Address reprint requests to Oh Kyung Lim, M.D., Ph.D.
Department of Physical & Rehabilitation Medicine, Gachon University School of Medicine, 1198 Guwol-dong, Namdong-gu 405-760, Korea
TEL: 82-10-2260-3196, Fax: 82-32-460-3722, E-mail : [email protected] 투고일: 2014년 4월 30일, 수정일: 2014년 5월 22일, 게재확정일: 2014년 5월 22일
INTRODUCTION
The spinal accessory nerve (SAN) provides main motor innervations to the trapezius and sternocleidomas- toid muscles. The SAN receives contributions from the second, third, and fourth cervical nerves, and may be injured at any point along its course.
1In the posterior
cervical region, the SAN has a long and superficial course, and is especially susceptible to injury during neck surgery or lymph node dissection, and to blunt direct trauma to the lateral neck.
2Whiplash injuries resulting from motor vehicle acci- dents are very common.
3Some patients with whiplash injury demonstrate irritation of the brachial plexus,
편타손상 후 발생한 지연성 부 척수신경병증 - 증례보고 -
가천의과대학교 재활의학교실
이진영∙윤진원∙이주강∙박기덕∙임오경
– Abstract –
Delayed Unilateral Spinal Accessory Neuropathy after Whiplash Injury - A case report -
Jin Young Lee, M.D., Jin Won Yoon, M.D., Ju Kang Lee, M.D., Ph.D., Ki Deok Park, M.D., Ph.D, Oh Kyung Lim, M.D., Ph.D.
Physical & Rehabilitation Medicine, Gachon University School of Medicine
Unilateral spinal accessory nerve (SAN) palsy is an uncommon pure motor mononeuropathy. Branches of the SAN innervate the sternocleidomastoid and trapezius muscles. Here, the authors describe the case of a 48-year-old man who presented with left shoulder discomfort with shoulder girdle muscle atrophy after a traffic accident. No limitation in any direction was observed in active or passive range of neck motion. How- ever, the patient presented with left shoulder motor weakness on flexion and abduction and limitation of motion; he complained of shoulder pain during forward flexion, abduction, and external rotation. On physi- cal examination, there were no pathologic reflexes, but the patient complained of a tingling sensation in left shoulder concurrent with atrophic sternocleidomastoid and trapezius muscles.
An electrodiagnostic study revealed evidence of a unilateral left spinal accessory nerve lesion. The authors report a rare case of isolated unilateral spinal accessory nerve palsy with delayed shoulder pain after whiplash injury.
Key Words: Spinal accessory nerve palsy, Whiplash injury, Winging scapula
resulting in pain and discomfort of the shoulder and upper limb without abnormal images, but in such cases, MRI and CT findings are usually normal.
4We report the case of a patient with delayed unilateral spinal accessory nerve lesion resulting from whiplash injury. Although, SAN palsy following traumatic stretch injury has been widely reported and has a major detri- mental impact on the functional performance of the shoulder girdle, our patient demonstrated progressive unilateral shoulder pain with limitation of motion during 14 months. This is the first report of such a case to be issued in Korea.
CASE REPORT
Our patient, a 48-year-old male, was struck from behind by another vehicle while his car was stationary.
Resultantly, his head was forced backward and then for- ward. He had not noticed any symptoms immediately after the crash, but one month later experienced mild posterior neck and left shoulder pain. Fourteen months after the incident, he presented at a clinic complaining of posterior neck, upper back, and shoulder pain with motor weakness. An X-ray of the cervical spine was normal, and he was treated with physiotherapy and analgesics.
Despite treatment for a year, he complained of pain of the left upper back radiating to his left shoulder that was aggravated by sitting or standing without using hands and by overhead shoulder activities. He also mentioned volume asymmetry of his shoulders and a reduced active range of motion. In addition, he complained of sleep dis- turbance and interference of active exercise by disabili-
ties of his left shoulder due to motor weakness.
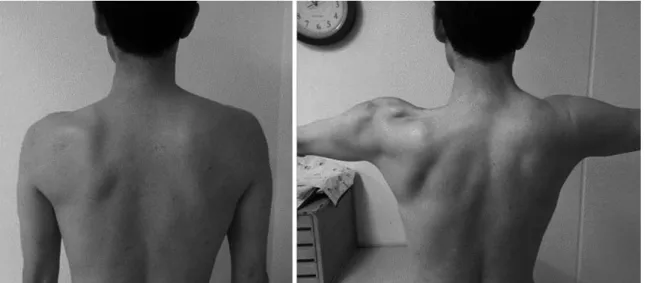
Inspection revealed lateral displacement of the left scapula and atrophic sternomastoid and trapezius mus- cles at our clinic. Active range of motion testing of neck lateral rotation and of left shoulder adduction and poste- rior extension were near normal with end-point pain. The lateral border of the left scapula was more prominent than the right (Fig. 1). He had lost passive movement of the shoulder and pain during abduction and external rota- tion was extremely aggravated. Manual motor testing revealed weakness of the left trapezius and sternomas- toid muscles; his left shoulder flexion and abduction motor grade was IV. A sensory examination of the poste- rior neck and left upper extremity revealed no sensory changes from the posterior neck to upper shoulder.
Conventional axial CT of the cervical spine revealed no abnormal lesions, and thus, a further imaging study was performed on the cranio-cervical junction. Cervical MR studies demonstrated cervico-brachial plexus injury in the infraclavicular area, and a high intensity lesion in his shoulder on T2 weighted images suggested injuries to its branches (Fig. 2-A). In addition, shoulder MR images displayed atrophy of the infraspinatus, supraspinatous, and sternomastoid muscles (Fig. 2-B).
A nerve conduction study (NCS) of the left SAN, with surface stimulation along the posterior border of the ster- nocleidomastoid muscle, and recordings of the upper trapezius, revealed compound muscle action potentials (CMAP) of lower amplitude and delayed latency as com- pared with the right side (0.4mV vs. 9.1mV). Further- more, there no CMAP were observed in middle and lower trapezius (Table 1). The sensory nerve action
Fig. 1. Winging scapula and trapezius muscle atrophy in the left shoulder.
potentials of the left greater auricular nerve and other brachial plexus branches were in normal ranges (Table 1). A needle electromyographic study showed abnormal spontaneous activities, such as, positive sharp waves, fibrillation potentials with polyphasic motor unit poten- tials, and reduced recruitment in the left trapezius and sternocleidomastoid muscles (Table 2). There were no abnormalities of CMAP and needle electromyographic studies in the infraspinatus and supraspinatus muscle, so suprascapular nerve was revealed intact (Table 2). These
findings were consistent with SAN palsy proximal to the innervation site of the sternocleidomastoid muscle.
The clinical impression was of left SAN palsy with delayed shoulder pain. Ultrasonography was performed to assess shoulder pathology, and showed thickening of the joint capsule in the rotator cuff interval and oblitera- tion of the angle under the coracoid process (Fig. 3).
These sonographic findings and clinical evidence were highly suggestive of secondary adhesive capsulitis.
5The patient was treated with by sonography-guided
Table 1. Nerve Conduction Study Compound Motor Action Potential
Stimulation Site Recording Site Onset Latency (ms) Amplitude (mV)
Lt spinal accessory nerve upper trapezius 3.55 20.4
middle trapezius No response
lower trapezius No response
Rt spinal accessory nerve upper trapezius 2.10 29.1
middle trapezius 2.90 26.1
lower trapezius 5.35 23.9
Lt scapular nerve Infraspinatus 2.30 26.2
Supraspinatus 2.25 25.6
Rt scapular nerve Infraspinatus 2.90 39.5
Supraspinatus 2.85 24.0
Sensory Nerve Action Potential
Stimulation Site Recording Site Peak Latency (ms) Amplitude (μV)
Lt greater auricular nerve Ear 1.95 31.7
Rt greater auricular nerve Ear 2.20 33.0
Lt median 2nd digit 3.05 35.4
Rt median 2nd digit 3.05 41.2
Lt ulnar 5th digit 3.15 33.2
Rt ulnar 5th digit 2.90 32.1
Lt Musculocutaneous - lateral branch Forearm 2.35 44.2
Lt Musculocutaneous - medial branch Forearm 2.45 27.3
Rt Musculocutaneous - lateral branch Forearm 2.40 45.0
Rt Musculocutaneous - medial branch Forearm 2.55 30.9
Fig. 2. Magnetic resonance T2 weighted images showing a focal high signal intensity lesion (arrow) in posterior por- tion of infraclavicular area of the cervicobrachial plexus (A) and muscle atrophy of the trapezius muscle (B).
A B
steroid injection into the glenohumeral intra-articular space and physical therapy involving strength and range of motion exercises. After 5 months of follow up, his pain improved partially from visual analog scale 8/10 to 4/10 and the progressive motor weakness was not aggra- vated.
DISCUSSION
Our case demonstrates SAN palsy presented shoulder pain 14 months after a traffic accident without history of surgical procedure or additional trauma. Physical exami- nation revealed the affected shoulder was lower than the normal contralateral shoulder. In addition, atrophy of the trapezius and sternocleidomastoid muscles and a winged scapula were detected.
The spinal accessory nerve (SAN) is consists of cranial and spinal portions. The cranial root arises from the cau- dal segment of the nucleus ambiguous and runs laterally toward the jugular foramen to join the spinal root. It innervates the trapezius and sternocleidomastoid mus-
cles, which stabilize the scapula and shoulder. So, SAN palsy may lead to dysfunction of the trapezius muscle, resulting in drooping of the shoulder, asymmetry of the neckline, downward rotation and protraction of the scapula, and weakness of shoulder movement.
6Further- more, some clinical cases have been reported to exhibit complete transection of the SAN and the greater auricu- lar nerve because the sensory branches of the greater auricular are derived from the same cervical plexus.
6Therefore, the determination of greater auricular nerve patency is important during the diagnosis of SAN injury.
In our patient, electrodiagnostic studies confirmed an intact greater auricular nerve (Table 1), and the location of SAN injury was at the neck posterior triangle on the posterior border of sternocleidomastoid muscle after the emergence of the greater auricular nerve.
SAN palsy is rarely the cause in patients that present with initial shoulder pain, and thus, is commonly misdi- agnosed and delayed management. However, iatropathic or traumatic injury to the spinal accessory nerve was var- ious diagnostic periods. In the report by Camp et al, the
Table 2. Needle Electromyographic FindingsMuscle IA Spontaneous activity MUAPs Recruitment pattern
Lt trapezius (upper) increased Fibs & PSWs (+) Polyphasic Discrete
Lt levator scapuli Normal - Normal Full
Lt SCM increased Fibs & PSWs (+) Polyphasic Discrete
Lt rhomboid major Normal - Normal Full
Lt supraspinatus Normal - Normal Full
Lt infraspinatus Normal - Normal Full
Lt deltoid Normal - Normal Full
Lt biceps Normal - Normal Full
Lt triceps Normal - Normal Full
SCM: Sternocleidomastoid muscle, IA: Insertional activity, Fibs: Fibrillation potentials, PSWs: Positive sharp waves, MUAPs:
Motor unit action potentials, Full: full recruitment pattern, Discrete: Reduced recruitment pattern
Fig. 3. Sonographic findings suggestive of adhesive capsulitis showing a thickened coracohumeral ligament (arrow) (A) with sagittal view and fluid collection of biceps long head tendon sheath (arrowhead) (B).
A B
mean delay was 12.6 months and pain was severe in 63% patients in the study.
7Adhesive capsulitis is a common, painful condition of the shoulder, and is associated with loss of range of motion of the glenohumeral joint. Furthermore, it can occur in isolation (idiopathic) or concomitantly with another pathologic condition (secondary).
8Although two thirds of patients with SAN palsy are referred to a shoul- der surgeon for neurolysis and nerve reconstruction, they only experience partial improvements in pain relief and motor weakness after surgery.
9We considered his pathologic condition resulted from contracture of the glenohumeral joint capsule caused by shoulder conditions associated with muscle paralysis and subsequent adherence to the humeral head.
8As a result, we concluded his shoulder pain resulted from muscle paralysis and subsequent drooping of the left shoulder followed by pain and range of motion limitation. So we diagnosed the shoulder pain in our patient to be adhesive capsulitis, and thus, we administered a sonoguided steroid injection into the intra-articular space. He was treated with medication and physiotherapy, such as, hyperthermia treatment. Furthermore, we believe that the physical activity and strengthening exercises may have reduced the muscle contracture and prevented weakness progression.
In conclusion, many reports on cases of SAN palsy have focused on posterior neck and scapula movement.
Here, we describe a case of isolated SAN palsy with delayed shoulder pathology following whiplash injury.
Our experience of this case suggests that early diagnosis
and treatment of SAN palsy with shoulder pain leads to more effective pain relief and better functional out- comes.
3REFERENCES
1. 1. Chan PK, Hems TE. Clinical signs of accessory nerve palsy. J Trauma. 2006:60:1142-4.
2. Kelley MJ, Kane TE, Leggin BG. Spinal accessory nerve palsy: associated signs and symptoms. J Orthop Sports Phys Ther. 2008:38:78-86.
3. Omar N, Alvi F, Srinivasan MS. An unusual presentation of whiplash injury: long thoracic and spinal accessory nerve injury. Eur Spine J. 2007:16:275-7.
4. Ide M, Ide J, Yamaga M, Takagi K. Symptoms and signs of irritation of the brachial plexus in whiplash injuries. J Bone Joint Surg Br. 2001 Mar:83(2):226-9.
5. Mengiardi B, Pfirrmann CW, Gerber C, Hodler J, Zanetti M Frozen. shoulder: MR arthrographic findings. Radiolo- gy, 2004:233:486-492
6. Grossman JA, Ruchelsman DE, Schwarzkopf R. Iatro- genic spinal accessory nerve injury in children. J Pediatr Surg. 2008 Sep:43(9):1732-5.
7. Camp SJ, Birch R. Injuries to the spinal accessory nerve. J Bone Joint Surg Br. 2011 Jan:93(1):62-7
8. Anthony E. Adhesive capsulitis: A Review. Am Fam Physician. 2011:83(4):417-422.
9. Porter P, Fernandez GN. Stretch-induced spinal accessory nerve palsy: a case report. J Shoulder Elbow Surg. 2001 Jan-Feb:10(1):92-4.