 동반하여, 국소 치료 실패 율은 28.6%였다. 재발한 종괴에 대한 종양 절제 및 경부곽청 술 이후에 사망한 1예를 제외하고 추적관찰 중이다(Table 3).
기관의 면도식절제술을 시행 받은 환자는 8명이었고, 이 중 6명(75.0%)에서 수술 전 성대마비가 관찰되었다. 1예에 서는 수술 71개월 후 객혈을 동반한 경부종괴를 주소로 하 는 국소재발을 보였고, 기관절제 후 단단문합술 및 경부곽 청술을 시행하였다. 또 1예의 환자는 술 후 8년이 지나서 국소재발이 발견되어 식도절제술 및 종괴제거수술 이후 현 재 8개월째 추적관찰 중이다. 이 외의 환자에서는 국소재발 이나 원격전이가 발생하지 않았고, 현재 모두 무병상태로 추적관찰 중이다(Table 4).
전체적으로, 40명의 환자 중 9명에서 국소 재발하여 5년 국소 제어율은 81.6%, 10년 국소 제어율은 57.4%였다(Fig. 1).
부위림프절 재발과 원격 재발을 포함하면 40명 중 18명에 서 재발하여, 전체 종양 제어율은 5년 64.5%, 10년 38.3%였다.
구제 수술로서 식도에 대한 수술을 받은 경우는 5예 있었 는데, 기관절제나 후두전적출술과 함께 면도식 기관절제술 을 시행하거나 식도절제술을 시행한 경우였다. 1예에서는 종양의 광범위한 식도침범으로 인해 후두식도적출술 후 공 장 유리피판을 이용한 재건술이 시행되었는데, 병리소견상 역형성 갑상선암이 부분적으로 발견되었고 환자는 수술 당 시 폐와 뇌전이가 발견된 상태였으며 수술 13개월 뒤에 뇌 전이로 인해 사망하였다.
갑상선암에 의한 사망 예는 모두 5예였는데, 이 중 3예가 경과 도중 갑상선 유두상암종에서 역분화 소견을 보인 경 우였다. 앞서 언급한 뇌전이로 사망한 1예를 제외한 다른 2예는 질환의 진행과 척추와 폐로의 다발성 원격전이로 사 망하였다. 대상 환자 40명 전체의 질병 특이 생존율은 5년 90.1%, 10년 81.1%였다(Fig. 2).
2) 합병증
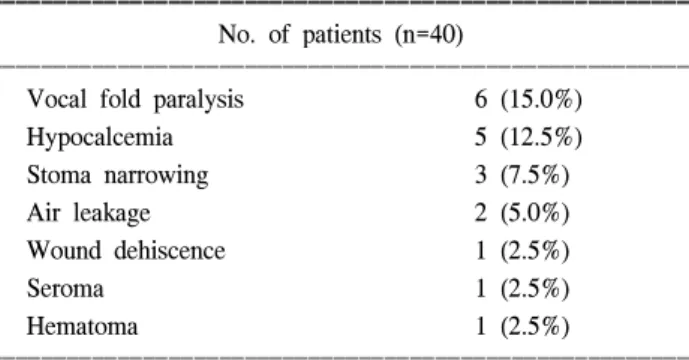
수술 후 성대마비가 6예(15%)에서 발생하였고, 이들 모 두는 기관절제 후 단단문합술을 시행 받은 경우였다. 양측 성대마비로 영구기관절개술을 시행 받은 환자가 3예였는 데 이들은 모두 수술 전 일측 성대마비가 있던 경우였다.
영구적인 저칼슘혈증은 5예(12.5%)에서 발생하였다. 기관 절제 후 단단문합술 시행 후 창상 치유 지연과 창상 열개로 대흉근피판을 이용한 창상재건이 필요한 경우가 1예 있었 지만, 모든 환자에서 생명을 위협할 만한 중대한 합병증은 발생하지 않았다(Table 5).
Fig. 1. Local control rate in 40 patients with thyroid cancer in- vading aerodigestive tract (Kaplan-Meier Method). Five- year and 10-year local control rates were 81.6% and 57.4%, respectively.
Fig. 2. Disease-specific survival curve in 40 patients with thyroid cancer invading aerodigestive tract (Kaplan-Meier Method).
Five-year and 10-year disease-specific survival rates were 90.1% and 81.1%, respectively.
Table 5. Complications after surgical treatment of thyroid cancers invading aerodigestive tract
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ No. of patients (n=40)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Vocal fold paralysis 6 (15.0%)
Hypocalcemia 5 (12.5%)
Stoma narrowing 3 (7.5%)
Air leakage 2 (5.0%)
Wound dehiscence 1 (2.5%)
Seroma 1 (2.5%)
Hematoma 1 (2.5%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
고 찰
기관식도를 침범한 갑상선암의 절제 범위 결정에는 논란 의 여지가 있다. 절제 범위는 종양의 치료 가능성, 생존율, 기능적 이환율 사이의 균형에 의해 결정되어야 한다. 박등8) 은 기관에 국한된 침습을 보이는 16예의 갑상선암 환자에 서 면도식 절제술과 추가 방사선치료를 시행하였는데, 12 예에서 재발하였고, 이중 7예의 환자에서 결국 재발로 인해 사망하였다고 보고하였다. Fujimoto등(9)과 Grillo등(10)의 연구에서도, 종양이 침범된 모든 구조물의 적극적인 광범 위 절제술은 종양의 기도 내강 내 침범여부에 관계없이 갑 상선암의 국소 재발률을 낮추고 환자의 이환율 및 사망률 을 낮춘다고 보고하였다. 그러나 Czaja와 McCaffrey(11)는 침습적 고분화 갑상선암의 치료에 있어서 292명의 환자를 대상으로 한 조사에서 면도식 절제술과 완전한 절제술 사 이에 생존율의 차이가 없다고 보고하였다.
이번 연구에서 저자들은 병변의 침범 범위에 따라 수술 의 범위를 결정하는 방법을 사용하여 좋은 국소 치료 결과 를 얻었으며, 전체 환자군에서 81.1%의 높은 10년 생존율을 얻을 수 있었다. 무작위 대조군 연구가 아니라는 한계가 있 지만, 선별된 환자에서 면도식 절제술만으로도 좋은 국소 제어 효과가 있었다. 기관식도를 침범한 갑상선암을 치료 함에 있어서, 컴퓨터 단층촬영이나 내시경 소견에서 기도 내강으로의 명확한 침범이 없는 경우, 육안적으로 관찰되 는 병변에 대한 면도식 절제술 등의 보존적인 수술을 시행 하는 것이 질병의 국소치료 효과나 환자의 기능적인 면을 고려했을 때 일차적으로 고려되어야 할 것으로 판단된다.
결 론
결론적으로, 기관과 식도에 대한 침습을 보이는 갑상선 암의 치료에 있어서 국소 치료가 매우 중요하지만, 선별된 환자에서는 면도식 절제술 같은 보존적인 수술을 시행하는 것이 기능을 보존하면서 높은 국소 제어율을 보이는 효과 적인 치료 방법이었다.
REFERENCES
1) McConahey WM, Hay ID, Woolner LB, Van Heerden JA, Taylor WF. Papillary Thyroid Cancer Treated at the Mayo Clin- ic, 1946 through 1970: initial manifestations, pathologic find- ings, therapy and outcome. Mayo Clinic Proc 1986;61:978-96.
2) Clark RL, Ibanez ML, White EC. What constitutes an adequate operation for carcinoma of the thyroid? Arch Surg 1966;92:23-6.
3) Hay ID. Papillary thyroid carcinoma. Endocrinol Metab Clin North Am 1990;19:545-76.
4) Andersen PE, Kinsella J, Loree TR, Shaha AR, Shah JP. Dif- ferentiated carcinoma of the thyroid with extrathyroidal extension. Am J Surg 1995;170:467-70.
5) Tollefson H, DeCosse J, Hutter R. Papillary carcinoma of the thyroid: a clinical and pathological study of 70 fatal cases.
Cancer 1964;17:1035-44.
6) MaCaffrey TV, Lipton RJ. Thyroid carcinoma invading the upper aerodigestive system. Laryngoscope 1990;100:824-36.
7) Vassilopoulou-Sellin R, Schultz PN, Haynie TP. Clinical outco- me of patients with papillary thyroid carcinoma who have recur- rence after initial radioactive iodine therapy. Cancer 1996;
78:493-501.
8) Park CS, Suh KW, Min JS. Cartilage-shaving procedure for the control of tracheal cartilage invasion by thyroid carcinoma.
Head Neck 1993;15:289-91.
9) Fujimoto Y, Obara T, Ito Y. Aggressive surgical approach for locally invasive papillary carcinoma of the thyroid in patients over forty-five years of age. Surgery 1986;100:1098-107.
10) Grillo HC, Suen HC, Mathisen DJ. Resectional management of thyroid carcinoma invading the airway. Ann Thorac Surg 1992;54:3-10.
11) Czaja JM, McCaffrey TV. The surgical management of laryngo- tracheal invasion by well-differentiated papillary thyroid carci- noma. Arch Otolaryngol Head Neck Surg 1997;123:484-90.
12) Bayles SW, Kingdom TT, Carlson GW. Management of thyroid carcinoma invading the aerodigestive tract. Laryngoscope 1998;108:1402-7.