서 론
만성폐쇄성폐질환(chronic obstructive pulmonary disease, 이하 COPD)은 만성염증에 의한 기도와 폐실질 손상으로 인 해 발생하며, 비가역적인 기류제한을 특징으로 한다. COPD 환자는 적절한 치료를 할 경우에도 폐 기능이 점차 저하되 므로, 정기적으로 추적 관찰하면서 치료 변경을 결정하는 것 이 필요하다.1)
원격의료는 원거리에 있는 환자에게 보건의료 서비스를 제 공할 목적으로 정보통신기술을 이용하여 임상 정보를 전송 하는 것을 의미한다.2,3) 최근 정보통신기술의 접근성 증가와
비용 감소로 원격의료가 관심을 받고 있으며, COPD 환자의 자가관리를 돕고 의료결과를 향상시킬 목적으로 원격의료 를 도입하는 것도 고려되고 있다. 이에 COPD의 관리에 사 용된 원격의료의 효과를 연구한 일차 연구뿐 아니라 체계적 문헌고찰 문헌2-14)도 다수 출판되어 있다. 하지만, 원격의료 는 포함내용 및 범위에 따라 다양한 종류의 중재가 있으며, 여러 연구에서 중재에 대한 조작적 정의가 다르다.
이에 본 연구에서는 COPD 관리를 위한 원격의료 중재의 일차 문헌에 대한 요약결과를 보고하는 체계적 문헌고찰을 개관하여 중재법의 세부 특성을 파악하는 것과 더불어 임상 적 효과, 경제적 효과 및 중재 적용 관련 영향에 대한 주요
An Overview of Systematic Reviews of Telehealth
Intervention for Chronic Obstructive Pulmonary Disease
Ah Ram Sul, Da Hyun Lyu, and Dong Ah Park
National Evidence-based Healthcare Collaborating Agency, Seoul, Korea
만성폐쇄성폐질환에서 원격의료 중재의 체계적 문헌고찰 개관
한국보건의료연구원
설아람·류다현·박동아
Received November 20, 2017 Revised November 29, 2017 Accepted December 8, 2017 Address for Correspondence:
Dong Ah Park
National Evidence-based Healthcare Collaborating Agency, 173 Toegye-ro, Jung-gu, Seoul 04554, Korea Tel: +82-2-2174-2771 Fax: +82-2-747-4918 E-mail: pda124@neca.re.kr
Objectives: The aim of this overview was to synthesize the current evidence of published system- atic reviews (SRs) addressing telehealth intervention for chronic obstructive pulmonary disease (COPD). Methods: We searched 3 databases (MEDLINE, EMBASE, and Cochrane Library) up to March 2016. By two authors independently, SRs were selected based on predefined inclusion crite- ria. Only English or Korean articles published after 2010 were selected. The outcomes of interest were clinical outcome (i.e., exacerbation events, dyspnea scale, health-related quality of life, mortal- ity, and healthcare utilization), associated costs and factors influencing the adoption of telehealth.
Narrative analysis was conducted. Results: Of the 147 articles, 13 SRs of telehealth met all inclu- sion criteria. Most of the control groups were offered usual care. Overall, there were no clinical vari- ables reported consistent improvements in telehealth group compared with control group. With re- gard to quality of life outcomes, it was found that telehealth group showed statistically significant improvement than control group. As a result of analyzing hospitalization and medical costs, the de- creasing tendency appeared in telehealth group compared with control group. In the studies explored factors affecting the adoption of telehealth, some barriers and facilitators in telehealth uptake were suggested. Conclusion: Possible beneficial effects were observed for telehealth of COPD patients in some of the outcomes. However, the detailed interventions differed between studies. This is an important area of research and further studies regarding impacts of telehealth for COPD manage- ment would be needed.
Key Words Chronic obstructive pulmonary disease · Telemedicine · Telemonitoring · Overview of systematic reviews.
J Health Tech Assess 2017;5(2):108-117 ISSN 2288-5811 Copyright © 2017 The Korean Association for Health Technology Assessment Original Article
JoHTA
결과를 검토하고자 하였다.
방 법
문헌 검색 데이터베이스로 Ovid-MEDLINE, Ovid-EM- BASE, Cochrane Library를 활용하였고, Scottish Intercol- legiate Guidelines Network(SIGN)의 Systematic reviews 검색필터를 사용하였다. 검색일은 Ovid 기반 데이터베이스의 경우 2016년 2월 29일이었고, Cochrane Library의 경우 2016 년 3월 9일이었다. 보충 검색을 위하여 본 연구 주제와 관련 된 문헌의 참고문헌을 토대로 수기검색도 병행하였다.
문헌 선택은 검색된 문헌을 2명의 연구자가 독립적으로 검 토한 뒤, 의견 일치를 통하여 최종 문헌을 선택하였다. COPD 환자를 대상으로 원격의료 중재의 임상적 효과, 경제적 효과 또는 중재 적용 관련 결과에 대해 연구한 이차 문헌을 선택 하였다. 2010년 이후에 출판된 체계적 문헌고찰 중 영어 또는 한국어 문헌을 선택하였으며, 초록만 발표되거나 동료심사 된 학술지에 게재되지 않은 문헌은 배제하였다. 1차 문헌선 택 과정은 문헌의 제목과 초록을, 2차 문헌선택 과정은 전문 (full-text)을 검토하여 선택/배제기준에 따라 적합한 문헌을 선정하였다.
자료추출은 문헌의 일반적 특성과 임상 결과(증상 악화, 건 강관련 삶의 질, 사망률, 의료이용 결과), 경제성 결과, 중재 적용 측면 결과로 분류하여 수행하였다. 이에 따른 결과를 서 술적으로 분석하였다.
결 과
체계적 문헌고찰 선정 결과
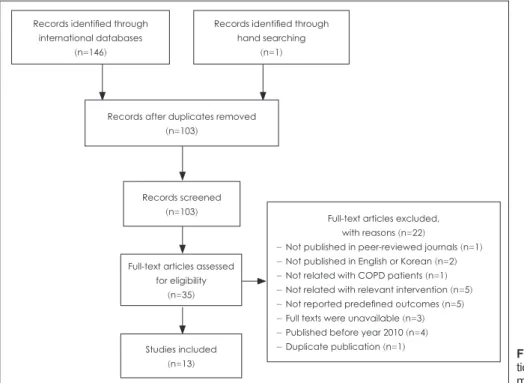
연구 주제에 부합하는 문헌은 데이터베이스 검색으로 146 편이 확인되었고, 수기 검색으로 1편2)이 추가되었다. 중복 검 색을 제거한 후 103편의 문헌 중 1차 선택/배제를 통해 35편 이 선택되었고, 2차 선택/배제를 통해 13편이 최종 선정되었 다. 문헌선정 흐름도는 그림 1과 같다.
선정된 체계적 문헌고찰에 대한 특성표는 표 1과 같다. 연 구 국가는 유럽이 9편(영국 4편, 스웨덴 1편, 이탈리아 1편, 포르투갈 1편, 덴마크 1편, 노르웨이 1편)으로 가장 많았고, 북미 3편(캐나다 2편, 미국 1편), 아시아 1편(일본)의 순이었다.
비교중재법의 경우 별도의 설명이 없이 대조군(control group) 으로 표현하기도 하였으나, 대개 일상 진료가 제공되었다고 보고하였다. 문헌에 무작위배정 비교임상연구(randomized controlled trial, 이하 RCT)만을 포함한 연구는 7편이었고, 그 외의 6편은 비무작위 연구(non-randomized controlled trial, 이하 NRCT)를 포함하였다.
명칭별로 분류 시 각 연구에 사용된 중재에 대한 조작적 정 의는 상이하였다(Appendix). 원격의료를 지칭하는 용어로는
‘telehealthcare,’3,13) ‘telehealth,’6,7,10,14) ‘telemedicine,’2,4,11)
‘telemonitoring,’5,12) ‘telenursing’9) 등이 대표적이었다. 이 외 에 리마인더 기능을 포함한 휴대전화 이용 중재를 보고한 1 편8)에서는 ‘mobile phone’ 또는 ‘cellular phone’라는 용어로 중재를 주로 표현하였다. 휴대전화 중재 외에는 모두 생체정
Fig. 1. Flow diagram of study selec- tion. COPD: chronic obstructive pul- monary disease.
Full-text articles excluded, with reasons (n=22)
- Not published in peer-reviewed journals (n=1) - Not published in English or Korean (n=2) - Not related with COPD patients (n=1) - Not related with relevant intervention (n=5) - Not reported predefined outcomes (n=5) - Full texts were unavailable (n=3) - Published before year 2010 (n=4) - Duplicate publication (n=1) Records identified through
hand searching (n=1) Records identified through
international databases (n=146)
Records after duplicates removed (n=103)
Records screened (n=103)
Full-text articles assessed for eligibility
(n=35)
Studies included (n=13)
보의 전송이 이루어졌다.
증상 악화-악화 사건 발생
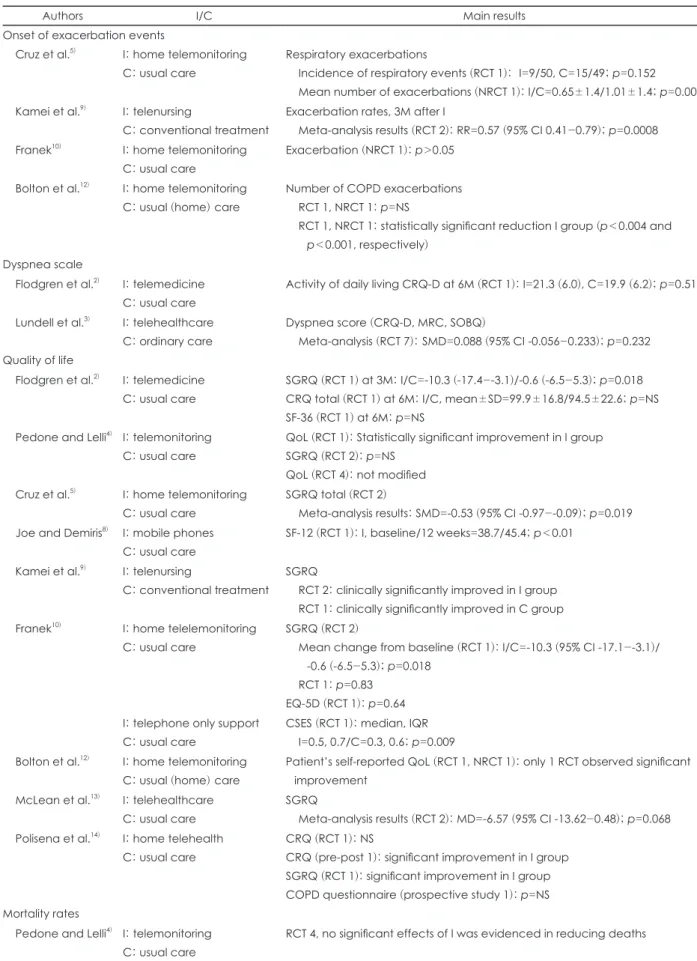
COPD 환자를 대상으로 원격의료 중재 시 증상 악화를 악 화 사건 발생 결과로 보고한 문헌은 4편5,9,10,12)이었다(표 2).
이 중 양적합성을 수행한 문헌은 1편9)이었다. RCT 2편을 메 타분석한 결과, 원격간호 중재 시행 3개월 후 원격간호군에 서 전통 관리군보다 악화율이 유의하게 낮았다(RR 0.57, 95% CI 0.41-0.79, p=0.0008).
나머지 3편 중 Cruz5)의 연구에서 가정 원격모니터링군과 일상 진료군의 호흡 사건 발생률(RCT 1)은 유의한 차이가 없었으나(각각 9/50 및 15/49, p=0.152), 평균 악화 횟수 (NRCT 1)는 원격모니터링군에서 유의하게 감소하였다고 보고하였다(각각 0.65회 및 1.01회, p=0.004). Franek10)의 연 구는 NRCT 1이 포함되었으며 가정 원격모니터링군과 일상 진료군 간에 악화는 유의한 차이가 나타나지 않았다.
Bolton12)의 연구에서 악화 횟수를 보고한 4편 중 2편(RCT 1, NRCT 1)에서 가정 원격모니터링군에서 일상 진료군보다 악화 횟수가 유의하게 감소한 것으로 나타났으나(각각 p
<0.004 및 p<0.001), 나머지 2편에서는 두 군 간 차이가 없 다고 보고하였다.
증상 악화-호흡곤란 점수
COPD 환자를 대상으로 원격의료 중재 시 증상 악화를 호 흡곤란 점수 결과로 보고한 문헌은 2편2,3)이었다(표 2). 호흡 곤란 점수 측정도구는 2편에서 모두 보고되었으며 Chronic Respiratory Questionnaire, Dyspnea subscale(CRQ-D), Medical Research Council(MRC) Dyspnea scale, Shortness of Breath Questionnaire(SOBQ) 등이 이용되었다.
양적합성은 1편3)에서 수행하였으며, RCT 7편을 메타분석 한 결과 원격보건 의료군과 일상 진료군 간에 호흡곤란 점 수는 유의한 효과가 나타나지 않았다. 다른 1편2)은 RCT 1편 을 포함하였으며, 원격 의료군과 일상 진료군 간에 일상생활 활동 시 호흡곤란 점수는 유의한 차이를 보고하지 않았다.
삶의 질
COPD 환자를 대상으로 원격의료 중재의 삶의 질 결과를 보고한 문헌은 9편2,4,5,8,9,12-14)이었으며(표 2), 1편12)을 제외하 면 모두 삶의 질 측정도구에 대해서 구체적인 언급이 있었다.
가장 많이 이용한 평가도구는 질병특이적 도구인 St George’s Respiratory Questionnaire(이하 SGRQ)이었으며, 임상적으 로 유의한 차이의 판단기준은 4점 이상의 향상이었다. 그 외 에 Chronic Respiratory Questionnaire(CRQ), Chinese Self- Table 1. Characteristics of the included systematic reviews AuthorsStudy countryInterventionComparatorSearch periodIncluded studies Flodgren et al.2) United KingdomTelemedicineUsual care-June 2013RCT 3* Lundell et al.3) SwedenTelehealthcareOrdinary care-August 30, 2013RCT 9 Pedone and Lelli4) ItalyTelemonitoringUsual careJanuary 2005-December 2014RCT 12 Cruz et al.5) PortugalHome telemonitoring Usual care-July 2013RCT 7, NRCT 2 Gorst et al.6) United KingdomHome telehealthUsual care-September 2013RCT 6, cohort 1, qualitative 4, mixed method 4† Udsen et al.7)DenmarkTelehealthUsual care (+education/Instructins)-August 2013RCT 6 Joe and Demiris8)United StatesMobile phonesUsual care1965-June 2012RCT 3* Kamei et al.9)JapanTelehome monitoring- based telenursingConventional treatment or care
-8 October 2011/ -third quarter of 2011 (CENTRAL
)RCT 5, NRCT 2 Franek10) CanadaHome telehealthUsual care1 January 2000-3 November 2010RCT 4, NRCT 2 Wootton11) NorwayTelemedicineUsual care-July/August 2011RCT 11* Bolton et al.12) United KingdomHome telemonitoringUsual
(home
) careJanuary 1990-July 2009RCT 2, NRCT 4 McLean et al.13)United KingdomTelehealthcareFace-to-face usual care-January 2010RCT 10 Polisena et al.14) CanadaHome telehealthUsual care1988-RCT 7, prospective study 1, quasi- experimental study 1, pre-post study 1 *Studies on COPD were counted, †Studies on COPD (+heart failure
) were counted.
CENTRAL
: Cochrane
Central Register of Controlled Trials, COPD
: chronic obstructive pulmonary disease, NRCT
: non-randomized controlled trial, RCT : randomized controlled trial
Table 2. Results of clinical outcomes
Authors I/C Main results
Onset of exacerbation events
Cruz et al.5) I: home telemonitoring C: usual care
Respiratory exacerbations
Incidence of respiratory events (RCT 1): I=9/50, C=15/49; p=0.152 Mean number of exacerbations (NRCT 1): I/C=0.65±1.4/1.01±1.4; p=0.004 Kamei et al.9) I: telenursing
C: conventional treatment
Exacerbation rates, 3M after I
Meta-analysis results (RCT 2): RR=0.57 (95% CI 0.41-0.79); p=0.0008 Franek10) I: home telemonitoring
C: usual care
Exacerbation (NRCT 1): p>0.05
Bolton et al.12) I: home telemonitoring C: usual (home) care
Number of COPD exacerbations RCT 1, NRCT 1: p=NS
RCT 1, NRCT 1: statistically significant reduction I group (p<0.004 and p<0.001, respectively)
Dyspnea scale
Flodgren et al.2) I: telemedicine C: usual care
Activity of daily living CRQ-D at 6M (RCT 1): I=21.3 (6.0), C=19.9 (6.2); p=0.51
Lundell et al.3) I: telehealthcare C: ordinary care
Dyspnea score (CRQ-D, MRC, SOBQ)
Meta-analysis (RCT 7): SMD=0.088 (95% CI -0.056-0.233); p=0.232 Quality of life
Flodgren et al.2) I: telemedicine C: usual care
SGRQ (RCT 1) at 3M: I/C=-10.3 (-17.4--3.1)/-0.6 (-6.5-5.3); p=0.018 CRQ total (RCT 1) at 6M: I/C, mean±SD=99.9±16.8/94.5±22.6; p=NS SF-36 (RCT 1) at 6M: p=NS
Pedone and Lelli4) I: telemonitoring C: usual care
QoL (RCT 1): Statistically significant improvement in I group SGRQ (RCT 2): p=NS
QoL (RCT 4): not modified Cruz et al.5) I: home telemonitoring
C: usual care
SGRQ total (RCT 2)
Meta-analysis results: SMD=-0.53 (95% CI -0.97--0.09); p=0.019 Joe and Demiris8) I: mobile phones
C: usual care
SF-12 (RCT 1): I, baseline/12 weeks=38.7/45.4; p<0.01
Kamei et al.9) I: telenursing
C: conventional treatment
SGRQ
RCT 2: clinically significantly improved in I group RCT 1: clinically significantly improved in C group Franek10) I: home telelemonitoring
C: usual care
SGRQ (RCT 2)
Mean change from baseline (RCT 1): I/C=-10.3 (95% CI -17.1--3.1)/
-0.6 (-6.5-5.3); p=0.018 RCT 1: p=0.83
EQ-5D (RCT 1): p=0.64 I: telephone only support
C: usual care
CSES (RCT 1): median, IQR I=0.5, 0.7/C=0.3, 0.6; p=0.009 Bolton et al.12) I: home telemonitoring
C: usual (home) care
Patient’s self-reported QoL (RCT 1, NRCT 1): only 1 RCT observed significant improvement
McLean et al.13) I: telehealthcare C: usual care
SGRQ
Meta-analysis results (RCT 2): MD=-6.57 (95% CI -13.62-0.48); p=0.068 Polisena et al.14) I: home telehealth
C: usual care
CRQ (RCT 1): NS
CRQ (pre-post 1): significant improvement in I group SGRQ (RCT 1): significant improvement in I group COPD questionnaire (prospective study 1): p=NS Mortality rates
Pedone and Lelli4) I: telemonitoring C: usual care
RCT 4, no significant effects of I was evidenced in reducing deaths
Efficacy Scale(CSES), EuroQoL 5D(EQ-5D), 36-item short form health survey(SF-36) 등이 사용되었다.
삶의 질 결과에 대해 양적합성을 수행한 연구는 2편5,13)이 었다. Cruz5)의 연구에서 RCT 2편을 메타분석한 결과, SGRQ 총점을 고려 시 가정 원격모니터링군이 대조군에 비 해 건강관련 삶의 질 향상이 더 컸으나[standardized mean difference -0.53, 95% confidence interval(이하 CI) -0.97~
-0.09, p=0.019), 하위 영역별 점수는 두 군 간 유의한 차이 가 없었다. McLean13)의 연구에서 RCT 2편의 합성 결과 SGRQ 평균차이가 임상적으로 유의한 차이(-4.0)를 보였으 나, 신뢰구간이 매우 넓었다(mean difference -6.57, 95% CI -13.62~0.48). 나머지 연구에서도 원격 의료군이 비교군보다 삶의 질이 우수하거나 유사한 경향성을 나타냈다.
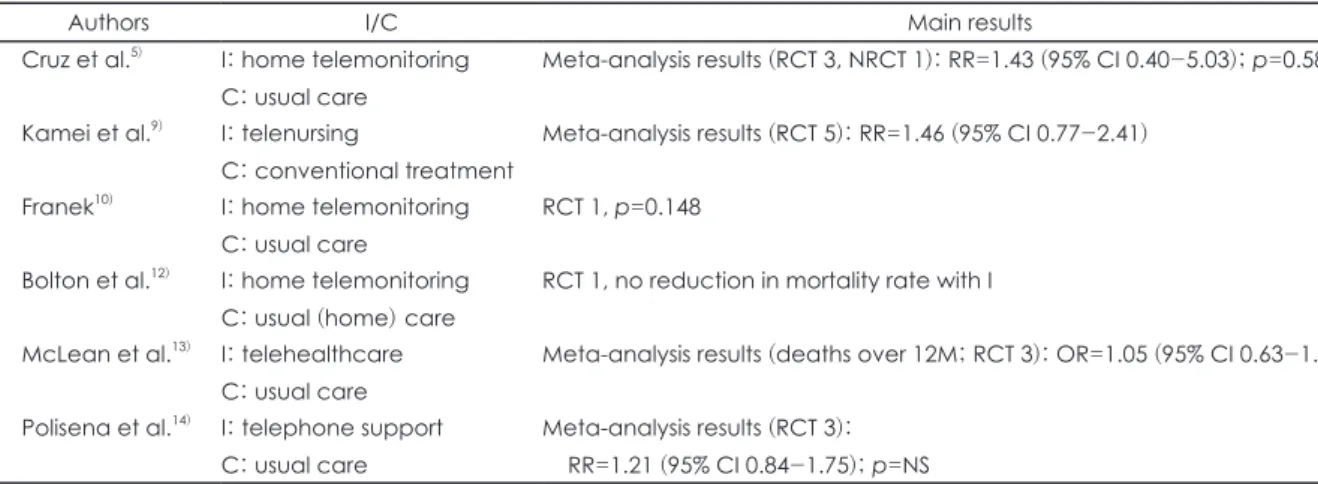
사망률
COPD 환자를 대상으로 원격의료 중재 시 사망률을 보고 한 문헌은 7편4,5,9,10,12-14)이었다(표 2). 양적합성을 수행한 연 구는 4편5,9,13,14)이었다. 각각 원격모니터링, 원격간호, 원격의 료, 전화 지원 중재에 대한 문헌을 메타분석한 결과 일상 진 료군 간에 사망률에는 통계적으로 유의한 차이가 나타나지 않았다. 나머지 연구 3편4,10,12)에서도 모두 원격모니터링군에 서 대조군과 비교 시 사망률의 유의한 감소 효과가 나타나지 않았다.
입원율
COPD 환자를 대상으로 원격의료 중재 시 의료이용도를 입 원율 결과로 보고한 문헌은 6편2,5,9,10,13,14)이었다(표 3). 이 중 양 적합성을 수행한 연구는 3편5,9,13)이었다. Cruz5)의 연구는
RCT 6편과 NRCT 2편을 메타분석한 결과, 가정 원격모니 터링군이 일상 진료군보다 입원 위험이 유의하게 낮게 나타 났다[risk ratio(이하 RR) 0.72, 95% CI 0.53~0.98, p=0.034].
이와 유사하게 Kamei9)의 연구에서도 RCT 4편과 NRCT 2편 을 메타분석한 결과, 원격 간호군이 일상 진료군보다 입원 위험이 유의하게 낮게 보고되었다(RR 0.80, 95% CI 0.68~
0.94, p=0.007). 중재기간을 기준으로 하위군 분석 시 3개월 이하, 6개월, 12개월 모두 두 군 간 통계적으로 유의한 차이 가 없었다. 반면, 질병 중증도를 기준으로 하위군 분석 시 중 등도 COPD와는 달리 중증에서 매우 중증인 COPD 환자의 경우 원격 간호군이 일상 진료군보다 입원 위험이 유의하게 낮게 보고되었다(RR 0.81, 95% CI 0.69~0.95, p=0.007). 마 찬가지로, McLean13)의 연구에서 RCT 6편을 메타분석한 결 과 12개월 동안 병원에 1회 이상 입원환 환자수를 비교 시 원 격보건 의료군이 대면 일상 진료군보다 입원 위험이 유의하 게 낮았다[odds ratio(이하 OR) 0.46, 95% CI 0.33~0.65, p<
0.0001].
나머지 Flodgren2)과 Franek10)의 연구에서는 두 군 간 유의 한 차이가 보고된 결과가 없었고, Polisena14)의 연구에서는 포함된 RCT 2편 각각에서 전화 중재군이 일상 진료군보다 입원율이 유의하게 낮은 것으로 보고하였다.
응급실 방문율
COPD 환자를 대상으로 원격의료 중재 시 의료이용도를 응급실 방문율 결과로 보고한 문헌은 3편2,5,14)이었다(표 3).
이 중 양적합성을 수행한 연구는 1편5)이었으며, RCT 4편을 메타분석한 결과 원격모니터링군과 일상 진료군의 응급실 방문 위험은 유의한 차이가 나타나지 않았다(RR 0.68, 95%
Table 2. Results of clinical outcomes (continued)
Authors I/C Main results
Cruz et al.5) I: home telemonitoring C: usual care
Meta-analysis results (RCT 3, NRCT 1): RR=1.43 (95% CI 0.40-5.03); p=0.582
Kamei et al.9) I: telenursing
C: conventional treatment
Meta-analysis results (RCT 5): RR=1.46 (95% CI 0.77-2.41)
Franek10) I: home telemonitoring C: usual care
RCT 1, p=0.148
Bolton et al.12) I: home telemonitoring C: usual (home) care
RCT 1, no reduction in mortality rate with I
McLean et al.13) I: telehealthcare C: usual care
Meta-analysis results (deaths over 12M; RCT 3): OR=1.05 (95% CI 0.63-1.75)
Polisena et al.14) I: telephone support C: usual care
Meta-analysis results (RCT 3):
RR=1.21 (95% CI 0.84-1.75); p=NS
C: comparator (95%), CI: confidence interval, COPD: chronic obstructive pulmonary disease, CRQ (-D): Chronic Respiratory Questionnaire (-Dyspnea subscale), EQ-5D: EuroQoL 5-D, I: intervention, IQR: interquartile, M: month(s), MD: mean difference, MRC: Medical Research Council, NRCT: non-randomized controlled trial, NS: not statistically significant, OR: odds ratio, QoL: quali- ty of life, RCT: randomized controlled trial, RR: risk ratio, SD: standard deviation, SF-36: 36-item short form health survey, SGRQ: St George’s Respiratory Questionnaire, SMD: standardized mean difference, SOBQ: Shortness of Breath Questionnaire
CI 0.38~1.18, p=0.179).
나머지 Flodgren2)의 연구는 RCT 1편을 포함하였으며 원 격 의료군과 일상 진료군 간에 응급실 방문율은 유의한 차 이가 없었던 반면, Polisena14)의 연구에 포함된 RCT 1편에서 는 전화 지원 중재군이 일상 진료군보다 응급실 방문율이 유의하게 낮게 나타났다(각각 40.6% 및 63.2%, p=0.002).
경제성 결과
COPD 환자를 대상으로 한 원격의료 중재의 경제성 결과 를 보고한 문헌은 총 5편이었다. 의료관련 비용 및 절감에 대해서 보고한 문헌이 4편2,5,11,12)이었고, 일인당 평균 비용에 대해서 보고한 문헌이 1편7)이었다.
의료 관련 비용 결과에서 Flodgren2)의 연구에서는 RCT 1 편을 토대로 원격 의료군과 일상 진료군 간에 전체 보건의 료 비용에는 차이가 없었다고 보고하였다. 반면, Cruz5)의 연 구에서는 원격모니터링군에서 일상 진료군보다 의료비용이 더 감소하는 경향을 보고하였으며, Wootton11)에 포함된 RCT 1편에서는 장기 산소요법 치료를 받는 병원기반 가정 간호 프로그램군에서 비교군에 비해 전체 비용 절감(US$ 46823) 을 보고하였다. 이와 유사하게 Bolton12)의 연구에서도 원격
모니터링군에서 환자당 50% 또는 15%의 비용 절감을 보고 하였으며, 비용 절감 효과에는 입원 횟수 감소 등이 주요한 원인으로 작용했을 것으로 추정하였다.
일인당 평균 비용을 보고한 Udsen7)의 연구에서는 RCT 6 편에서 입원, 응급실 또는 외래 방문, 원격의료 실행, 가정 방 문 등의 비용을 비교한 결과, 원격모니터링군에서 일상 진료 군보다 비교적 더 낮은 일인당 평균 비용을 확인하였다.
중재적용 측면 결과
COPD 환자를 대상으로 원격의료 중재를 적용하는 측면 의 결과를 보고한 문헌은 총 3편6,10,13)이었다.
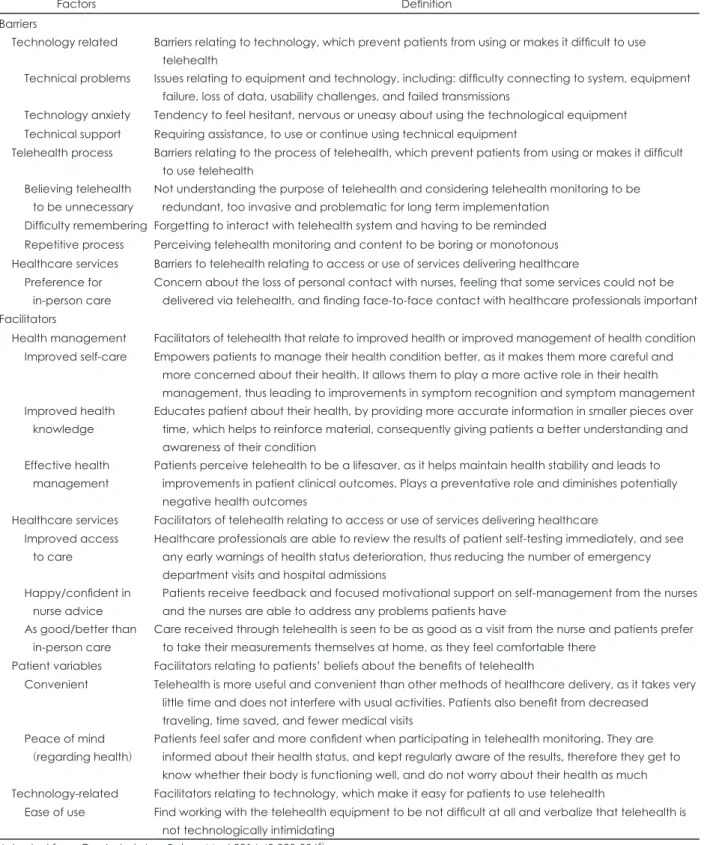
Gorst6)의 연구는 심부전 및 COPD 환자를 대상으로 가정 원격의료 중재의 수용과 지속적 사용에 관한 총 37편의 연구 를 서술적으로 합성하였다. 원격의료를 제공받은 환자 중 약 3분의 1 가량이 중재 참여를 거부하였고, 중재를 수용했던 참가자 중 5분의 1이 이후에 원격의료를 철회하였다고 보고 하였다. 또한, 가정 원격의료 사용에 있어서 환자 측면의 장 애요인 7가지와 촉진요인 9가지를 보고하였다(표 4). 장애요 인으로는 기술 관련 요인(장비 등의 기술적 문제, 기술에 대 한 불안감, 기술적인 지원필요), 원격의료 과정과 관련된 요 Table 3. Results of healthcare utilizations
Authors I/C Main results
Hospitalization rates
Flodgren et al.2) I: telemedicine C: usual care
Hospital admission rates (RCT 1): p=NS
Cruz et al.5) I: home telemonitoring C: usual care
Hospitalization rates
Meta-analysis results (RCT 6, NRCT 2): RR=0.72 (95% CI 0.53-0.98), p=0.034 Kamei et al.9) I: telenursing
C: conventional treatment
Hospitalization by COPD
Meta-analysis results (RCT 4, NRCT 2): RR=0.80 (95% CI 0.68-0.94), p=0.007 Franek10) I: home telemonitoring
C: usual care
Proportion of patients with at least one hospitalization during follow-up, I/C RCT 1: 5.3% (1/19)/15.8% (3/19), p>0.05
NRCT 1: 5.3% (1/19)/40.0% (4/10), p>0.05 NRCT 1: 16.0% (8/50)/30.0% (15/50), p>0.05 McLean et al.13) I: telehealthcare
C: usual care
Hospitalizations: OR of having one or more admissions to hospital over 12M Meta-analysis results (RCT 6): OR=0.46 (95% CI 0.33-0.65), p<0.0001 Polisena et al.14) I: telephone support
C: usual care
Number of patients hospitalized RCT 1: I/C=46%/66% (p=0.03) RCT 1: I/C=32%/51% (p=0.01) Emergency department visit rates
Flodgren et al.2) I: telemedicine C: usual care
RCT 1, p=NS
Cruz et al.5) I: home telemonitoring C: usual care
Meta-analysis results (RCT 4): RR=0.68 (0.38-1.18), p=0.179
Polisena et al.14) I: telephone support C: usual care
Number of patients who visited the emergency department (RCT 1) I/C=40.6% (39/96)/63.2% (60/95), p=0.002
C: comparator (95%), CI: confidence interval, COPD: chronic obstructive pulmonary disease, I: intervention, M: month(s), n:
sample size, NRCT: non-randomized controlled trial, NS: not statistically significant, OR: odds ratio, RCT: randomized controlled tri- al, RR: risk ratio
인(원격의료가 불필요할 것이라는 믿음, 시스템에 접속해야 함을 기억하기 어려움, 반복 과정이 지루하거나 단조롭다고 느낌), 보건의료 서비스와 관련된 요인(대면진료 선호)을 제
시하였다. 한편, 촉진요인으로는 보건 관리(자가관리 향상, 보건 지식 향상, 효과적인 보건 관리), 보건의료 서비스(진료 접근성 향상, 간호사의 조언에 동기부여됨, 대면진료보다 우
Table 4. Barriers and facilitators of telehealth
Factors Definition
Barriers
Technology related Barriers relating to technology, which prevent patients from using or makes it difficult to use telehealth
Technical problems Issues relating to equipment and technology, including: difficulty connecting to system, equipment failure, loss of data, usability challenges, and failed transmissions
Technology anxiety Tendency to feel hesitant, nervous or uneasy about using the technological equipment Technical support Requiring assistance, to use or continue using technical equipment
Telehealth process Barriers relating to the process of telehealth, which prevent patients from using or makes it difficult to use telehealth
Believing telehealth to be unnecessary
Not understanding the purpose of telehealth and considering telehealth monitoring to be redundant, too invasive and problematic for long term implementation
Difficulty remembering Forgetting to interact with telehealth system and having to be reminded Repetitive process Perceiving telehealth monitoring and content to be boring or monotonous Healthcare services Barriers to telehealth relating to access or use of services delivering healthcare
Preference for in-person care
Concern about the loss of personal contact with nurses, feeling that some services could not be delivered via telehealth, and finding face-to-face contact with healthcare professionals important Facilitators
Health management Facilitators of telehealth that relate to improved health or improved management of health condition Improved self-care Empowers patients to manage their health condition better, as it makes them more careful and
more concerned about their health. It allows them to play a more active role in their health management, thus leading to improvements in symptom recognition and symptom management Improved health
knowledge
Educates patient about their health, by providing more accurate information in smaller pieces over time, which helps to reinforce material, consequently giving patients a better understanding and awareness of their condition
Effective health management
Patients perceive telehealth to be a lifesaver, as it helps maintain health stability and leads to improvements in patient clinical outcomes. Plays a preventative role and diminishes potentially negative health outcomes
Healthcare services Facilitators of telehealth relating to access or use of services delivering healthcare Improved access
to care
Healthcare professionals are able to review the results of patient self-testing immediately, and see any early warnings of health status deterioration, thus reducing the number of emergency department visits and hospital admissions
Happy/confident in nurse advice
Patients receive feedback and focused motivational support on self-management from the nurses and the nurses are able to address any problems patients have
As good/better than in-person care
Care received through telehealth is seen to be as good as a visit from the nurse and patients prefer to take their measurements themselves at home, as they feel comfortable there
Patient variables Facilitators relating to patients’ beliefs about the benefits of telehealth
Convenient Telehealth is more useful and convenient than other methods of healthcare delivery, as it takes very little time and does not interfere with usual activities. Patients also benefit from decreased traveling, time saved, and fewer medical visits
Peace of mind (regarding health)
Patients feel safer and more confident when participating in telehealth monitoring. They are informed about their health status, and kept regularly aware of the results, therefore they get to know whether their body is functioning well, and do not worry about their health as much Technology-related Facilitators relating to technology, which make it easy for patients to use telehealth
Ease of use Find working with the telehealth equipment to be not difficult at all and verbalize that telehealth is not technologically intimidating
Adapted from Gorst et al. Ann Behav Med 2014;48:323-3366)
수함), 환자 변수(편리함, 마음에 평화를 줌), 기술 관련 요인 (사용이 용이함)을 보고하였다.
이외에도 중재적용 측면의 결과를 직접적으로 보고하지 않았지만, Franek10)의 연구는 원격모니터링은 지역의 정보 기술, 인프라 및 개인에 크게 의존하여 외부 연구 결과의 일 반화가 부족할 수 있기 때문에 가정 원격모니터링을 채택하 고자 하는 관할 구역에서 중재를 먼저 시험해보거나, 적절 한 효과가 입증된 중재에 집중해야 함을 제언하였다. 또한, McLean13)의 연구 중 RCT 1편15)에서 환자들이 평가에 대한 큰 부담으로 중도탈락 하였음을 언급하고 있다.
고 찰
본 연구는 만성폐쇄성폐질환 관리를 위한 원격의료 중재 를 주제로 최근에 발표된 다수의 체계적 문헌고찰을 종합 정리하였다는 데 의의가 있다.
포함된 체계적 문헌고찰은 넓은 의미의 원격의료에 대하 여 검토하거나,2,3,6,7,10,11,13,14) 휴대전화를 이용하는 중재8) 또는 모니터링-기반 원격간호9)처럼 특정 중재에 대하여 수행되 었다. 만성폐쇄성폐질환에 사용되는 원격의료 중재와 관련 하여 분석한 임상 지표 중 일관성 있는 결과 개선을 통해 원 격의료의 효과를 제시한 지표는 없었다. 다만, 최근 문헌들 을 중심으로 원격의료 중재 적용 시 삶의 질 향상에 유의한 효과가 있는 것으로 보고되었으나, 다양한 평가 도구가 사용 되어 삶의 질 결과에 대한 정확한 해석이 어려웠다. 또한, 원 격의료를 통해 입원율이 유의하게 감소하여 이에 따른 의료 비용도 줄어드는 경향을 보이는 것으로 보고되었으나, 우리 나라에서 수행된 연구를 통해 얻어진 결과가 아니므로 불확 실성이 존재한다. 따라서, 만성폐쇄성폐질환 관리에 활용된 원격의료 중재의 이득에 대한 분명한 결론을 도출하기에는 근거가 부족하였다.
본 연구에는 아래와 같은 제한점이 존재하기 때문에 결과 해석 시에는 주의를 요한다.
첫째, 연구에 포함된 문헌들에서 대상자의 특성에 대해서 는 고려하지 않았다. 원격의료의 효과는 연구대상의 연령이 나 질환의 중증도에 따라 달라질 개연성이 있으므로, 향후 추가 연구가 축적되면 연구대상자의 질환 특성에 따른 분석 이 필요할 것이다.
둘째, 연구에 포함된 체계적 문헌고찰에서 원격의료로 규 정하고 포함시킨 중재의 범위가 달랐다. 휴대전화 기반 중재 를 배제한 연구6)가 있는 반면, 휴대전화 중재에 대해서만 초 점을 맞추어 수행된 연구8)도 있었다. 또한, 유사명칭의 중재 일 경우에도 모니터링된 생체지표나 전송 장비 및 주기 등
을 포함한 중재의 세부 내용이 이질적이었다. 원격의료 중재 법은 교육이나 상담 등을 포함한 복합서비스 중재법의 특성 을 지니고 있어, 어떤 중재 유형 및 프로토콜이 효과적인지 에 대한 규명이 이루어져야 임상현장에서 유용하게 적용될 것이다. 이를 위해 추가적인 일차연구가 많이 실행될 필요가 있으며, 이에 앞서 효과적인 중재의 가능성을 제시하는 체계 적 문헌고찰 연구나 메타분석 연구를 수행하는 것도 바람직 할 것이다.
셋째, 본 연구에 포함된 체계적 문헌고찰 문헌마다 평가에 사용된 측정 도구나 결과지표가 상이하였다. 예를 들어 호흡 곤란 점수나 삶의 질에 대한 평가지표가 다양하였다. 정확한 결과 분석을 위해서는 전문가 그룹의 통일된 효과변수 및 지표에 대한 의견합일이 선행되어야 하며, 공통 지표별로 결 과를 합성하여 분석하는 것이 필요하다. 또한 도출된 결과를 해석하기 위해서는 결과 판단기준에 대한 논의도 선행되어 야 할 것으로 생각된다.
넷째, 본 연구에 포함된 이차 연구의 결과들이 매우 이질 적이고 일관성이 없었다. 이러한 결과를 제시한 원인은 각 연구마다 적용된 중재가 다양하였고 서로 다른 설계의 일차 연구가 포함되었기 때문일 것으로 판단된다. 이에 대하여 명 확히 규명하기 위해서는 연구들 간의 매핑(mapping)을 통한 보다 체계적인 분석이 필요할 것으로 사료된다.
다섯째, 본 연구는 이차 문헌에서 보고하는 결론의 전반적 인 경향성을 파악하는 데 주안점을 두었다. 이에 각 이차 문 헌에 포함된 일차 문헌이 중복되었을 개연성이 있으므로, 결 과 해석에 주의를 요한다.
마지막으로, 본 연구에서는 기존의 문헌을 신속하고 효과 적으로 조사하고자 질 평가를 생략하였다. 보건의료 중재에 대한 체계적 문헌고찰 개관에 포함되는 문헌의 질을 평가의 필요여부와 방법에 대한 지침은 아직 제한적이다. 하지만, 일 반적으로 A MeaSurement Tool to Assess Systematic Re- views(AMSTAR)와 같은 도구를 사용하여 체계적 문헌고찰 의 방법론적 질을 평가하여 보고하도록 권고되고 있다. 체계 적 문헌고찰의 질 평가 결과는 일차 연구의 질 평가 및 결과 지표 자료와 함께 개관의 결과와 결론을 맥락과 관련 짓는 데 사용될 수 있다고 여겨지고 있다.16)
본 연구에서 개관한 내용은 추후 관련 연구 설계 시 방향 설 정에 참고자료가 될 수 있을 것으로 판단된다. 또한, 원격의 료 중재가 만성폐쇄성폐질환의 관리에 긍정적인 영향이 있 음이 확증될 경우, 중재적용 측면의 장애요인과 촉진요인을 고려한다면 현명한 도입전략의 수립과 도입과정에서 직면 하게 될 도전과제의 해결에 도움이 될 것으로 사료된다.
본 연구는 만성폐쇄성폐질환에 사용되는 원격의료의 현
황 파악을 주목적으로 수행되었으나, 추후 임상에서의 요구 도를 고려하여 만성폐쇄성폐질환 환자의 자가 관리에 활용 될 수 있을 것으로 기대되는 원격모니터링 중재에 초점을 맞추어 임상 효과 및 비용효과성에 대한 일차 연구를 수행 하는 것이 필요할 것으로 생각된다.
결 론
본 연구는 만성폐쇄성폐질환의 관리에 사용되는 원격의 료 중재에 대하여 파악하고 그 효과를 확인하기 위하여 체 계적 문헌고찰을 개관하였다. 분석한 임상 지표 중 원격의료 를 통해 일관성 있는 결과 개선을 제시한 지표는 없었으나, 최근 문헌들을 중심으로 원격의료 중재 적용 시 삶의 질 향 상에 유의한 효과가 있는 것으로 나타났다. 또한, 원격의료 를 통해 입원율의 유의한 감소와 이에 따른 의료비용의 감 소로 이어지는 경향을 보이는 것으로 보고되었다. 하지만 여 러 연구들에서 사용된 세부중재법에 차이가 있기 때문에, 만 성폐쇄성폐질환의 관리에 활용되는 원격의료에 대한 효과 규명을 위해서는 특정한 중재유형별로 효과를 분석하는 것 이 필요할 것으로 판단된다.
Acknowledgments
본 원고는 2016년도 한국보건의료연구원에서 수행한 연구(과제번 호: NECA-H-16-002) 보고서의 일부 내용을 발췌 및 수정한 것임.
REFERENCES
1) 대한결핵 및 호흡기학회. COPD 진료지침. 서울: 대한결핵 및 호 흡기학회;2014.
2) Flodgren G, Rachas A, Farmer AJ, Inzitari M, Shepperd S. Interac- tive telemedicine: effects on professional practice and health care outcomes. Cochrane Database Syst Rev 2015:CD002098.
3) Lundell S, Holmner Å, Rehn B, Nyberg A, Wadell K. Telehealthcare in COPD: a systematic review and meta-analysis on physical out- comes and dyspnea. Respir Med 2015;109:11-26.
4) Pedone C, Lelli D. Systematic review of telemonitoring in COPD: an update. Pneumonol Alergol Pol 2015;83:476-484.
5) Cruz J, Brooks D, Marques A. Home telemonitoring effectiveness in COPD: a systematic review. Int J Clin Pract 2014;68:369-378.
6) Gorst SL, Armitage CJ, Brownsell S, Hawley MS. Home telehealth uptake and continued use among heart failure and chronic obstructive
pulmonary disease patients: a systematic review. Ann Behav Med 2014;48:323-336.
7) Udsen FW, Hejlesen O, Ehlers LH. A systematic review of the cost and cost-effectiveness of telehealth for patients suffering from chron- ic obstructive pulmonary disease. J Telemed Telecare 2014;20:212- 220.
8) Joe J, Demiris G. Older adults and mobile phones for health: a review.
J Biomed Inform 2013;46:947-954.
9) Kamei T, Yamamoto Y, Kajii F, Nakayama Y, Kawakami C. System- atic review and meta-analysis of studies involving telehome monitor- ing-based telenursing for patients with chronic obstructive pulmo- nary disease. Jpn J Nurs Sci 2013;10:180-192.
10) Franek J. Home telehealth for patients with chronic obstructive pul- monary disease (COPD): an evidence-based analysis. Ont Health Technol Assess Ser 2012;12:1-58.
11) Wootton R. Twenty years of telemedicine in chronic disease manage- ment--an evidence synthesis. J Telemed Telecare 2012;18:211-220.
12) Bolton CE, Waters CS, Peirce S, Elwyn G; EPSRC and MRC Grand Challenge Team. Insufficient evidence of benefit: a systematic review of home telemonitoring for COPD. J Eval Clin Pract 2011;17:1216- 1222.
13) McLean S, Nurmatov U, Liu JL, Pagliari C, Car J, Sheikh A. Telehealth- care for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2011:CD007718.
14) Polisena J, Tran K, Cimon K, Hutton B, McGill S, Palmer K, et al.
Home telehealth for chronic obstructive pulmonary disease: a system- atic review and meta-analysis. J Telemed Telecare 2010;16:120-127.
15) Bourbeau J, Julien M, Maltais F, Rouleau M, Beaupré A, Bégin R, et al. Reduction of hospital utilization in patients with chronic obstruc- tive pulmonary disease: a disease-specific self-management interven- tion. Arch Intern Med 2003;163:585-591.
16) Pollock M, Fernandes RM, Hartling L. Evaluation of AMSTAR to assess the methodological quality of systematic reviews in overviews of reviews of healthcare interventions. BMC Med Res Methodol 2017;17:48.
17) Institute of Medicine, Committee on Evaluating Clinical Applica- tions of Telemedicine, Field MJ. Telemedicine: a guide to assessing telecommunications for health care. Washington, D.C.: National Acad- emy Press;1996.
18) McLean S, Nurmatov U, Liu JL, Pagliari C, Car J, Sheikh A. Tele- healthcare for chronic obstructive pulmonary disease: Cochrane Re- view and meta-analysis. Br J Gen Pract 2012;62:e739-e749.
19) Miller EA. Solving the disjuncture between research and practice:
telehealth trends in the 21st century. Health Policy 2007;82:133-141.
20) Jaana M, Paré G, Sicotte C. Home telemonitoring for respiratory conditions: a systematic review. Am J Manag Care 2009;15:313-320.
21) icn.ch [Homepage on the Internet] International Council of Nurses;
Telenursing fact sheet [cited 2011 Dec 1]. Available from: http://
www.icn.ch/images/stories/documents/publications/fact_sheets/18b_
FS-Telenursing.pdf.
Appendix. Operational definition of telehealth
Intervention Authors Operational definition
telehealthcare Lundell et al.3) The use of electronic information and communications technologies to provide and support health care when distance separates the participants17)
McLean et al.13)Healthcare at a distance, involving the communication of data from the patient to the health carer, usually a doctor or nurse, who then processes the information and responds with feedback regarding the management of the illness
telehealth Gorst et al.6) Intervention that specifically utilized technology as a means of delivering healthcare Udsen et al.7) Mclean et al.’s adaptation18) of Miller’s conceptualization of telehealth19) in the most recent
systematic review: patients measure standardized physical indicators periodically, these physical indicators are transmitted by telecommunication technology, and a healthcare professional interprets these data provides the patient with feedback.
Franek10) Telehealth: using advanced information and communication technologies and electronic medical devices to support the delivery of clinical care, professional education, and health-related administrative services
Telemonitoring (or remote monitoring): the use of medical devices to remotely collect a patient’s vital signs and/or other biologic health data and the transmission of those data to a monitoring station for interpretation by a health care provider
Telephone only support: disease/disorder management support provided by a health care provider to a patient who is at home via telephone or videoconferencing technology in the absence of transmission of patient biologic data
Polisena et al.14)Home telemonitoring: remote care delivery or monitoring that occurs between the patients in their place of residence and the health-care provider located somewhere else
Telephone support: patient or caregiver support by a health-care provider through telephone contact. It does not involve electronic transmission of patient outcome data
telemedicine Flodgren et al.2)The patient is at a different location to the healthcare professional and transmits clinical information via a telecommunication technology and the healthcare professional responds Pedone and
Lelli4)
Delivery of health services via remote telecommunications
Wootton11) Wide definition - medicine practised at a distance
telemonitoring Cruz et al.5) Periodically record clinical data (e.g., oxygen saturation, heart rate, symptoms) in their homes and transmit the data on a regular basis (i.e., ≥5 days/week) using information and communication technologies for further assessment by a healthcare team
Bolton et al.12) The use of telecommunication technologies by patients for the timely transmission of data (e.g., spirometric measures, vital signs and symptoms) from home to a health care service centre20)
Additionally, operationalized the definition further:
require the patient or their carer to periodically measure physiological indicators (e.g., arterial oxygen saturation and heart rate) and/or record their symptoms/vital signs in a standardized format
Use telecommunication technologies (e.g., telephone, internet, web-phone) that either manually or automatically transferred the patients health status data from home to a health care service
Lead to the automated or manual review of the patient’s health status data
Involve an automated or manual response when the patients health status data crossed a pre-defined threshold
telenursing Kamei et al.9) Use of telecommunications technology in nursing, including the use of electromagnetic channels to transmit voice, data, and video communication signals for the purpose of enhanc- ing patient care21)