Original Article
중등도 이상의 만성폐쇄성폐질환 환자에서 흡입용
기관지확장제와 흡입용 기관지확장제/스테로이드 병합요법의 효과 및 안전성 평가
이수경†, 강효정, 윤정이, 권은영, 강진숙 가톨릭대학교 서울성모병원 약제부
Efficacy and Safety of Inhaled Bronchodilator Versus Inhaled Bronchodilator/Inhaled Corticosteroid in Patients with Moderate
to Severe Chronic Obstructive Pulmonary Disease
Soo Kyung Lee†, Hyo Jung Kang, Jeong Yi Yoon, Eyn Young Kwon and Jin Suk Kang
Department of Pharmacy, Seoul St. Mary’s Hospital, The Catholic University of Korea 222 Banpo-daero, Seocho-gu, Seoul, 06591, Republic of Korea
Background : According to the treatment guidelines for Chronic Obstructive Pulmonary Dis- ease (COPD), long-acting β2 agonists (LABA) and long-acting muscarinic antagonists (LAMA) are recommended. Addition of inhaled corticosteroid (ICS) is more effective in reducing acute exacerbations in patients with exacerbations and moderate to very severe COPD, but some studies have shown that it could increase the risk of pneumonia. Therefore, this study was conducted to evaluate the efficacy and safety of LABA/LAMA versus LABA/LAMA/ICS.
Methods : Between January 2016 and June 2017, medical records of patients with moderate to severe COPD who visited the Department of Pulmonology in one hospital and started using LABA/LAMA (dual therapy) or LABA/LAMA/ICS (triple therapy) were reviewed retrospectively.
The efficacy between in the two groups was evaluated as the number of acute exacerbations and change in pulmonary function. We also analyzed adverse drug reactions including pneumonia.
투고일자 2020.10.13; 심사완료일자 2020.11.20; 게재확정일자 2020.12.16
†교신저자 이수경 Tel:02-2258-2533 E-mail:[email protected]
Results : A total of 53 patients received dual therapy and 47 patients received triple therapy.
The rate of acute exacerbations was reduced and change in FEV1 (Forced expiratory volume for 1 second) was improved in each group, but there was no difference between the two groups.
Pneumonia occurred in 7.5% of patients receiving dual therapy versus 4.3% of patients receiv- ing triple therapy, and other adverse drug reactions occurred in 11.3% of patients receiving dual therapy versus 4.3% of patients receiving triple therapy.
Conclusion : Reduction in the rate of acute exacerbations in the triple therapy group was not significantly better than that in the dual therapy group, but adverse drug reactions, including pneumonia also did not show a difference between the two groups.
[Key words] Chronic obstructive pulmonary disease (COPD), Inhaled corticosteroid (ICS), Acute exacerbation, Pulmonary function, Pneumonia
만성폐쇄성폐질환(Chronic obstructive pul- monary disease, COPD)는 완전히 회복되지 않 는 기류제한을 특징으로 하는 폐질환이다. 만성 염증 에 의한 기도와 폐 실질의 손상으로 인해 발생하며 호 흡곤란, 기침, 가래 등의 지속적인 호흡기계 증상을 동반한다. COPD는 전 세계적으로 높은 사망률과 유 병률을 나타내고 있으며, COPD로 인한 의료비가 급 증하는 등 사회경제적인 부담이 발생하고 있다.1) 대 한결핵 및 호흡기학회 COPD 진료지침 2018 개정판 에서는 COPD 환자의 증상, 폐활량, 악화위험을 평 가하고 이에 따라서 약물 치료를 권고하고 있다. 환자 의 증상은 호흡곤란과 삶의 질로 평가하며 평가 도구
로는 mMRC 호흡곤란점수(modified Medical Research Council Dyspnea Scale), COPD 평 가검사(COPD Assessment Test, CAT)가 있다.
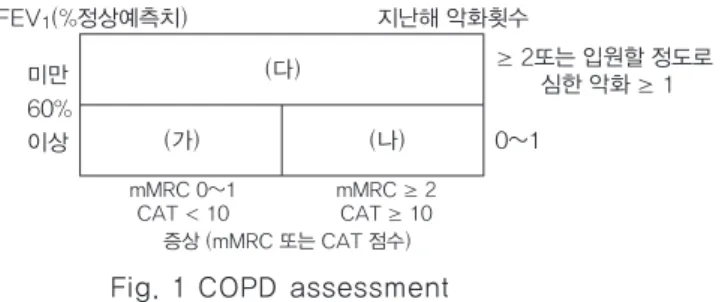
환자의 폐활량은 강제호기량(Forced expiratory volume for 1 second, FEV1)으로 평가하며, FEV1을 정상 예측치 대비 60% 이상과 미만으로 나누 어 가, 나, 다군으로 환자를 분류하고, 환자군마다 다 른 치료요법을 권장하고 있다(Fig. 1). 특히 mMRC 또는 CAT 점수와 상관없이 FEV1이 정상 예측치의 60% 미만이거나 지난 1년간 2회 이상 급성악화 또는 입원할 정도로 심한 악화의 이력이 있는 다군 환자의 치료에는 LABA (Long-acting β2 agonist)/
Fig. 1 COPD assessment
(가) group: low exacerbation risk, minor symptoms. FEV1 is more than 60%, no exacerbation or 1 exacerbation in previous year and mMRC score is 0~1 (or CAT score is below 10). (나) group: low exacerbation risk, severe symptoms. FEV1 is more than 60%, no exacerbation or 1 exacerbation in previous year and mMRC score is 2 or more(or CAT score is 10 or more). (다) group: high exacerbation risk. FEV1 is less than 60% regardless of mMRC or CAT score or 2 or more acute exacerbations in previous year or 1 or more severe exacerbations that need hospitalization.
출처: The Korean Academy of Tuberculosis and Respiratory Diseases: COPD Clinical Practice Guidelines 2018 FEV1(%정상예측치) 지난해 악화횟수
미만 60%
이상
(다)
(가) (나)
mMRC 0~1
CAT < 10 mMRC ≥ 2
CAT ≥ 10
≥ 2또는 입원할 정도로 심한 악화 ≥ 1 0~1
증상 (mMRC 또는 CAT 점수)
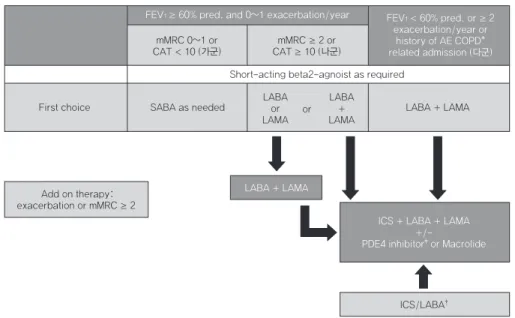
LAMA (Long-acting muscarinic antagonist) 의 병용요법을 일차적으로 권장하고 있다. 그러나 LABA/LAMA 병합요법에도 불구하고 mMRC 2 점 이상의 증상이 지속되거나 급성악화가 발생하는 경우 ICS (Inhaled corticosteroids)를 추가하 여 LABA/LAMA/ICS 3제요법을 권장하고 있다 (Fig. 2).1)
GOLD (Global Initiative for Chronic ob- structive lung disease) 2018 report에서는 한 국의 진료지침과는 다르게 환자를 네 군으로 나누어 각 군에 따라 치료 요법을 권장하고 있다. 폐기능 검 사로 FEV1/FVC (Forced vital capacity) 비율 이 0.7 미만인 경우 COPD로 확진한 후 기류제한의 정도를 FEV1 수치로 평가한다. 그 후 중등도 이상의 악화 이력과 mMRC 또는 CAT을 통해 A, B, C, D 네 군으로 나누고 각 군마다 다른 치료 요법을 권장한 다(Fig. 3, 4). 그 중 D군에서는 LABA/LAMA 병 합요법이 초기 치료 요법으로 추천되고 있으나, 혈중
호산구 수치가 높은 경우 ICS/LABA의 초기 사용 가 능성을 제안하고 있으며, LABA/LAMA를 사용하 는 환자에게서 급성악화가 있는 경우에는 LABA/
LAMA/ICS로 대체하도록 제안하고 있다.2) COPD 환자를 대상으로 LABA/LAMA/ICS 3제 요법군과 LABA/LAMA 2제요법군의 효과 및 안전 성을 비교한 기존 연구 중 fluticasone furoate/
umeclidinium/vilanterol 3제요법군과 fluti- casone furoate/vilanterol 또는 umeclidini- um/vilanterol 2제요법군 비교연구에서는 3제요 법군이 2제요법군에 비해 연간 중등도 이상의 급성악 화 빈도는 유의하게 낮았으나 폐렴 발생 빈도는 fluticasone furoate를 포함한 군에서 더 높게 나 타났다.3) 그러나 beclometasone dipropionate /formoterol fumarate/glycopyrronium 3제 요법군과 indacaterol/glycopyrronium 2제요 법군을 비교한 다른 연구에서는 3제요법군에서 중등 도 이상의 연간 급성악화가 유의하게 감소하였으며
FEV1 ≥ 60% pred. and 0~1 exacerbation/year FEV1 < 60% pred. or ≥ 2 exacerbation/year or
history of AE COPD*
related admission (다군) mMRC 0~1 or
CAT < 10 (가군)
Short-acting beta2-agnoist as required mMRC ≥ 2 or
CAT ≥ 10 (나군)
First choice SABA as needed LABA
LAMAor or LABA LAMA+
LABA + LAMA
ICS + LABA + LAMA PDE4 inhibitor+/-‡ or Macrolide
ICS/LABA† LABA + LAMA
Add on therapy:
exacerbation or mMRC ≥ 2
Fig. 2 Pharmacological therapy in stable COPD
*AE COPD: Acute exacerbation of COPD.
† Asthma overlap or high blood eosinophil
‡ COPD with acute exacerbation history and chronic bronchitis: 1) FEV1 is less than 50% or 2 or more acute exacerbation although continuous administration of LABA or LAMA
SABA: Short-Acting Beta2-Agonists, LABA: Long-Acting Beta2-Agonists, LAMA: Long-Acting Muscarinic Antagonist.
출처: The Korean Academy of Tuberculosis and Respiratory Diseases: COPD Clinical Practice Guidelines 2018
폐렴 발생 빈도는 두 군간 차이가 없는 것으로 나타났 다.4) 이러한 연구들을 통해 COPD 환자에게 LABA/
LAMA/ICS 3제요법을 사용하는 것이 연간 급성악 화 빈도를 낮추는 것으로 보고되고 있으나 ICS 사용 과 폐렴 발생 위험 증가 간의 연관성에 대한 연구들은 서로 상반되는 결과들이 나타나고 있어 COPD 환자
에서 ICS 병합요법에 대한 연구가 추가적으로 필요 한 실정이다.5),6)
이에 본 연구에서는 COPD 환자를 대상으로 LA BA/LAMA 2제요법군와 LABA/LAMA/ICS 3제 요법군 간의 급성악화 빈도, 폐기능 변화, 폐렴 발생 횟수 및 기타 부작용을 비교하여 효과 및 안전성을 평 Fig. 3 ABCD assessment tool
Fig. 4 Initiation of pharmacological therapy of COPD
출처: GOLD(Global initiative for chronic obstructive lung disease) 2018 report
출처: GOLD(Global initiative for chronic obstructive lung disease) 2018 report
가하고자 한다. 또한 최근 COPD 환자 중 혈중 호산 구수가 2~4% 이상으로 높은 환자에게 ICS를 사용 하는 것이 급성악화 감소에 효과가 있는 것으로 보고 되고 있으며, 혈중 호산구수가 COPD 환자에서 ICS 사용의 효과를 예측하는 지표로도 사용될 수 있는 가 능성을 나타내는 연구 결과들이 보고되고 있어, 이를 바탕으로 본 연구에서는 LABA/LAMA/ICS 3제요 법군에서 혈중 호산구수가 2% 이상인 군과 2% 미만 인 군으로 나누어 두 군간의 하위그룹 분석을 통해 그 효과 및 안전성을 평가하고자 한다.7)-11)
연구방법
1. 연구대상자 및 연구방법
2016년 1월부터 2017년 6월까지 본원 호흡기내과 에 방문한 중등도 이상의 COPD 환자를 대상으로 사 용하는 흡입제에 따라 LABA/LAMA를 사용하는 환 자군(2제요법군)과 LABA/LAMA/ICS를 사용하 는 환자군(3제요법군)으로 나누어 이후 1년간의 전 자의무기록 검토를 통해 후향적으로 연구를 실시하였 다. 전자의무기록을 통해 성별, 연령, 체중, 신장, 흡연여부, 유병기간 등 기본 정보 및 인구학적 특성 정보를 수집하였으며, 연간 악화 빈도(입원 빈도, 경 구스테로이드 또는 항생제 사용 빈도 포함), 폐기능 변화, 폐렴 발생 빈도, 기타 부작용 종류 및 빈도를 확인하여 두 군간의 효과 및 안전성을 비교 분석하였 다. 또한 3제요법군에서 혈중 호산구수에 따라 2% 이 상인 군과 2% 미만인 군으로 나누어 두 군간의 악화 빈도, 폐기능 변화에 대한 하위그룹 분석을 실시하였 다. 연구 대상자는 만 19세 이상의 성인으로 FEV1이 정상 예측치의 60% 미만이며 LABA/LAMA 2제 혹 은 LABA/LAMA/ICS 3제요법으로 처음 흡입제 사 용을 시작한 환자 및 기존 흡입제에서 2제 또는 3제요 법으로 신규 변경한 환자 모두를 포함하여 1년 이상 유지한 환자로 선정하였으며, 두 군 모두 흡입제 성분 에 제한을 두지 않았다. 2제요법군의 경우 indaca- terol/tiotropium, indacaterol/ glycopyrro- nium, indacaterol/aclidinium 또는 vilan- terol/umeclidinium을, 3제요법군의 경우 for- moterol/tiotropium/beclomethasone, for-
moterol/tiotropium/budesonide, formoter- ol/tiotropium/ fluticasone, formoterol/ac- lidinium/beclomethasone, salmeterol/ti- otropium/fluticasone 또는 salmeterol/ac- lidinium/fluticasone을 사용하였다. 천식의 기 왕력이 있거나 폐기능검사를 1회 이하 시행한 환자는 대상에서 제외하였으며, 연구기간 중 COPD 치료 약 제 변경이 있는 환자는 제외하였으나 급성악화 치료 시 일시적으로 약제 변경이 있었던 경우는 연구 대상 에 포함하였다.
2. 평가 지표
1차 평가 지표는 LABA/LAMA 2제요법군과 LA BA/LAMA/ICS 3제요법군 간의 연간 급성악화 빈 도로 1년간 입원 빈도, 경구스테로이드 또는 항생제 사용 빈도를 포함하였으며, 2차 평가 지표로는 두 군 간의 1년간 폐기능 변화(FEV1, FVC, FEV1/FVC 변화), 폐렴 발생 빈도 및 기타 부작용 종류와 빈도를 확인하였다. 또한 3제요법군에서 혈중 호산구수에 따라 2% 이상인 군과 2% 미만인 군 사이의 연간 급 성악화 빈도 및 폐기능 변화에 대한 하위그룹 분석을 실시하였다.
3. 통계 분석
1차 평가 지표인 1년간 급성악화 빈도 분석은 Wil- coxon rank sum test, Chi-square test 또는 Fisher’s exact test를 사용하였다. 2차 평가 지표 인 폐기능검사 결과는 Wilcoxon rank sum test, T-test로 분석하였고 폐렴과 기타 부작용 빈도는 Fisher’s exact test로 분석하였다. 혈중 호산구 수에 따른 하위그룹 분석에는 T-test, Wilcoxon rank sum test를 사용하였으며 모두 SAS 통계 프 로그램을 이용하였다.
4. 피험자 보호
본 연구는 가톨릭대학교 서울성모병원 기관윤리심 의위원회(Institutional Review Board, IRB)의 승인을 받아 진행하였다(IRB No. KC18RESI0428).
연구결과
1. 연구대상자의 인구학적 특성
연구대상자는 LABA/LAMA 2제요법군이 53명, LABA/LAMA/ICS 3제요법군이 47명이었으며, 2 제요법군이 3제요법군에 비해 연령이 유의하게 높게 나타났으나, 그 외 다른 항목에서는 두 군간 유의한 차이가 없었다(Table 1).
2. 효과 분석
1) 연간 급성악화 빈도
연간 급성악화 빈도는 LABA/LAMA 2제요법군의 경우 1년간 흡입제 사용 후 통계적으로 유의하게 감 소하였으나, LABA/LAMA/ICS 3제요법군에서는 통계적으로 유의한 감소는 없었다(Table 2).
1년간 흡입제 사용 후 연간 급성악화 빈도 변화에서 는 2제요법군과 3제요법군 간 통계적으로 유의한 차 이가 없었고(Table 3), 중등증 이상의 급성악화를 나타내는 항생제 치료, 경구스테로이드 치료 또는 입 원의 경우에서도 두 군간 유의한 차이는 확인되지 않 Table 1 Baseline characteristics of study population
Age (years) 71.4±9 65.3±10.9 0.003
Gender (n (%)) 0.729
Male 39 (73.6) 36 (76.6)
Female 14 (26.4) 11 (23.4)
Height (cm) 163.4±7.5 163.7±7.5 0.838
Weight (kg) 59±11.4 59.7±11.1 0.737
Smoking history (n (%)) 0.865
Smoker 4 (7.6) 5 (10.6)
Ex-smoker 34 (64.2) 28 (59.6)
Non-smoker 15 (28.3) 14 (29.8)
Smoking period (years) 41±42.9 30.7±28.6 0.313
Duration of COPD (years) 3.9±3.7 3.6±3.8 0.359
Blood eosinophil counts (n (%)) 0.089
<2% 25 (51) 14 (33.3)
≥2% 24 (49) 28 (66.7)
FEV1* (L) 1.3±0.3 1.2±0.4 0.243
FVC† (L) 2.7±0.7 2.8±0.9 0.717
FEV1*/FVC† (%) 47.6±11.1 44.2±13.1 0.119
Acute exacerbation rate 0.5±0.7 0.6±0.7 0.425
P-value LABA/LAMA (N=53) LABA/LAMA/ICS (N=47)
Values are numbers (percentages) for categorical variables and mean±SD for continuous variables
* FEV1: Forced expiratory volume for 1 second
† FVC: Forced vital capacity
았다(Table 3).
또한 3제요법군 중 혈중 호산구수 결과가 확인된 대 상자 42명만을 대상으로 혈중 호산구수에 따른 하위 그룹 분석 결과 두 군간 연간 급성악화 빈도 변화에서 통계적으로 유의한 차이는 없었다(Table 4).
2) 폐기능 변화
폐기능 검사 결과 LABA/LAMA 2제요법군과 LA BA/LAMA/ICS 3제요법군 모두 1년간 흡입제 사 용 후 FEV1, FVC, FEV1/FVC이 통계적으로 유의 하게 향상되었다(Table 5).
1년간 흡입제 사용 후 2제요법군과 3제요법군 간
FEV1(L) 변화량, FVC(L) 변화량, FEV1/FVC(%) 변화량에서 유의한 차이 없었으며(Table 6), 3제요 법군 중 혈중 호산구수에 따른 하위그룹 분석 결과 혈 중 호산구수가 2% 미만인 군에서의 FEV1/FVC(%) 변화량이 혈중 호산구수 2% 이상인 군에 비해 더 높 게 나타났으나 통계적으로 유의한 차이는 보이지 않 았다(Table 7).
3. 안전성 분석
흡입제 사용 후 폐렴 및 기타 부작용 발생 빈도는 LABA/LAMA/ICS 3제요법군에 비해 LABA/LA MA 2제요법군에서 더 많이 발생하였으나 두 군간 통 Table 2 The rate of acute exacerbations in each group
AE† rate 0.5±0.7 0.3±0.7 0.037 0.6±0.7 0.4±0.8 0.146
LABA/LAMA/ICS (N=47) LABA/LAMA (N=53)
Pre*
Pre* Post* P-value Post* P-value
Values are mean±SD for continuous variables.
Data is collected before and after using inhalers which contain LABA/LAMA or LABA/LAMA/ICS for 1 year
*‘Pre’ and ‘post’ mean outcomes before and after using dual therapy or triple therapy
† AE: Acute exacerbation
Values are numbers (percentages) for categorical variables and means(SD) for continuous variables.
*‘Pre’ and ‘post’ mean outcomes before and after using dual therapy or triple therapy
† AE: Acute exacerbation
‡ OCS: Oral corticosteroids
Table 3 The rate of acute exacerbations, hospitalizations, oral corticosteroids or antibiotics prescription for 1 year
Pre* AE† rate 0.5±0.7 0.6±0.7 0.425
Post* AE† rate 0.3±0.7 0.4±0.8 0.403
Change of AE† rate for 1 year -0.2±0.8 -0.2±0.9 0.946
Hospitalization >0.999
None 51 (96.2) 45 (97.8)
≥ 1 2 (3.8) 1 (2.2)
OCS‡ prescription rate 0.1±0.3 0.2±0.6 0.051
Antibiotics prescription rate 0.2±0.6 0.4±0.8 0.372
P-value LABA/LAMA (N=53) LABA/LAMA/ICS (N=47)
Table 5 Pulmonary function test in each group
FEV1† (L) 1.3±0.3 1.4±0.4 <0.001 1.2±0.4 1.4±0.5 <0.001
FVC‡ (L) 2.7±0.7 2.9±0.8 0.001 2.8±0.9 3.1±1.1 0.005
FEV1†/FVC‡ (%) 47.6±11.1 49.7±11.4 0.047 44.2±13.1 47.7±13.0 0.001 LABA/LAMA/ICS (N=47) LABA/LAMA (N=53)
Pre*
Pre* Post* P-value Post* P-value
Values are mean±SD for continuous variables.
Data is collected before and after using inhalers which contain LABA/LAMA or LABA/LAMA/ICS for 1 year
*‘Pre’ and ‘post’ mean outcomes before and after using dual therapy or triple therapy.
† FEV1: Forced expiratory volume for 1 second; ‡ FVC: Forced vital capacity Values are mean±SD for continuous variables
*‘Pre’ and ‘post’ mean outcomes before and after using dual therapy or triple therapy
†AE: Acute exacerbation
Values are mean±SD for continuous variables
*‘Pre’ and ‘post’ mean outcomes before and after using dual therapy or triple therapy.
† FEV1: Forced expiratory volume for 1 second; ‡FVC: Forced vital capacity
Table 4 The rate of acute exacerbations in triple therapy inhaler sub-group according to eosinophil count
Table 6 Pulmonary function test after 1 year
Pre* AE† rate 1.0±0.8 0.4±0.6 0.014
Post* AE† rate 0.4±0.8 0.4±0.7 0.830
Change of AE† rate for 1 year -0.6±0.9 -0.1±0.9 0.074
Pre* pulmonary function test
FEV1† (L) 1.3±0.3 1.2±0.4 0.243
FVC‡ (L) 2.7±0.7 2.8±0.9 0.717
FEV1†/FVC‡ (%) 47.6±11.1 44.2±13.1 0.119
Post* pulmonary function test
FEV1† (L) 1.4±0.4 1.4±0.5 0.863
FVC‡ (L) 2.9±0.8 3.1±1.1 0.822
FEV1†/FVC‡ (%) 49.7±11.4 47.7±13.0 0.564
Change of pulmonary function test for 1 year
FEV1† (L) 0.2±0.2 0.2±0.4 0.388
FVC‡ (L) 0.2±0.4 0.3±0.6 0.825
FEV1†/FVC‡ (%) 2.1±7.1 3.5±6.5 0.212
P-value
P-value Eosinophil <2% (N=14)
LABA/LAMA (N=53)
Eosinophil ≥2% (N=28)
LABA/LAMA/ICS (N=47)
계적으로 유의한 차이는 없었다(Table 8).
고찰 및 결론
COPD는 기류 제한을 특징으로 하는 폐질환으로 국 내외 가이드라인에 따르면 흡입용 기관지확장제 치료 를 일차적으로 권장한다.1),2) 이러한 COPD 환자에 게 일반적으로 ICS의 단독 사용은 권장되지 않으나 천식이 동반된 중복 증후군(Asthma-COPD over- lap syndrome, ACOS) 환자나 중등도 이상의 COPD 환자에서의 ICS 병용은 환자의 폐기능과 삶 의 질을 향상시키고 급성악화 빈도를 감소시킬 수 있 는 것으로 제시하고 있다. LABA/LAMA/ICS 3제 요법군과 LABA/LAMA 2제요법군의 효과 및 안전 성을 비교한 기존의 IMPACT 연구와 TRIBUTE 연 구에서는 3제요법군이 2제요법군에 비해 연간 중등
도 이상의 급성악화 빈도를 유의하게 감소시키고, 폐 기능에서도 개선을 보이는 것으로 나타났으나 폐렴 발생 빈도에서는 3제요법군에서 폐렴 발생 빈도가 증 가되는 것으로 나타난 IMPACT 연구와는 달리 TRIBUTE 연구에서는 증가시키지 않는 것으로 나 타나 서로 다른 결과가 제시되었다.3),4) 본 연구에서 는 1년간 흡입제 사용 후 두 군간의 연간 급성악화 빈 도에서 통계적으로 유의한 차이는 확인할 수 없었다.
즉, ICS의 병용이 급성악화의 빈도를 감소시키지는 않는 것으로 나타났으나 본 연구가 환자에게 사용한 흡입제 성분이나 용량에 제한을 두지 않았으며, 이전 사용하던 흡입제의 영향 및 후향적 의무기록 연구로 급성악화 정보 수집이나 COPD의 악화와 폐기능 결 과에 영향을 미칠 수 있는 흡입제 사용 순응도는 파악 할 수 없었던 점에서 그 한계가 있다.
또한 최근 연구에서 ICS 병용이 혈중 호산구수가 높
Values are mean±SD for continuous variables
* FEV1: Forced expiratory volume for 1 second
† FVC: Forced vital capacity
Values are numbers (percentages) for categorical variables
Table 7 Change of pulmonary function test for 1 year in triple therapy inhaler sub-group according to eosinophil count
FEV1* (L) 0.3±0.3 0.2±0.4 0.575
FVC† (L) 0.4±0.5 0.3±0.6 0.330
FEV1*/FVC† (%) 3.7±4.6 2.3±6.3 0.457
P-value Eosinophil <2% (N=14) Eosinophil ≥2% (N=28)
Table 8 Pneumonia and other adverse drug reactions for 1 year
Pneumonia 4 (7.5) 2 (4.3) 0.681
Other adverse drug reactions 6 (11.3) 2 (4.3) 0.276
Dry mouth 4 1
Sore throat 0 2
Cough 1 0
Dizziness 1 0
Tremor 0 1
P-value LABA/LAMA (N=53) LABA/LAMA/ICS (N=47)
은 환자에게서 급성악화를 예방하는데 효과가 있음을 나타내고 있으며,10),11) 최근 발표된 GOLD (Global initiative for obstructive lung disease) 2019 report에서도 혈중 호산구수가 300 cells/
μL 이상인 경우 또는 LABA/LAMA를 사용하면서 혈중 호산구수가 100 cells/μL 이상이며 악화 위험 이 높은 경우 ICS 병용 시 급성악화 예방 가능성을 제 시하고 있다.12) 본 연구가 진행된 당시에는 GOLD 2019 report가 발표되기 전으로 GOLD 2018 re- port에서는 별도의 혈중 호산구수가 제시되어 있지 않아 기존의 연구들을 바탕으로 혈중 호산구수 2%를 기준으로 ICS사용에 따른 급성악화 빈도 차이를 비 교하였으며,7),9),11) 연구 결과 혈중 호산구수 2% 미 만인 군에서 급성악화 빈도가 더 감소한 것으로 나타 났으나 통계적으로 유의한 차이는 없었으며, 이는 혈 중 호산구수 2% 미만인 군의 흡입제 사용 전 급성악 화 빈도가 혈중 호산구수 2% 이상인 군에 비해 유의 하게 높았던 점의 영향을 배제할 수 없을 것으로 사료 된다. 본 연구에서는 혈중 호산구수 2%를 기준으로 ICS의 급성악화 빈도 예방 효과를 분석하였으나, GOLD 2019 report 및 다른 연구들에서 혈중 호산 구수가 300 cells/μL 또는 4% 이상의 높은 호산구 수를 보이는 환자에서 급성악화 예방 효과가 있다는 결과들이 발표되고 있어 이에 대한 후속연구가 필요 할 것이다.11),13),14)
LABA/LAMA 2제요법군과 LABA/LAMA/ICS 3제요법군 모두 1년간 흡입제 사용 후 FEV1 (L), FVC (L), FEV1/FVC (%)이 통계적으로 유의하게 향상되었으나 두 군간의 유의한 차이는 없었다. 다만 통계적으로 유의한 차이는 없었으나 3제요법군의 기 저 FEV1 수치가 2제요법군보다 낮은 경향을 보였던 것을 고려할 때 3제요법군에서 FEV1이 더 많이 향상 된 것을 확인할 수 있었다.
COPD 환자에서 기관지확장제와 병용하여 ICS를 사용하는 것은 급성악화의 위험을 감소시키는 반면 폐렴 발생 위험 증가 가능성 있는 것으로 보고되고 있
으나,5),10) 일부 연구에서는 ICS를 병용했을 때 폐렴
발생 위험이 증가되지 않는다는 결과가 보고되고 있 다.4) 본 연구에서는 LABA/LAMA/ICS 3제요법군 에 비해 LABA/LAMA 2제요법군에서 폐렴이 더 많 이 발생한 것으로 나타났으나 두 군간 통계적으로 유
의한 차이는 없었다. 즉, ICS의 병용이 폐렴 발생 위 험을 증가시키지는 않는 것으로 나타났으나 이는 2제 요법군 환자의 평균연령이 3제요법군보다 유의하게 높았던 인구학적 특성 차이에 의한 영향을 배제할 수 없을 것으로 사료된다.
본 연구 결과, 중등도 이상의 COPD 환자에서 LA BA/LAMA/ICS 3제요법이 LABA/LAMA 2제요 법에 비해 연간 급성악화 빈도를 유의하게 감소시키 지는 않았으나, ICS 병용에 따른 폐렴 발생 등 부작 용 발생 측면에서도 증가를 보이지 않았다. 다만 유의 하지는 않았으나 3제요법군에서 FEV1/FVC (%)이 2제요법군에 비해 더 많이 향상되었으며, 3제요법군 의 기저 FEV1 수치가 2제요법군에 비해 낮았던 점을 고려할 때 중등도 이상의 COPD 환자 중 FEV1 수치 가 낮은 환자에서 LABA/LAMA/ICS 3제요법을 초 기부터 고려해 볼 수도 있을 것으로 사료되며, 차후 본 연구의 한계점을 보완하여 이에 대한 추가적인 연 구가 필요할 것으로 판단된다.
참고문헌
1) The Korean Academy of Tuberculosis and Respiratory Diseases: COPD Guide- line Revision Committee. COPD Clinical Practice Guidelines, updated 2018. https:
//www.lungkorea.org/
2) Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Dis- ease (2018 Report). http://goldcopd.
org/gold-reports/
3) Lipson DA, Barnhart F, Brealey N et al.
Once-Daily Single-Inhaler Triple versus Dual Therapy in Patients with COPD.
The New England journal of medicine.
2018;378(18):1671-80.
4) Papi A, Vestbo J, Fabbri L et al. Extraf- ine inhaled triple therapy versus dual bronchodilator therapy in chronic ob- structive pulmonary disease (TRIBUTE):
a double-blind, parallel group, rando- mised controlled trial. Lancet (London, England). 2018;391(10125):1076-84.
5) Yang IA, Clarke MS, Sim EH et al. In- haled corticosteroids for stable chronic obstructive pulmonary disease. The Co- chrane database of systematic reviews.
2012(7):Cd002991.
6) Crim C, Calverley PMA, Anderson JA et al. Pneumonia risk with inhaled flutica- sone furoate and vilanterol in COPD pa- tients with moderate airflow limitation:
The SUMMIT trial. Respiratory medi- cine. 2017;131:27-34.
7) Bafadhel M, Peterson S, De Blas MA et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease:
a post-hoc analysis of three randomised trials. The Lancet Respiratory medicine.
2018;6(2):117-26.
8) Kerkhof M, Sonnappa S, Postma DS et al. Blood eosinophil count and exacerba- tion risk in patients with COPD. The Eu- ropean respiratory journal. 2017;50(1).
9) Cheng SL. Blood eosinophils and inhaled corticosteroids in patients with COPD:
systematic review and meta-analysis.
International journal of chronic obstruc- tive pulmonary disease. 2018;13:2775- 84.
10) Oh YM, Lee KS, Hong Y et al. Blood eo- sinophil count as a prognostic biomark- er in COPD. International journal of chronic obstructive pulmonary disease.
2018;13:3589-96.
11) Yun JH, Lamb A, Chase R et al. Blood eosinophil count thresholds and exac- erbations in patients with chronic ob- structive pulmonary disease. The Jour- nal of allergy and clinical immunology.
2018;141(6):2037-47.
12) Global Initiative for Chronic Obstruc- tive Lung Disease. Global Strategy for the Diagnosis, Management, and Pre- vention of Chronic Obstructive Pulmo- nary Disease (2019 report). http://gold copd.org/gold-reports/
13) Watz H, Tetzlaff K, Wouters EF et al.
Blood eosinophil count and exacerba- tions in severe chronic obstructive pul- monary disease after withdrawal of in- haled corticosteroids: a post-hoc ana- lysis of the WISDOM trial. The Lancet Respiratory Medicine. 2016;4(5):390-8.
14) Oshagbemi OA, Odiba JO, Daniel A et al. Absolute Blood Eosinophil Counts to Guide Inhaled Corticosteroids Therapy Among Patients with COPD: Systemat- ic Review and Meta-analysis. Current Drug Targets. 2019;20(16):1670-9.