https://doi.org/10.14734/PN.2021.32.2.80 pISSN 2508-4887•eISSN 2508-4895
Eun Hye Jeon, MD, Sul Lee, MD, So Hee Kim, MD, Hyung Joon Yoon, MD, Jong Kil Joo, MD, PhD, Seung Chul Kim, MD, PhD Department of Obstetrics and Gynecology, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea
Pregnancy-associated atypical hemolytic-uremic syndrome (p-aHUS) is a rare and fatal thrombotic microangiopathy characterized by hemolytic anemia, thrombocytopenia and acute renal injury during pregnancy. A pregnant woman with atypical symptoms of hemolytic-uremic syndrome (HUS) delivered a baby by cesarean delivery under suspicion of atypical hemolysis, elevated liver enzymes, low platelets (HELLP) syndrome at 35 weeks of gestation. However, even after delivery, the patient’s condition worsened. Following this, p-aHUS was diagnosed through as a result of ADAMTS13 activity.
After several plasma exchanges (PEs) based on diagnosis, vital signs were stabilized and laboratory results were normalized. Herein, we report and review an unusual case of woman with complicated p-aHUS who recovered after PE.
Key Words: Atypical hemolytic-uremic syndrome, Plasma exchange, Thrombotic microangiopathy
Introduction
Hemolytic-uremic syndrome (HUS) is a rare thrombotic angiopathy characterized by hemolytic anemia, thrombocytopenia, and acute renal injury. In most cases, HUS is caused by infection with certain strains of Escherichia coli. Atypical HUS (aHUS), not caused by Shiga-like toxin producing bacteria, is a complement-mediated disorder. A mortality rate of up to 25% and progression to end-stage renal disease in half of the patients has been previously reported.1,2 In p-aHUS, pregnancy may act as a trigger for complement activation in genetically susceptible individual. Diagnosis of p-aHUS is often delayed due to its rare incidence and difficulty in distinguishing it from other thrombotic microangiopathy disorders.
Therefore, understanding the characteristics of these diseases can help in the diagnosis.
Early diagnosis and immediate management have a profound effect on prognosis. Therapeutic options for aHUS are plasma exchange (PE) and eculizumab, a monoclonal antibody against complement protein C5.3 Here we report a case of p-aHUS diagnosed during postpartum period that, owing to rapid diagnosis and timely treatment, resulted in favorable outcomes and successful renal recovery.
Case
A 36-year-old pregnant woman with gravida 2 para 1 was referred to the hospital from a local clinic at 34 weeks and 4 days of gestation due to diarrhea and vomiting for 1 day.
The patient had no significant medical or family history, other than the history of cesarean delivery for her first child with cephalopelvic disproportion in the previous year. During antenatal screening at the local clinic, there were no abnormal findings.
Received: 13 September 2020 Revised: 13 November 2020 Accepted: 14 December 2020 Correspondence to Seung Chul Kim, MD, PhD Department of Obstetrics and Gynecology, Pusan National University Hospital, Pusan National University School of Medicine, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea
Tel: +82-51-240-7282 Fax: +82-51-248-2384 E-mail: [email protected] Copyright© 2021 by The Korean Society of Perinatology
This is an Open Access article distributed under the terms of the Creative Com- mons Attribution Non-Commercial License (http://creativecommons.org/
license/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any
Case Report of Pregnancy Induced Atypical
Hemolytic-uremic Syndrome
examinations revealed elevated levels of hemoglobin (Hb) 19.2 g/dL, white blood cell 8.94×103/uL, platelet 167×103/uL, lactate dehydrogenase (LDH) 386 IU/L, aspartate transaminase (AST) 152 IU/L, alanine aminotransperase (ALT) 180 IU/L, blood urea nitrogen (BUN) 23.2 mg/dL and creatinine (Cr) 1.58 mg/dL. Although proteinuria (1+ dipstick) was present, her blood pressure values were within normal limits. Therefore, preeclampsia could be excluded. Chest radiography and electo- cardiography were also nonspecific. The antibody tests (C3, Immunoglobulin A, fluorescent antinuclear antibody, anti-ds DNA, IgG, antineutrophil cytoplasmic antibodies) performed for excluding autoimmune diseases that could cause kidney damage, showed normal results. Liver, kidney ultrasound and echocardiography also revealed no abnormal findings.
Laboratory findings deteriorated over time despite the steady normal blood pressure values. On the fourth day of hospitali- zation, thrombocytopenia (65,000/IU) began to appear and Cr (2.12 mg/dL) and AST (611 IU/L) levels were elevated.
Despite the worsening of the laboratory findings, the patient did not complain of any symptoms. At 35 weeks of gestation, emergency cesarean delivery was performed under suspicion of atypical hemolysis, elevated liver enzymes, low platelets (HELLP) syndrome. The operation was completed uneventfully, and the newborn was in good condition with a weight of 2,720 g and Apgar score of 7/9. There was no abnormality in the breath- ing or laboratory examination of the newborn after delivery.
After surgery, the patient entered the intensive care unit for close monitoring. The day after cesarean delivery, the value of
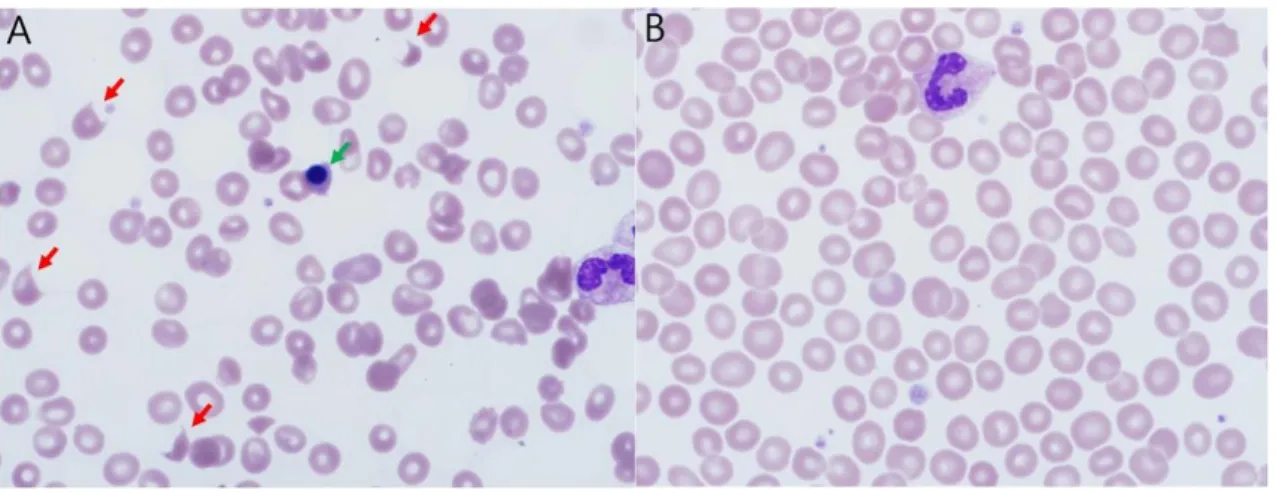
LDH peaked at 1,800 IU/L or more, and peripheral blood smear (PBS) revealed micro-angiopathic hemolytic anemia (MAHA) with schistocytes (Fig. 1A). Her AST and Cr levels were also elevated and thrombocytopenia worsened. The hematologist was consulted ADAMTS13 levels were checked and daily PE with transfusion of packed RBCs and platelets was initiated. The laboratory values improved with each PE. After four cycles of daily PE, the values of LDH, Hb, and platelet were normalized (Fig. 2). PBS was also normalized without any further schistocyte findings (Fig. 1B). The patient underwent a total of five cycles of PE. On postoperative day 4, prednisolone was initiated at a dose of 30 mg/day. On postoperative day 6, ADAMTS13 activity was reported to be normal at 69.5% and then diagnosis of p-aHUS was confirmed. On postoperative day 11, she was discharged without further complications. At present, the patient is doing well in clinical remission without further treatment.
Discussion
P-aHUS occurs in approximately 10-15% of female pa- tients with aHUS. It has been reported in 0.004% of all pregnancies, mostly in the postpartum period.4 P-aHUS is associated with high maternal and fetal morbidity and mortality. Preterm delivery and intrauterine fetal death are common and often progress to end-stage renal disease that require dialysis or kidney transplant.
The associated pathogenesis is uncontrolled complement
Fig. 1. Peripheral blood smears (A: before, B: after) showing many schistocytes (red arrows) and a nucleated red blood cell (green arrow) (×1,000, Wright stain).
plement activation. Pregnant women with such mutations are more likely to develop p-aHUS.7,8 Therefore, it leads to unrestrained complement activation and generation of the membrane attack complex (MAC). MAC deposition incites an inflammatory response that results in diffuse endothelial damage, platelet activation, and thrombotic microangiopathy with multi-organ dysfunction.2
Diagnosing p-aHUS is challenging. The first reason is the activation that contributes to aHUS. In particular, pregnancy
could be a complement amplifying condition, and maternal exposure to semi-allogenic feto-placental tissue increases over gestation, with peak exposure at delivery.5,6 The patient in this case also worsened immediately after delivery. Excess complement activation is often mitigated by the alternative complement pathway. However, inherited mutations in re- gulators are the predisposing factors which increase com-
A B
C D
E F
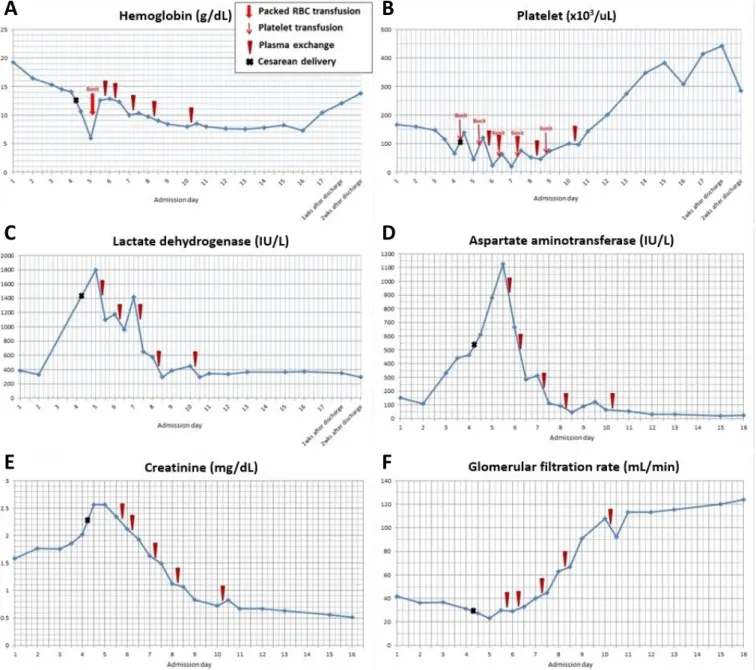
Fig. 2. The figure outlines the response to plasma exchange. (A) Hemoglobin, (B) platelet and (C) lactate dehydrogenase obtained through hemolysis rapidly recover after each plasma exchange (PE). (D) Aspartate aminotransferase, indicator of the liver function, falls dramatically after each PE. (E) Creatinine and (F) glomerular filtration rate, indicators of renal function, improve after each PE.
has been empirically considered to be plasma infusion and exchange. This procedure not only provides a functional complement regulatory factor but also removes abnormal complement-related factors such as mutant proteins. PE can increase survival rates by 80% to 90%. PE as first-line treatment during pregnancy has a response rate of 64%.10 It should be promptly performed daily. Serial assessment of hematologic, renal, and hepatic function is also essential.
Currently, a multidisciplinary approach is needed. The treat- ment using a complement-inhibiting drug, eculizumab, is now replacing plasma therapy as the gold standard in the management of aHUS. Eculizumab, a monoclonal humanized antibody against C5, prevents MAC formation. Gupta et al.3 in their systematic review summarized that more females achieved disease remission when treated with eculizumab compared to those not treated with eculizumab (88% vs.
57%, P=0.02). In addition, corticosteroids were sometimes effective in aHUS.
During the assessment of our case, aHUS was not dia- gnosed at the first instance. The patient was suspected to have a relatively common HELLP syndrome. However, as the patient’s condition did not improve after delivery, aHUS or TTP were considered. As ADAMTS13 activity appears after a long duration, considering the patient’s condition, first PE was performed under consultation with a hematologist.
The patient responded favorably to PE and steroid therapy.
Therefore, eculizumab was not required. We assume that our report is significant since the patient remained in complete remission after PE without anti-complement therapy.
The strength of this case report is that, like other cases reported in Korea and abroad, we could estimate the pro- gress pattern of the disease because the patient was tested during the early stages of the HUS outbreak. In the regard, our case report is very meaningful.
In conclusion, early diagnosis of aHUS followed by imme- diate PE may be beneficial in preventing long-term sequelae such as chronic renal failure. Further assessment of the patients with p-aHUS could help facilitating its diagnosis and management.
presence of features similar to many other diseases such as thrombotic thrombocytopenic purpura (TTP), HELLP syndrome, and acute fatty liver syndrome of pregnancy (AFLP). They all often show thrombocytopenia, MAHA, and renal dysfunction, which mostly co-exist.7 Secondly, there is no specific test available to confirm the diagnosis of aHUS, which is diagnosed through exclusion. The disease condi- tions such as anemia, thrombocytopenia, and acute kidney injury occurring during pregnancy or the postpartum period, should be quickly suspected. Knowing the features and etiologies of the above disorder may aid in distinguishing them.
Preeclampsia is a disorder caused during pregnancy and can further develop into HELLP syndrome. About 70% of the cases have been reported to develop before delivery.
However, it usually recovers within a week of delivery.
AFLP occurs in the third trimester or early postpartum period. Patients often present with nonspecific symptoms such as nausea, headache, and abdominal pain. AFLP often presents more acutely than preeclampsia, which can develop over several days or weeks. It recovers within 1-2 days of delivery. In this case, preeclampsia and AFLP were ruled out owing to the non-recovery of the patient after delivery. TTP, as with other MAHA, is caused by spontaneous aggregation of platelets and activation of coagulation in the small blood vessels. Onset of TTP occurs in the first trimester in 12%
patients, in the second in 56%, and in the third trimester or soon postpartum in 32% patients.9 In TTP, neurological symptoms are quite common, varying greatly in severity.
Frequently reported symptoms include fatigue, confusion, and headaches. In this case, there were no neurological symptoms even when the laboratory test was abnormal.
Unlike HELLP and AFLP, aHUS and TTP do not recover after delivery. Alternatively, in the case of patients with aHUS or TTP, delivery does not act as a definitive treatment.
TTP occurs due to autoimmunity and an inherited deficiency of ADAMTS13. Therefore, TTP can be easily ruled out with an ADAMTS13 activity level >10% and the absence of autoantibodies.
Until a diagnosis of p-aHUS can be made with reasonable certainty, the initial treatment should be approached on a case-by-case basis. The first-line management for aHUS
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Acknowledgemants
This study was supported by clinical grant in 2019 from Pusan National University Hospital.
References
1) Egerman RS, Witlin AG, Friedman SA, Sibai BM. Thrombotic thrombo
cytopenic purpura and hemolytic uremic syndrome in pregnancy:
review of 11 cases. Am J Obstet Gynecol 1996;175(4 Pt 1):9506.
2) Noris M, Remuzzi G. Atypical hemolyticuremic syndrome. N Engl J Med 2009;361:167687.
3) Gupta M, Govindappagari S, Burwick RM. Pregnancyassociated atypical
hemolytic uremic syndrome: a systemic review. Obstet Gynecol 2020;
135:4658.
4) Dashe JS, Ramin SM, Cunningham FG. The longterm consequences of thrombotic microangiopathy (thrombotic thrombocytopenic purpura and hemolytic uremic syndrome) in pregnancy. Obstet Gynecol 1998;
91(5 Pt 1):6628.
5) Richani K, Soto E, Romero R, Espinoza J, Chaiworapongsa T, Nien JK, et al. Normal pregnancy is characterized by systemic activation of the complement system. J Matern Fetal Neonatal Med 2005;17:23945.
6) Medearis AL, Hensleigh PA, Parks DR, Herzenberg LA. Detection of fetal erythrocytes in maternal blood post partum with the fluorescence
activated cell sorter. Am J Obstet Gynecol 1984;148:2905.
7) Fakhouri F, Roumenina L, Provot F, Sallée M, Caillard S, Couzi L, et al.
Pregnancyassociated hemolytic uremic syndrome revisited in the era of complement gene mutations. J Am Soc Nephrol 2010;21:85967.
8) Bruel A, Kavanagh D, Noris M, Delmas Y, Wong EKS, Bresin E, et al.
Hemolytic uremic syndrome in pregnancy and postpartum. Clin J Am Soc Nephrol 2017;12:123747.
9) Martin JN Jr, Bailey AP, Rehberg JF, Owens MT, Keiser SD, May WL.
Thrombotic thrombocytopenic purpura in 166 pregnancies: 1955
2006. Am J Obstet Gynecol 2008;199:98104.
10) Davies GE. Thrombotic thrombocytopenic purpura in pregnancy with maternal survival. Case report. Br J Obstet Gynaecol 1984;91:3968.