REVIEW ARTICLE
진정내시경 시술 전후 환자 준비, 평가 및 회복
박홍준, 손병관
1, 구훈섭
2, 김병욱
3연세대학교 원주의과대학 내과학교실, 을지대학교 의과대학 내과학교실1, 건양대학교 의과대학 내과학교실2, 가톨릭대학교 인천성모병원 내과학교실3
Preparation, Evaluation, and Recovery before and after Conscious Sedative Endoscopy
Hong Jun Park, Byoung Kwan Son1, Hoon Sup Koo2, and Byung-Wook Kim3
Department of Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Department of Internal Medicine, Eulji General Hospital, Eulji University School of Medicine1, Seoul, Department of Internal Medicine, Konyang University College of Medicine2, Daejeon, Department of Internal Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea3, Incheon, Korea
(Korean J Gastroenterol 2017;69:59-63) Key Words: Endoscopy; Conscious sedation
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2017. Korean Society of Gastroenterology.
교신저자: 김병욱, 21431, 인천시 부평구 동수로 56, 가톨릭대학교 인천성모병원 내과학교실
Correspondence to: Byung-Wook Kim, Department of Internal Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 56 Dongsu-ro, Buyeong-gu, Incheon 21431, Korea. Tel: +82-32-280-5052, Fax: +82-32-289-5987, E-mail: [email protected]
Financial support: None. Conflict of interest: None.
서 론
진정은 진정약물을 이용하여 의식수준을 억제하는 것이다.
내시경에 있어서 진정은 검사 또는 시술에 대한 환자가 느끼 는 불안감을 최소화하여 최선의 내시경이 진행되도록 도와주 며, 일정기간 힘들었던 기억을 소실하게 하여 반복되는 추적 검사에 대한 순응도를 높일 수 있는 장점을 가지고 있다.1또 한, 내시경과 관련된 통증을 줄여줘서 시술을 용이하게 함으 로써 환자의 만족도를 높일 뿐만 아니라 내시경의사의 만족도 도 높일 수 있다.2,3 진정내시경은 이러한 장점으로 최근 널리 시행되고 있지만, 진정관련 합병증이라는 잠재적인 위험도 가 지고 있어서 이를 줄이기 위한 예방과 준비가 필수적이다. 특 히, 진정 전 환자에 대한 평가는 합병증 발생을 예측하고 대비 하는데 필수적인 절차이며, 진정 후 환자의 평가는 진정으로 부터 충분히 회복이 되어 퇴원이 가능한지 판단할 수 있는 근거가 된다. 본고에서는 진정내시경 전후 필요한 환자의 준 비와 평가 및 회복에 대하여 알아보고자 한다.
본 론
1. 국내 진정내시경
진정은 주로 사용되는 진정약물의 종류에 따라 미다졸람 기 본의 표준진정, 프로포폴 기본의 프로포폴 진정으로 나뉜다.
미다졸람과 비교하여 프로포폴의 특징은 길항제가 없고, 안전 역(margin of safety)이 좁아서 단독으로 사용할 때에 쉽게 깊 은 진정이 유도될 수 있어서 이와 관련된 책임인력이 각 국가 별 이슈가 되고 있다. 프로포폴 진정은 주체에 따라서 마취과 의사주도 프로포폴 진정(anesthesiologist administration of propofol, AAP)과 비마취과의사주도 프로포폴 진정(non-anes- thesiologist administration of propofol, NAAP)으로 분류된다.
보고에 따르면 국내 진정내시경의 행태는 프로포폴 사용의 98.6%가 내시경의사에 의해서 이뤄지고 88.5%를 내시경보조 자가 투여하는 비마취과의사주도(내시경의사 주도) 내시경보 조자 투여의 방법으로 시행되고 있다.4 최근 연구들에서 NAAP는 AAP보다 진정과 관련된 합병증을 더 높이지 않는 안전한 방법임을 보고하였고, 이는 적절하게 수련 받은 내시
Table 1. American Society of Anesthesiologists (ASA) physical status classification18 Class I A normal healthy patient
Class II A patient with mild systemic disease
Class III A patient with severe systemic disease that limits activity but is not incapacitating Class IV A patient with an incapacitating systemic disease that is a constant threat to life Class V A moribund patient who is not expected to survive for 24 h with or without an operation
경의사 또는 간호사에 의해서 적절하게 환자를 선택하여 충분한 감시하에 이뤄진다는 전제가 선행되어야 한다.5-7 NAAP에 대한 가이드라인은 2010년 제정되고 2015년 개정된 유럽위장관내시 경학회(European Society of Gastrointestinal Endoscopy, ESGE)가 유일하다.8
국내 진정교육은 주로 관련된 학회차원으로 이루어져 왔지 만, 아직까지 체계적인 교육시스템이나 국내 가이드라인은 없 는 상태이다. 이에, 대한의사협회를 중심으로 2016년 5월에
‘의원 및 병원급 의료기관 의사를 위한 프로포폴 진정 임상권 고안’이 만들어졌으며, 이를 기반으로 한 체계적 교육 프로그 램이 개발되어 시행 중에 있다.
2. 진정내시경 관련 합병증과 위험인자
진정관련 합병증은 대표적으로 저산소증, 저혈압, 고혈압, 부정맥, 약제과민성 등이 있다. 이 중 임상적으로 특히 문제가 되는 합병증이 저산소증이며, 중추신경억제에 따른 저환기증 과 수면무호흡증에 동반된 기도폐쇄가 원인이 된다. 저산소증 의 빈도는 사용되는 약제와 용량에 따라서 약 6-18%로 보고 되며, 이 중 심각한 심폐합병증은 1,000명 당 1명 정도로 알려 져 있다.2,9,10 실제로 국내에서 2009년부터 2014년까지 진정 관련 법적인 분쟁에 대한 분석에서 진정과 관련된 구체적 사 망원인으로 기도폐쇄나 저환기증에 따른 저산소증이 66%로 가장 많다고 보고를 하고 있다.11
진정관련 저산소증과 이와 관련된 위험인자는 고령, 3등급 이 상의 미국마취과학회 신체상태 분류(American Society of Anesthesiologists [ASA] physical status), 비만 등의 환자관련 인자와 장시간 진정을 요하는 고난도 내시경 시술 등이 있다.8
고령환자에서는 만성적인 환기-관류장애에 따른 만성적인 저 산소혈증 및 고탄산혈증이 동반되어 있는 경우가 흔하여 진정내 시경 시 발생한 저산소증의 자극에 대처하는 능력이 떨어질 수 있다고 알려져 있다.12 2000년부터 2008년까지 미국에서 시행된 내시경의 clinical outcomes research initiative database 1,300만 건을 분석하였을 때, 모든 내시경시술에 대하여 나이 가 들어감에 따라서 합병증의 발생빈도가 높아지는 경향을 보 였다.13 또한, 약 1만 명의 진정내시경에 대한 분석에서도 위, 대장내시경의 합병증이 발생한 평균연령은 60세 이상, 그중 에서 저산소증이 발생한 나이는 평균 65세로 보고되어 유럽 가이드라인에서도 고령은 진정관련 합병증의 위험인자로 제
시하고 있다.8,14
미국마취과학회 신체상태 분류는 환자의 전반적인 상태 및 동반 질환의 위험도를 분류하는 기준으로 3등급 이상의 높은 ASA는 독립적인 위험인자이다.15 각 등급의 추가적인 정보나 구체적인 예가 조금씩 달라서 같은 환자에 대한 일치도가 다 를 수 있지만, 임상에서 비교적 쉽게 환자의 전반적인 상태에 대한 평가를 할 수 있는 장점이 있다.16,17 대한의사협회 임상 권고안에서 제시하는 ASA등급표는 Table 118과 같다.
한국에서 체질량지수(body mass index, BMI)가 25 kg/m2 를 넘는 비만은 약 25%, BMI가 30 kg/m2을 넘는 고도비만은 약 5% 정도로 증가추세에 있다. 비만은 연령, 미국마취과학회 신체상태 분류와 더불어 진정내시경 시 발생할 수 있는 합병 증의 독립적인 위험인자로 알려져 있다.19,20
비만환자에서는 체지방의 비율이 증가하여 프로포폴이나 펜타닐과 같은 지용성 약제의 분포면적이 늘어나게 됨에 따라 중등도 진정에 필요한 약물 요구량이 증가하고, 효과가 오랫 동안 지속되어 진정에서 잘 깨어나지 못하는 경우도 있다.21 특히, BMI 30 이상의 고도 비만환자에서는 진정관련 저산소 증의 발생이 2배 정도 더 흔하게 발생할 수 있다고 알려져 있으며, 이는 비만환자에서 상부호흡계의 구조적인 변형으로 높은 Mallampati점수를 보이고, 수면무호흡증이 흔하게 발생 하기 때문이다.22수면무호흡증이 있는 경우 진정 시 발생하는 저산소증의 빈도가 15%로 수면무호흡증이 없는 경우 4%보 다 매우 높다.8 또한, Mallampati점수는 수면 중 발생할 수 있는 희발호흡 또는 저호흡(hypopnea or apnea)점수와 높은 연관성이 있다고 보고되고 있어서, 비만-높은 Mallampati점 수-수면무호흡증은 서로 맞물려서 진정 시 기도폐색에 의한 저산소증을 유발시킬 수 있는 위험인자로 작용할 수 있다.23
3. 진정 전 환자의 평가와 준비
진정내시경 관련 합병증의 위험인자를 가지고 있는 고위험 환자는 진정 전 환자의 평가를 통하여 선별이 필요하다. 고위 험도 환자에 대한 선별을 통하여 진정 시 산소투여나 진정약 물을 조정하는 등 추가적인 합병증을 줄이기 위한 노력이 필 요한지의 여부를 결정하고, 위험도가 큰 경우 마취과의사에 의한 진정이 필요할 수도 있기 때문이다.
국내 대한의사협회 프로포폴 진정 임상권고안에서는 시술/
수술의 침습도, 환자의 진정 관련 위험인자, 및 시술자의 임상
Table 2. STOP-BANG Questionnaire24,25
S Snoring: Do you snore loudly (louder than talking or loud enough to be heard through closed door?) Yes/No
T Tired: Do you often feel tired, fatigued, or sleepy during the daytime? Yes/No
O Observed: Has anyone observed you stop breathing during your sleep? Yes/No
P Blood pressure: Have you or are you being treated for high blood pressure? Yes/No
B BMI: >35 kg/m2 Yes/No
A Age: Age older than 50 y Yes/No
N Neck circumference: >40 cm Yes/No
G Gender: Male Yes/No
High risk of obstructive sleep apnea (OSA): yes to 3 or more question; low risk of OSA: yes less than 3 questions. BMI, body mass index.
능력과 경험에 따라 종합적으로 판단하여, 아래의 경우에는
‘마취통증의학과 전문의에 의한 프로포폴 진정(감시하 전신마 취; monitored anesthesia care)’을 고려할 것으로 제시하고 있다.
① 미국마취과학회 신체상태 분류법에서 3등급, 4등급, 5등급
② 장시간 또는 침습도가 높은 시술/수술 시의 깊은 진정
③ 기도폐쇄 또는 기관내 삽관이 어려울 것으로 예측되는 위험인자를 가진 환자
④ 과거 진정 또는 마취 시 부작용 경험 환자
이를 위해서 진정 전 확인사항으로 유럽 NAAP 가이드라 인에서 다음과 같이 제시하였다.8
① Age
② ASA physical status
③ Body mass index
④ Mallampati’s classification
⑤ Risk factors for obstructive sleep apnea (OSA)
⑥ Risk of airway obstruction (e.g. pharyngolaryngeal tumors)
⑦ Type of endoscopic procedure
특히, 수면무호흡증에 대한 위험도에 대한 평가로 STOP- BAND questionnaire를 권고하는데 이는 몇 가지 문진과 신 체검사 등으로 다음과 같이 확인할 수 있다(Table 2).24,25
국내 대한의사협회 프로포폴 진정 임상권고안에서는 이와 같은 사항을 포함하여 조금 더 포괄적으로 제시하고 있으며, 이는 진정내시경 전에 꼭 확인해야 할 사항들이다.
진정 전 적절한 환자 평가
1) 진정 전 활력징후(baseline vital sign)
2) 미국마취과학회 신체상태 분류(American Society of Anesthesiologists [ASA] physical status)
3) 기도의 이학적 검사(기능적 및 해부학적 요인으로 마스크 환기나 기 관 내 삽관에 어려움을 제공할 수 있는 위험인자 파악)
4) 과거 진정 및 마취 시 특이사항 5) 현재 약물 복용 상태 및 약제 알레르기 6) 동반 심혈관계 및 호흡기 질환 7) 가임기 여성의 경우 현재 임신 여부
8) 진정 처치 후 귀가 시 안전 문제 고려(처치 후 귀가 시 보호자 동행을 권장하나, 개별 환자 별로 진료의사가 선택적 적용 가능)
응급처치가 아닌 경우 전신 마취와 동일한 수준의 금식 시 간이 필요하며 깨끗한 소량의 물은 최소 2시간, 고형식, 우유 의 경우 최소 6-8시간 이상의 금식 시간이 지켜져야 한다.
4. 진정 후 회복에 대한 평가
내시경검사가 종료된 후에도 진정약물에 의한 합병증 발생 의 위험은 남아있는 상태이다. 환자에 대한 자극이 줄어들고 진정약물의 대사지연에 따른 약 효과가 지속되는 경우도 있으 므로 회복 시에도 의식수준, 혈압과 맥박, 산소 포화도를 모니 터링해야 한다. 회복관찰 시간이나 효용성에 대한 문헌 보고 된 연구는 드물지만 회복실에서의 환자 관리 및 퇴실에 대한 정해진 기준과 매뉴얼은 반드시 필요하다.13
진정에서 회복되어 퇴실이 가능한 상태라 하면, 의식이 명 료하고 지남력이 적절하여야 하고, 생체징후가 안정적으로 유 지가 되어야 하며, 회복 평가 점수가 적절해야 한다. 퇴실 후 에 발생할지도 모르는 사고에 대비하여 보호자와 동반하여 안 전하게 귀가하도록 하며, 퇴원 후 식사, 투약 및 활동 제약에 대한 정보 및 응급 연락번호를 제공하는 것도 좋은 방법이다.
진정 시술 당일에는 자동차 운전이나 고도의 집중력이 필 요한 활동과 알코올이나 흥분 각성제 및 수면제의 섭취는 피 하도록 교육해야 한다.
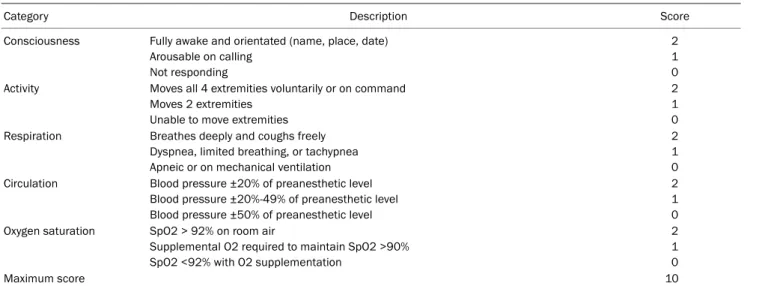
회복 평가 점수로는 Modified Aldrete score (Table 3)26 또는 마취 후 퇴원점수체계(postanesthetic discharge scor- ing system, PADSS) (Table 4)27를 퇴실 기준으로 많이 사용 하고 있다. Modified Aldrete score 기준으로 8점 이상, PADSS 기준으로 9점 이상이면 퇴실이 가능한 상태이다.
결 론
최근 건강에 대한 관심이 높아지고 있으며, 국내의 위암 발 생이 매우 높고, 대장암의 발생이 꾸준히 증가하고 있는 인구 학적 특성과 더불어 내시경의 접근성이 좋고, 비용이 저렴하 다는 의료환경적인 상황으로 인해 내시경 시행은 꾸준히 증가 하고 있으며, 이와 더불어 진정의 비율도 높아지고 있다. 또 한, 향후 진정에 대한 보험급여가 예정되어 있어서 진정내시
Table 3. Modified Aldrete Score26
Category Description Score
Consciousness Fully awake and orientated (name, place, date) Arousable on calling
Not responding
2 1 0 Activity Moves all 4 extremities voluntarily or on command
Moves 2 extremities Unable to move extremities
2 1 0 Respiration Breathes deeply and coughs freely
Dyspnea, limited breathing, or tachypnea Apneic or on mechanical ventilation
2 1 0 Circulation Blood pressure ±20% of preanesthetic level
Blood pressure ±20%-49% of preanesthetic level Blood pressure ±50% of preanesthetic level
2 1 0 Oxygen saturation SpO2 > 92% on room air
Supplemental O2 required to maintain SpO2 >90%
SpO2 <92% with O2 supplementation
2 1 0
Maximum score 10
Adequate to discharge when the total score is 8 or over, or when the score is same before and after surgery.
Table 4. Post Anaesthetic Discharge Scoring System27 1. Vital Signs
2 = Within 20% of preoperative value 1 = 2040% of preoperative value 0 = > 40% preoperative value 2. Activity and mental status
2 = Oriented x3 AND has a steady gait 1 = Oriented x3 OR has a steady gait 0 = Neither
3. Pain, nausea and/or vomiting 2 = Minimal
1 = Moderate, having required treatment 0 = Severe, requiring trealtment 4. Bleeding
2 = Minimal 1 = Moderate 0 = Severe 5. Intake and output
2 = Has had PO fluids AND voided 1 = Has had PO fluids OR voided 0 = Neither
Total pads score is 10; Score ≥ 9 considered it for discharge.
경은 지금보다 더 증가할 것으로 예상된다.
이러한 의료환경의 변화에 발맞추어 대한의사협회에서 최 근 제시된 ‘의원 및 병원급 의료기관 의사를 위한 프로포폴 진정 임상권고안’은 현재로서 국내 진정의 현실을 감안한 최 선의 진정방법을 제시하고 있다. 이를 바탕으로 진정내시경 전후 환자에 대한 적절한 평가와 위험도 관리를 통해 보다 더 안전하고 질 높은 진정내시경을 제공할 수 있으리라 생각 된다.
REFERENCES
1. Cohen LB, Delegge MH, Aisenberg J, et al. AGA Institute review of endoscopic sedation. Gastroenterology 2007;133:675-701.
2. McQuaid KR, Laine L. A systematic review and meta-analysis of randomized, controlled trials of moderate sedation for routine endoscopic procedures. Gastrointest Endosc 2008;67:910-923.
3. Schroeder C, Kaoutzanis C, Tocco-Bradley R, et al. Patients prefer propofol to midazolam plus fentanyl for sedation for colono- scopy: results of a single-center randomized equivalence trial.
Dis Colon Rectum 2016;59:62-69.
4. Lee CK, Dong SH, Kim ES, et al. Room for quality improvement in endoscopist-directed sedation: results from the first nation- wide survey in Korea. Gut Liver 2016;10:83-94.
5. Ferreira AO, Torres J, Barjas E, et al. Non-anesthesiologist admin- istration of propofol sedation for colonoscopy is safe in low risk patients: results of a noninferiority randomized controlled trial.
Endoscopy 2016;48:747-753.
6. American Association for Study of Liver Diseases; American College of Gastroenterology; American Gastroenterological Association Institute, et al. Multisociety sedation curriculum for gastrointestinal endoscopy. Gastrointest Endosc 2012;76:e1-e25.
7. Dumonceau JM, Riphaus A, Beilenhoff U, et al. European curricu- lum for sedation training in gastrointestinal endoscopy: position statement of the European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Gastroenterology and Endoscopy Nurses and Associates (ESGENA). Endoscopy 2013;45:496-504.
8. Dumonceau JM, Riphaus A, Schreiber F, et al. Non-anesthesiolo- gist administration of propofol for gastrointestinal endoscopy:
European Society of Gastrointestinal Endoscopy, European Society of Gastroenterology and Endoscopy Nurses and Associates Guideline--Updated June 2015. Endoscopy 2015;47:1175-1189.
9. Triantafillidis JK, Merikas E, Nikolakis D, Papalois AE. Sedation
in gastrointestinal endoscopy: current issues. World J Gastroenterol 2013;19:463-481.
10. Agostoni M, Fanti L, Gemma M, Pasculli N, Beretta L, Testoni PA.
Adverse events during monitored anesthesia care for GI endos- copy: an 8-year experience. Gastrointest Endosc 2011;74:266-275.
11. Roh WS, Kim DK, Jeon YH, et, al. Analysis of anesthesia-related medical disputes in the 2009-2014 period using the Korean Society of Anesthesiologists database. J Korean Med Sci 2015;
30:207-213.
12. ASGE Standards of Practice Committee, Chandrasekhara V, Early DS, et al. Modifications in endoscopic practice for the elderly. Gastrointest Endosc 2013;78:1-7.
13. Enestvedt BK, Eisen GM, Holub J, Lieberman DA. Is the American Society of Anesthesiologists classification useful in risk strat- ification for endoscopic procedures? Gastrointest Endosc 2013;
77:464-471.
14. Friedrich K, Stremmel W, Sieg A. Endoscopist-administered pro- pofol sedation is safe - a prospective evaluation of 10,000 pa- tients in an outpatient practice. J Gastrointestin Liver Dis 2012;21:259-263.
15. Cohen LB, Delegge MH, Aisenberg J, et al. AGA Institute review of endoscopic sedation. Gastroenterology 2007;133:675-701.
16. Dripps RD, Lamont A, Eckenhoff JE. The role of anesthesia in sur- gical mortality. JAMA 1961;178:261-266.
17. Fitz-Henry J. The ASA classification and peri-operative risk. Ann R Coll Surg Engl 2011;93:185-187.
18. Haynes SR, Lawler PG. An assessment of the consistency of ASA physical status classification allocation. Anaesthesia 1995;50:
195-199.
19. Wani S, Azar R, Hovis CE, et al. Obesity as a risk factor for seda- tion-related complications during propofol-mediated sedation for advanced endoscopic procedures. Gastrointest Endosc 2011;74:1238-1247.
20. Berzin TM, Sanaka S, Barnett SR, et al. A prospective assessment of sedation-related adverse events and patient and endoscopist satisfaction in ERCP with anesthesiologist-administered sedation.
Gastrointest Endosc 2011;73:710-717.
21. Vargo JJ. Procedural sedation and obesity: waters left uncharted.
Gastrointest Endosc 2009;70:980-984.
22. Wani S, Azar R, Hovis CE, et al. Obesity as a risk factor for seda- tion-related complications during propofol-mediated sedation for advanced endoscopic procedures. Gastrointest Endosc 2011;74:1238-1247.
23. Friedman M, Tanyeri H, La Rosa M, et al. Clinical predictors of ob- structive sleep apnea. Laryngoscope 1999;109:1901-1907.
24. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008;108:812-821.
25. Jirapinyo P, Thompson CC. Sedation challenges: obesity and sleep apnea. Gastrointest Endosc Clin N Am 2016;26:527-537.
26. Rudner R, Jalowiecki P, Kawecki P, Gonciarz M, Mularczyk A, Petelenz M. Conscious analgesia/sedation with remifentanil and propofol versus total intravenous anesthesia with fentanyl, midazolam, and propofol for outpatient colonoscopy. Gastrointest Endosc 2003;57:657-663.
27. Chung F, Chan VW, Ong D. A post-anesthetic discharge scoring system for home readiness after ambulatory surgery. J Clin Anesth 1995;7:500-506.