105
책임저자:한덕종, 서울시 송파구 풍납동 388-1
울산대학교 의과대학 서울아산병원 외과, 138-736 Tel: 02-3010-3480, Fax: 02-474-9027
E-mail: [email protected]
본 논문의 내용은 2006년 대한이식학회 추계학술대회에서 구연 되었음.
Analysis of Long Term Follow Up Result be- tween Cycolosporine Based Azathioprine ver- sus Mycophenolate Mofetil Groups Randomized after Renal Transplant
Yo Han Park, M.D., Kwan Tae Park, M.D., Song Cheol Kim, M.D. and Duck Jong Han, M.D.
Department of Surgery, Ulsan University College of Medicine and Asan Medical Center, Seoul, Korea
Purpose: Mycophenolate mofetil (MMF) has been used widely due to lesser acute rejection episode, better renal function and graft survival than azathioprine (AZA). But currently, there is controversy that which combination of im- munosuppressants is most beneficial and cost-effective for renal transplant, because some authors reported MMF was related to more infectious complications and no actual su- periority to AZA in aspect of graft survival. So, the aims of this study is to compare the long term outcome of renal transplants and the infectious complications between two groups treated with AZA and MMF in CSA based im- munosuppressant treatment at our hospital. Methods: We retrospectively reviewed allograft recipients who had been transplanted from January of 1998 to July of 2000. 301 patients were enrolled (AZA=150/MMF=151) and analyzed for the incidence of acute rejection, infectious complication, renal function and graft survival. Results: Patients treated with MMF had fewer episodes of acute rejection (AR) within 3 months; 4/151 (2.6%) in MMF versus 15/150 (10%) in AZA (P=0.017), but after 3 months there was no difference in the incidence of AR. However, the patients treated with MMF
had more infectious complications such as pneumonia, cyto- megalovirus (CMV) infection, but there were no differences in urinary tract infection. There were also no differences in crea- tinine level at postoperative 1 week, discharge, 1 year, 3 year and 5 year. Graft survival and patient survival after 1 year and 5 showed no statistical differences between two groups. Con- clusion: MMF combined with CsA was more effective in the prevention of acute rejection within 3 months than AZA, but there was no long term significant difference in renal function, graft and patient's survival. Due to higher incidence of pneu- monia and CMV infection in MMF group, it is necessary to choose the combination of immunosuppressants (AZA versus MMF) more appropriately considering efficacy of immuno- suppression and infectious complication as well. (J Korean Soc Transplant 2007;21:105-110)
Key Words: Renal transplant, Azathioprine (AZA), Myco- phenolate mofetil (MMF)
중심 단어: 신이식, Azathioprine (AZA), Mycophenolate mofetil (MMF)
신 이식 후 무작위로 배정된 Azathioprine과 Mycophenolate Mofetil 투여군의 이식성적 비교: 장기 추적 결과
울산대학교 의과대학 서울아산병원 외과 박요한․박관태․김송철․한덕종
서 론
Mycophenolate mofetil (MMF)와 Azathioprine (AZA)은 같 은 항대사산물계열의 면역 억제제로 세포증식에 필요한 DNA 합성에 필수적인 퓨린 합성을 억제하여 T 및 B 림프 구의 증식을 억제한다.(1) MMF는 체내에서 mycophenoleic acid (MPA)로 대사되어 퓨린합성을 선택적으로 억제하며, 특히 활성 T 및 B 림프구에서 발현되는 inosine mono- phosphate dehydrogenase (IMPDH)를 가역적으로 억제하여, 림프구의 증식을 조혈작용 억제의 부작용 없이 선택적으로 억제한다.(2) 즉, MMF는 AZA에 비해 부작용은 적고 좀 더 강력한 면역억제제로 개발되었고, 1990년대 이후 널리 사 용되고 있다.(3,4) 서구의 여러 문헌에서 MMF가 AZA에 비 해 급성거부반응의 발생을 감소시키고, 이식신의 생존율을 높인다고 보고되었으나,(5-8) 최근들어 MMF가 AZA에 비 해 급성거부반응의 감소나 이식신 생존율 향상에 이점이
Table 1. Donor profile
AZA MMF
P-value*
(n=150) (n=151)
Age 38.91 37.48 0.169
Sex (M:F) 1:0.48 1:0.56 NS
Donor type
Deceased 48 (32%) 47 (31%) NS
Living unrelated 85 (56%) 71 (47%) NS Living related 17 (11%) 33 (21%) NS Creatinine clearance
110±30.29 95,3±31.94 NS (mL/min)
Serum creatinine
1.0±0.47 1.2±0.95 0.068 (mg/dL)
Kidney weight (g) 168.0±37.60 165.4±35.77 0.600 Cold ischemic time
132±191.3 180±232.1 0.093 (min)
*P-value by paired t-test or Chi-square test.
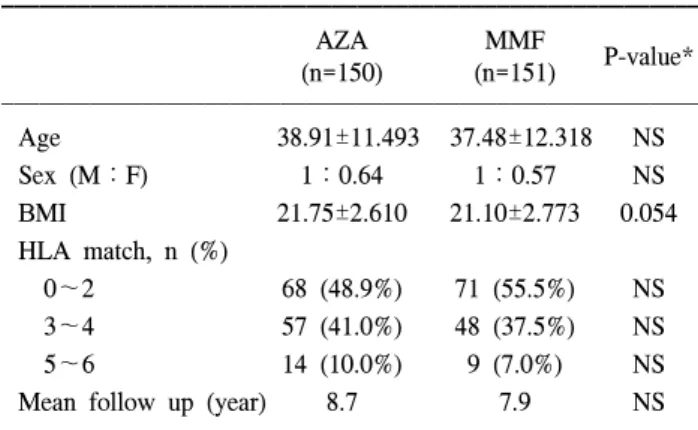
Table 2. Recipient profile
AZA MMF
P-value*
(n=150) (n=151)
Age 38.91±11.493 37.48±12.318 NS
Sex (M:F) 1:0.64 1:0.57 NS
BMI 21.75±2.610 21.10±2.773 0.054
HLA match, n (%)
0~2 68 (48.9%) 71 (55.5%) NS
3~4 57 (41.0%) 48 (37.5%) NS
5~6 14 (10.0%) 9 (7.0%) NS
Mean follow up (year) 8.7 7.9 NS
BMI = body mass index. *P-value by paired t-test or Chi-square test.
없고,(3,9) 도리어 cytomegalovirus (CMV)감염과 같은 심각 한 감염 합병증의 빈도가 높다는 보고도 있다.(10,11) 이에 저자들은 MMF가 도입되던 시기에 무작위로 배정되어 MMF와 AZA를 사용했던 환자군의 장기 추적한 이식성적 을 비교하여 더 효과적인 면역억제제의 사용에 대해 연구 해 보고자 하였다.
방 법
1) 대상 환자의 선택 및 면역 억제제의 사용
1998년 1월부터 2000년 6월까지 서울아산병원 외과에서 신이식술을 시행 받은 환자 중, 재이식환자, PRA 30% 이상 의 환자, ABO minor mismatch 환자를 제외하고, 추적기간 중 면역억제제가 변경된 환자도 제외하고, cyclosporine (CsA)를 기본으로 하여 MMF 혹은 AZA를 병용한 301명을 대상으로 하였다. 동일 기간에 이식을 받은 301명의 환자는 MMF군 혹은 AZA군에 무작위로 배정되었으며, MMF군이 151예 AZA군이 150예로, 양군에서 모두 CsA은 이식 2일 전 5 mg/kg를 하루 두 번 경구 복용한 후 수술 당일에는 1.7 mg/kg씩 경정맥으로 2회 투여하였으며 수술 후 1일째부 터는 경구로 투여하였다. Prednisolone은 양군에서 모두 이 식 2일 전부터 10 mg을 하루 두 번 복용하였으며 이식 당일 에는 methyl prednisolone 500 mg을 정주하였고 이식 후 3일 째까지 반감하여 4일째부터는 경구 투여하였다. MMF는 체 중에 따라 하루 1.5~2 g을 사용하였고, AZA는 하루 50~75 mg의 용량으로 투여하였다. CsA의 12시간 혈중 최저농도 는 수술 초기에는 250 ng/mL 전후로, 유지기에는 100~150 ng/mL로 유지하였다.
2) 연구 방법 및 내용
양군간의 성별, 연령, HLA 항원적합도, 공여자 종류의 정 도를 비교하였다. 이식 후 신기능은 이식 후 1주, 최초 퇴원 시, 1년, 3년, 5년의 혈청 크레아티닌치를 비교하였다. 급성 거부반응의 진단은 지속적인 혈청 크레아티닌치의 상승, 요량의 감소, 단백뇨 등의 임상 소견과 신주사스캔 등의 검 사소견에서 급성 거부반응이 의심되는 경우를 임상적 거부 반응으로, 조직생검을 통해 확진된 경우를 조직생검상 거 부반응으로 각각 분류하였고, 스테로이드 충격요법을 사용 한 경우를 거부반응으로 인정하였다.
퇴원 후의 CsA 혈중 농도 및 용량, 크레아티닌치, 기타 검사 소견, 감염 발생 여부는 외래 임상 기록을 통해 관찰 하였으며, 양군간의 빈도나 수치의 차이는 Chi-square test와 t-test로 유의 수준 0.05 미만으로 검증하였으며 이식신과 환 자의 생존율은 Kaplan-Meier방법으로 구하였다.
결 과
1) 대상 환자의 특성
이식 공여자의 특성은 AZA군이 39.9세 MMF군이 37.5세 였다. 남녀비는 AZA군에서 1:0.48 MMF군에서 1:0.56 으 로 통계상 유의한 차이는 없었다. AZA군에서 크레아티닌 청소율은 110.0±30.29 mL/min, 수술 전 크레아티닌은 1.0±
0.47 mg/dL이었으며 MMF군에서는 각각 95.3±31.94 mL/min, 1.2±0.95 mg/dL로 통계적인 차이가 없었다. 공여 자 중 뇌사자 빈도는 AZA군에서 32% (48/150) MMF군에서 31% (47/151)으로 유의한 차이가 없었다(Table 1). 이식 수 혜자의 평균 연령은 AZA군이 38.9세 MMF군이 37.5세였고 남녀비는 각각 1:0.64. 1:0.57로 양군간 통계적인 차이는 없었다. HLA 항원의 적합도, CMV IgG 음성환자수, 평균 추적기간도 양군간 차이가 없었다(Table 2).
Table 3. Mean serum creatinine after transplantation
AZA MMF
P-value*
(n=150) (n=151)
1 week (mg/dL) 1.36±0.842 1.37±1.161 0.944 At discharge (mg/dL) 1.21±0.524 1.26±0.523 0.512 1 year (mg/dL) 1.37±0.721 1.33±1.048 0.733 3 year (mg/dL) 1.41±0.683 1.48±1.013 0.488 5 year (mg/dL) 1.69±1.597 1.59±1.234 0.563
*P-value by paired t-test.
Table 4. Acute rejection after transplantation
AZA (n=150) MMF (n=151)
P-value*
Clinical Clinical
BPAR Total BPAR Total
AR AR
Within 3 month 3 15 18 (12%) 6 4 10 (2.6%) 0.019
Within 1 year 0 6 6 (4%) 2 3 5 (2.3%) 0.308
After 1 year 5 13 18 (12%) 0 14 14 (9.3%) 0.414
AR = acute rejection; BPAR = biopsy proven acute rejection. *P-value for total incidence of AR by Chi-square test.
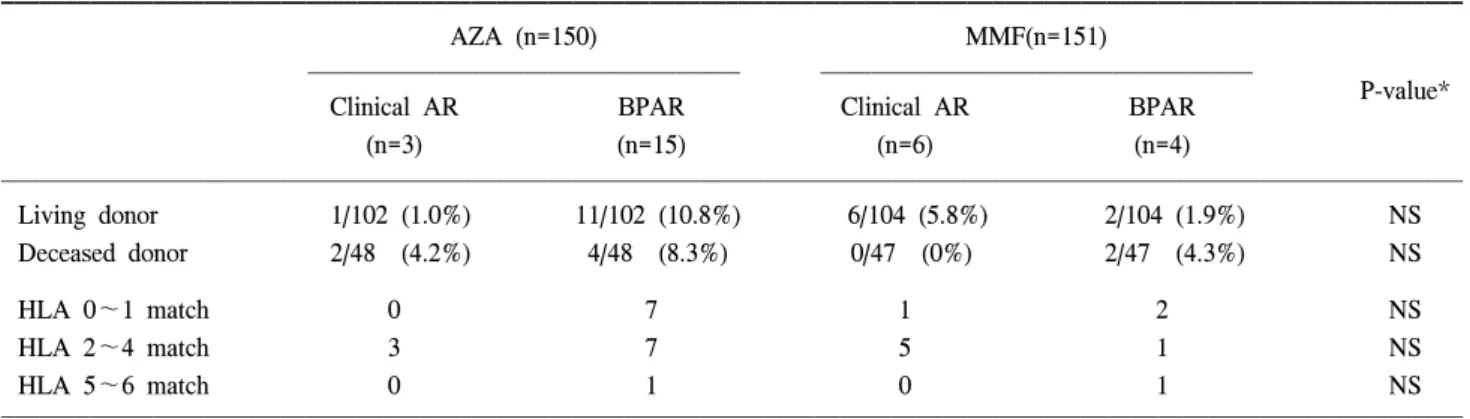
Table 5. Acute rejection within posttransplant 3 months by donor type and HLA match
AZA (n=150) MMF(n=151)
P-value*
Clinical AR BPAR Clinical AR BPAR
(n=3) (n=15) (n=6) (n=4)
Living donor 1/102 (1.0%) 11/102 (10.8%) 6/104 (5.8%) 2/104 (1.9%) NS Deceased donor 2/48 (4.2%) 4/48 (8.3%) 0/47 (0%) 2/47 (4.3%) NS
HLA 0~1 match 0 7 1 2 NS
HLA 2~4 match 3 7 5 1 NS
HLA 5~6 match 0 1 0 1 NS
*P-value by Chi-square test.
2) 이식신의 기능
양군간 이식 후 1주 및 퇴원시점 그리고 각각 1년, 3년, 5년 의 크레아티닌치를 비교하였다. 퇴원 시 크레아티닌은 AZA 군에서 1.21±0.524 mg/dL MMF군에서 1.37±0.523 mg/dL, 1년, 3년 그리고 5년째에 크레아티닌은 AZA군에서 1.37±
0.721 mg/dL, 1.41±0.683 mg/dL, 1.69±1.597 mg/dL 그리고 MMF군에서 1.33±1.048 mg/dL, 1.48±1.013 mg/dL, 1.59±
1.234 mg/dL로 두 집단의 통계적 차이는 없었다(Table 3).
3) 급성거부반응의 발생 빈도
3개월 이내의 급성거부반응은 AZA군에서 임상적 거부 반응과 조직생검상 거부반응이 각각 3예, 15예로 총 18예 (12%)에서 발생하였으며, MMF군에서는 임상적 거부반응 과 조직생검상 거부반응이 각각 6예, 4예로 총 10예(6.6%) 에서 발생하여 AZA군이 유의하게 그 발생 빈도가 높았다 (P=0.017). 이식 후 3개월에서 1년 이내의 거부반응은 전체 발생 빈도는 6예(4%)와 5예로 차이가 없었으나, 조직생검 상 거부반응이 AZA군에서 6예(4%)로 MMF군의 3예(2%)보 다 많았으나 통계적 유의성은 없었다. 1년 이후의 거부반응 은 AZA군이 임상적 거부반응과 조직생검상 거부반응이 각 각 5예, 13예로 총 18예(12%), MMF군이 각각 0예, 14예로 총 14예(9.3%)에서 발생하여 양군간 차이가 없었다(Table 4).
3개월 이내의 거부반응을 공여자 종류별, HLA 적합도별 로 나누어 분석하였으나, 어떠한 통계적 유의성도 발견할 수 없었다(Table 5).
4) 환자 및 이식편 생존율
1년과 5년째에 환자 및 이식편 생존율 모두 MMF군이 미 미하게 양호한 성적을 보이나, 통계적 유의성은 없었다
Table 6. Graft and patient survival by 1 and 5 year
AZA (%) MMF (%) P-value*
Patient survival 1 year 93.3 97.3
0.060
5 year 89.3 95.3
Graft survival 1 year 92.0 96.0
0.139
5 year 81.9 86.0
*P-value by log rank test.
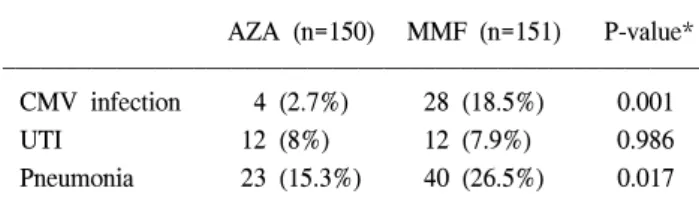
Table 7. Infectious complication after transplantation
AZA (n=150) MMF (n=151) P-value*
CMV infection 4 (2.7%) 28 (18.5%) 0.001
UTI 12 (8%) 12 (7.9%) 0.986
Pneumonia 23 (15.3%) 40 (26.5%) 0.017
UTI = urinary tract infection. *P-value by Chi-square test.
(Table 6)(P=0.06, 0.139, log rank test).
5) 기회감염
신이식 후 가장 흔히 문제가 되는 폐렴, 요로감염, CMV 감염에 대해 양군을 비교하였다. 폐렴은 호흡기 증상 및 흉 부 방사선 사진의 변화 또는 객담에서 의미 있는 균주가 동정된 경우로 제한하였으며, 요로감염은 임상 증상 및 소 변 검사 결과, 그리고 소변 검체에서 균주가 자란 경우로 간주하였다. CMV 감염은 임상 증상 및 CMV 항원혈증이 양성인 경우로 제한하였다. 폐렴은 AZA군에서 23예(15.3%) MMF군에서 40예(26.5%)로 통계적으로 유의한 차이를 보 였으나(P=0.017), 요로감염은 AZA군에서 12예(8%) MMF군 에서 12예(8%)로 차이를 보이지 않았다. CMV 감염은 AZA 군에서 4예(2.7%), MMF군에서 28예(18.5%)로 통계적으로 유의하게 MMF군에서 많이 발생하였다(Table 7)(P=0.001).
고 찰
1970년대 CsA이 사용된 후 이식신의 생존율이 크게 증가 향상되었으나, 신독성, 고지혈증, 고혈압 그리고 혈당 상승 등의 부작용이 문제가 되었고,(12) 이는 다른 면역억제제인 AZA와 prednisolone과의 병합 요법으로 어느 정도 극복할 수 있었다. 이후 90년대에 MMF가 소개되면서 MMF는 기 존의 AZA에 비해 급성 거부반응의 빈도를 낮출 수 있는 면역억제제로 알려졌다.(8)
MMF는 MPA의 전구약물로써 경구 투여 후 체내에서 MPA로 전환되어 작용을 나타낸다. 생체 내 퓨린 합성 경로 에는 de novo pathway와 salvage pathway가 있으며 MPA는 그 중 de novo pathway에서 IMPDH를 억제하여 inosine monophosphate (IMP)가 guanosine monophosphate로 전환되 는 과정을 억제한다. 림프구는 주로 de novo pathway에 의존 하므로 MPA에 대해 선택적으로 증식이 억제되는 것으로 알려져 있다. 또한 MPA는 GTP를 감소시켜 림프구에서 세 포막 당단백으로 fucose와 mannose의 이동을 감소시켜 adhesion molecule의 당화를 저해함으로 림프구가 target cell 에 부착되는 것을 방해한다.(1,13)
여러 문헌에서는 MMF가 AZA보다 급성 거부반응의 빈
도와 강도를 의미 있게 감소시키고 이에 따른 이식신의 소 실도 감소시킨다고 보고하고 있다.(5-8) 또한 Wuthrich 등 (14)은 급성 거부 반응으로 인한 재입원 및 조직검사 등의 시술에 들어가는 경제적 비용까지 고려하였을 때 MMF가 월등하다는 보고도 있다. 하지만 Remuzzi 등(9)은 급성 거 부 반응을 감소시키나 장기간의 이식편 생존에서는 큰 차 이가 없고, 도리어 비용만 15배 정도로 비싼 이유로 신이식 에서의 표준요법에 MMF 대신 AZA를 사용하자고 제안하 고 있다. 또한, CsA이 예전 SandimmuneⓇ (Novartis, Basel, Switzerland)에서 microemulsion 제제인 NeoralⓇ (Novartis, Basel, Switzerland)로 개량되면서 흡수가 빨라지고, 안정적 이 되면서 NeoralⓇ과 병용했을 때에 MMF가 AZA에 비해 우월한지도 의문이라고 지적한다.(9) 이와 같이, MMF의 안 정성과 효용성에 대해 최근 다양한 연구들이 진행되면서, MMF가 AZA에 비해 거부반응 예방효과가 뛰어난지, 이식 편 생존율 향상에 기여하는지에 대해 혼란이 있고, 그렇다 면 과연 어떤 약제를 병용하는 것이 최상의 조합인가에 대 한 의문이 있는 실정이다. 그런 의미에서, NeoralⓇ과 병용하 여 무작위로 배정된 MMF군과 AZA군을 장기추적하여 비 교하는 것은 의미가 있다고 하겠다. 이 연구에서는 3개월 이내의 급성거부반응 발생률이 AZA군에서 12%, MMF군에 서 6.6%의 환자에서 발생하여 MMF가 유의하게 거부반응 예방에 효과가 있음을 보여준다. 특히, 조직검사로 확진된 거부반응은 양군간 거부반응 발생률이 각각 10%와 2.6%로 더욱 유의한 차이를 보여주나, 본원의 경우 거부반응이 의 심되는 모든 경우에 신생검을 하고, 생검을 할 수 없는 부득 이한 경우에도 임상적으로 거부반응이 강력히 의심되는 경 우에만 스테로이드 충격요법을 사용하기에, 이식 후 초기 에 임상적 거부반응과 조직검사상 거부반응을 나누는 것은 큰 임상적 의미는 없다 하겠다. 또한 5년 추적한 이식편 생존 율과 신기능면에서는 양군간 차이가 없는 결과를 보여준다.
이식 후 기회감염은 치료법의 발달로 감소하는 추세이긴 하나 아직도 신이식 환자의 생존을 위협하는 이유로 남아 있고, 이중에서도 폐렴은 사망을 초래하는 중요 합병증으 로 이식 후 사망환자의 사인의 약 20%을 차지한다.(15) 또 한, CMV 감염은 신이식 후 신기능과 환자의 삶의 질에 중 요한 영향을 미치는데, MMF 사용이 CMV 감염률을 높이지
않는다는 보고도 있고,(16,17) Bernabeu-Wittel 등(11)은 MMF사용군에서 3배 가량 CMV감염이 있다고 보고하였고, Moreso 등(18)은 MMF의 용량에 따라 CMV감염의 빈도가 달라진다고 보고하였다. 이에 대해 국내에서는 보고된 바 가 적은데 최근 이 등(19)은 통계적 유의성은 없으나 도리 어 AZA군에서 CMV감염이 더 높다고 보고하였다. 이와 같 이 CMV감염과 MMF와의 관계에 대해서는 아직까지 논란 이 있는데, 이 연구에서는 2.7%와 18.5%로 유의하게(P=
0.0001) MMF군에서 CMV감염이 많았고, 폐렴 역시 15.3%
와 26.5%로 MMF군에서 발생이 많았다. 본원의 경험이나 많은 문헌의 고찰에 의하면 MMF가 더 높은 CMV 감염률 과 관계가 있다고 보여지고, 이는 MMF의 대사산물인 MPA glucuronide가 글루쿠론산이 분해되어 위장관에서 장관 재 순환을 통해 재흡수되는 과정에서 상부위장관에 MPA의 과 도한 축적을 일으키고, 이로 인한 국소적인 자극으로 위장 관에서 빠르게 분화하는 세포를 방해하여 결과적으로 CMV의 활성화를 가져온다는 가설과 관계가 있다고 보여 진다.(20)
면역억제제 선택에 있어 강한 면역억제능력과 감염증이 라는 부작용을 동시에 생각해 볼 때, MMF와 AZA의 상대 적 효용성에 대해서는 아직 어느 한쪽의 우월성을 단정짓 기는 힘든 상황이다. MMF가 거부반응을 줄이는 데는 이점 이 있으나 장기 추적결과 양군간 신기능에 별차이가 없고, 감염에 있어서는 주요한 감염증인 폐렴과 CMV감염을 높 인다고 한다면, 전체적으로 비용 효용성 면에서 환자의 입 원치료의 필요성 증가 및 감염으로 인한 경제적 손실, 이식 편의 기능 장애를 고려한 재평가가 이루어져야 할 것이다.
이를 위해, 좀더 많은 증례에 대해 전향적인 무작위 배정연 구가 필요하고, 아울러 최근 시행되고 있는 MPA 혈중치 감 시가 MMF로 인한 감염의 증가를 예방할 수 있는지도 향후 연구되어야 할 것이다.
결 론
CsA와 병합 약제로써 MMF는 AZA에 비해 초기 급성 거 부반응의 예방에 효과적이나, 장기적으로는 신기능, 환자 및 이식편 생존율에는 유의한 차이가 없었다. 요로감염에 있어서는 양군간 차이가 없으나 폐렴과 CMV감염률은 MMF군에서 더 높아, 면역억제제의 선택에 있어 면역억제 력과 감염 합병증을 종합적으로 고려하여 신중하게 결정해 야 하겠다. MMF와 AZA의 상대적 효용성에 대해서는 현재 로서는 단정짓기 어려우며, 향후 좀더 많은 증례의 전향적 인 연구가 필요할 것으로 사료된다.
REFERENCES
1) Gerber DA, Bonham CA, Thomson AW. Immunosuppressive
agents: recent developments in molecular action and clinical application. Transplant Proc 1998;30:1573-9.
2) Allison AC, Eugui EM. Mechanisms of action of myco- phenolate mofetil in preventing acute and chronic allograft rejection. Transplantation 2005;80:S181-90.
3) Shah S, Collett D, Johnson R, Thuraisingham RC, Raftery MJ, Rudge CJ, Yaqoob MM. Long-term graft outcome with myco- phenolate mofetil and azathioprine: a paired kidney analysis.
Transplantation 2006;82:1634-9.
4) Vasquez EM, Sifontis NM, Pollak R, Benedetti E. Impact of mycophenolate mofetil on recurrent rejection in kidney trans- plant patients. Clinical Transplantation 2001;15:253-7.
5) European Mycophenolate Mofetil Cooperative Study Group.
Placebo-controlled study of mycophenolate mofetil combined with cyclosporin and corticosteroids for prevention of acute rejection. Lancet 1995;345:1321-5.
6) The Tricontinental Mycophenolate Mofetil Renal Transplan- tation Study Group. A blinded, randomized clinical trial of mycophenolate mofetil for the prevention of acute rejection in cadaveric renal transplantation. Transplantation 1996;61:1029- 37.
7) Sollinger HW. Mycophenolate mofetil for the prevention of acute rejection in primary cadaveric renal allograft recipients.
U.S. Renal Transplant Mycophenolate Mofetil Study Group.
Transplantation 1995;60:225-32.
8) Ojo AO, Meier-Kriesche HU, Hanson JA, Leichtman AB, Cibrik D, Magee JC, Wolfe RA, Agodoa LY, Kaplan B.
Mycophenolate mofetil reduces late renal allograft loss independent of acute rejection. Transplantation 2000;69:2405- 9.
9) Remuzzi G, Lesti M, Gotti E, Ganeva M, Dimitrov BD, Ene-Iordache B, Gherardi G, Donati D, Salvadori M, Sandrini S, Valente U, Segoloni G, Mourad G, Federico S, Rigotti P, Sparacino V, Bosmans JL, Perico N, Ruggenenti P. Mycophe- nolate mofetil versus azathioprine for prevention of acute rejection in renal transplantation (MYSS): a randomised trial.
Lancet 2004;364:503-12.
10) Boucher A, Lord H, Collette S, Morin M, Dandavino R. Cy- tomegalovirus infection in kidney transplant recipients: evo- lution of approach through three eras. Transplant Proc 2006;
38:3506-8.
11) Bernabeu-Wittel M, Naranjo M, Cisneros JM, Canas E, Gentil MA, Algarra G, Pereira P, Gonzalez-Roncero FJ, de Alarcon A, Pachon J. Infections in renal transplant recipients receiving mycophenolate versus azathioprine-based immunosuppression.
Eur J Clin Microbiol Infect Dis 2002;21:173-80.
12) Williams D, Haragsim L. Calcineurin nephrotoxicity. Adv Chronic Kidney Dis 2006;13:47-55.
13) Kamar N, Glander P, Nolting J, Bohler T, Hambach P, Liefeldt L, Neumayer HH, Klupp J, Budde K. Effect of mycophenolate mofetil monotherapy on T-cell functions and inosine monophosphate dehydrogenase activity in patients
undergoing a kidney transplantation. Transplant Proc 2006;38:2292-4.
14) Wuthrich RP, Weinreich T, Ambuhl PM, Schwarzkopf AK, Candinas D, Binswanger U. Reduced kidney transplant rejec- tion rate and pharmacoeconomic advantage of mycophenolate mofetil. Nephrol Dial Transplant 1999;14:394-9.
15) Washer GF, Schroter GP, Starzl TE, Weil R 3rd. Causes of death after kidney transplantation. JAMA 1983;250:49-54.
16) European Mycophenolate Mofetil Cooperative Study Group.
Mycophenolate mofetil in renal transplantation: 3-year results from the placebo-controlled trial. Transplantation 1999;68:
391-6.
17) Halloran P, Mathew T, Tomlanovich S, Groth C, Hooftman L, Barker C. Mycophenolate mofetil in renal allograft reci- pients: a pooled efficacy analysis of three randomized, dou- ble-blind, clinical studies in prevention of rejection. The
International Mycophenolate Mofetil Renal Transplant Study Groups. Transplantation 1997;63:39-47.
18) Moreso F, Seron D, Morales JM, Cruzado JM, Gil-Vernet S, Perez JL, Fulladosa X, Andres A, Grinyo JM. Incidence of leukopenia and cytomegalovirus disease in kidney transplants treated with mycophenolate mofetil combined with low cyclosporine and steroid doses. Clinical Transplantation 1998;
12:198-205.
19) 이재창, 고석환, 오수명, 박호철. 신 이식 후 Azathioprine과 Mycophenolate Mofetil 투여군에서 발생한 감염의 비교. 대한 이식학회지 2005;19:36-41.
20) Kaplan B, Meier-Kriesche HU, Jacobs MG, Friedman G, Bonomini L, DeFranco P, Gelfand E, Mulgaonkar S. Preva- lence of cytomegalovirus in the gastrointestinal tract of renal transplant recipients with persistent abdominal pain. Am J Kidney Dis 1999;34:65-8.