근신경계 질환에서의 안구운동장애
허영은
분당서울대학교병원 신경과
Eye Findings in Neuro-muscular Diseases
Young-Eun Huh, MD
Department of Neurology, Seoul National University Bundang Hospital, Seongnam, Korea
Ocular myasthenia is a subtype of myasthenia gravis causing diplopia, ptosis, and weakness of lid closure. Clinically, ocular myas- thenia can mimic any form of pupil-sparing ocular motility disorder. Dynamic abnormalities of myasthenic eye movements may reflect the primary hallmarks of the disease, which are fatigability and variability in strength, or secondary adaptive effects by the central nervous system. Ice, sleep, and rest tests are safe and inexpensive test for ocular myasthenia with high specificity and sensi- tivity. Abnormal eye movements are increasingly recognized in patients with amyotrophic lateral sclerosis (ALS) and, when they occur, may provide insights into the pattern and pathogenesis of the disease process. Disorders of saccade (slow saccade, delayed memory-guided saccade, inaccurate and delayed antisaccade), smooth pursuit (decreased gain), ocular fixation (increased sacca- dic intrusion amplitude), and ophthalmoplegia are reported in patients with ALS.
Keywords: Ocular myasthenia; Amyotrophic lateral sclerosis; Eye movement
근신경계 질환에서도 다양한 형태의 안증상을 보일 수 있다. 본문 에서는 안구형 중증근무력증(ocular myasthenia gravis)과 근위축성 측색 경화증(amyotrophic lateral sclerosis, ALS) 환자에서 보이는 안증 상에 대해 간략하게 기술하였다.
안구형 중증근무력증
안구형 중증근무력증(ocular myasthenia gravis)은 근위약이 외안 근 (extraocular muscle), 윗눈꺼풀올림근(levator palpabrae superioris muscle), 눈둘레근(orbicularis oculi muscle)을 포함한 안구 주변 근육 에 국한되어 나타나는 중증근무력증의 아형이다. 75%의 근무력증 환 자가 초기 증상으로 안증상을 호소하며 이 중 90% 이상은 전신형으 로 발전한다.
140-50%는 초기에 안증상만을 보이는 경우가 있는데, 이 중 30-40%만이 안구형으로 남아 결과적으로 안구형이 전체 근무력
증에서 차지하는 비율은 약 12-15% 정도이다.
2안구형 중증근무력증 은 침범하는 근육에 따라 다양한 형태의 안증상을 보이는데, 이는 안 근마비 및 피로(fatigue)에 의한 증상과 이를 보상하려는 이차적 중추 신경계 적응작용(secondary adaptive mechanism)이 복합된 형태를 띤 다 . 본문에서는 안구형 중증근무력증에서 나타나는 특징적 안증상을 침범하는 근육에 따라 기술하고 이를 진단하는 방법을 제시하였다.
1. 안구형 중증 근무력증의 안증상
1) 윗눈꺼풀올림근윗눈꺼풀올림근 (levator palpabrae superioris muscle) 위약으로 인한 안검하수 (ptosis)는 단독으로 발생할 수도 있고 다른 안구 주변 근마 비를 동반할 수도 있다. 안검하수가 있는 환자에서 피로현상 및 기복 (fluctuation) 을 호소하는 경우, 근무력증을 강력히 의심할 수 있다. 안 검하수는 일측성 또는 양측성으로 발생하고, 대개는 비대칭적이다.
Correspondence to: Young Eun Huh, MD
Department of Neurology, Seoul National University Bundang Hospital, 300 Gumi-dong, Bundang-gu, Seongnam 463-707, Korea Tel: +82-31-787-6551; Fax: +82-31-719-6818; E-mail: [email protected]
Received: Jun. 8, 2011 / Accepted: Jul. 11, 2011
REVIEW
병력청취상 아침에 일어날 때는 증상이 없다가 시간이 갈수록 안검하 수가 뚜렷해지는 증상을 호소하는 것이 특징적이다. 안검하수는 지 속적 상방주시 시에 악화(lid fatigue test)되므로, 환자에게 수분간 위 를 쳐다보게 하면 안검하수가 나타나거나 악화됨을 관찰할 수 있다.
일측성으로 안검하수를 보이는 경우, 눈꺼풀을 손가락으로 들어올리 면 정상처럼 보였던 눈에 안검하수가 뚜렷해지는 현상(enhanced pto- sis) 을 관찰할 수 있는데, 이는 실제로 양측 안검하수가 있으나 Hering 의 법칙(공액근에는 동일한 정도의 신경지배가 이루어짐)에 의해 안 검하수 정도가 심하지 않은 쪽이 정상처럼 보이기 때문이다.
3근무력증 환자는 안검 후퇴(lid retraction) 역시 보일 수 있다. 일측 성으로 안검하수가 있는 경우 반대편에 안검 후퇴를 보일 수 있는데 (Fig. 1), 이 역시 Hering 의 법칙에 의한 것으로 아래를 바라보게 하거 나 안검하수가 있는 눈꺼풀을 들어올리면 안검 후퇴는 호전된다. 또 한 , 근무력증 환자의 4-10%가 갑상선 질환을 동반하므로 갑상선안병 증의 일종으로 안검 후퇴를 보일 수 있다.
4마지막으로 지속적 상방주 시 후에 일시적으로 안검 후퇴가 발생할 수 있는데, 이는 강직후 촉진 (post-tetanic facilitation) 또는 근긴장(myotonia)에 의한 현상이므로,
5Lambert-Eaton 증후군의 가능성도 고려해야 한다.
6아래를 10-20초간 바라보게 한 뒤 빠르게 정면을 보게 하면 눈꺼풀 이 일시적으로 위로 올라갔다가 아래로 처지는 현상이 나타날 수 있 는데 이를 ‘Cogan’s lid twitch’ 징후라 한다.
7이는 아래를 바라보는 동 안 근무력이 빠르게 회복되었다가 눈꺼풀을 들어올리면서 쉽게 피로 현상이 생기기 때문이다.
2) 눈둘레근
눈둘레근 (orbicularis oculi muscle) 역시 근무력증에서 흔하게 침범 되며 눈을 힘껏 감으라고 한 뒤 검사자가 눈을 억지로 띄우면서 위약 여부를 판단한다. 눈을 힘껏 감을 때 속눈썹이 눈꺼풀 틈새에 묻혀야 정상이며 , 눈을 감을 때 눈꺼풀 틈새가 벌어져서는 안 된다. 눈을 감고 서 시간이 지나면 눈둘레근의 피로현상으로 눈꺼풀 틈새가 서서히 벌 어지는 ‘peek-a-boo’ 징후를 보일 수 있다.
83) 외안근
외안근 (extraocular muscle) 마비에 의한 복시는 근무력증의 두 번 째로 흔한 증상이며 근무력증 환자의 90%가 복시를 호소한다. 대체 로 외안근 마비는 안검하수를 동반한다. 다양한 형태의 사시를 보이 는데 , 내직근(medial rectus muscle), 하직근(inferior rectus muscle), 상 사근 (superior oblique muscle)이 흔히 침범된다.
9안구형 근무력증은 말초성 외안근 마비는 물론 중추성 주시 마비의 형태로도 나타날 수 있으므로 , 동공침범이 없는 안근마비에서는 항상 안구형 중증근무 력증의 가능성을 염두하여야 한다. 안구형 근무력증의 안구운동장 애는 Table 1로 요약하였다. 외안근이 광범위하고 심하게 침범된 경우 에는 만성 진행성 외안근마비(chronic progressive external ophthal- moplegia)와 구별이 어려울 수 있다.
10두 질환 모두 외안근 완전마비, 안검하수 , 눈둘레근 위약을 보일 수 있고, 단일근섬유 근전도(single fiber electromyography)에서 jitter 증가를 보일 수 있기 때문이다. 만성
Table 1. Patterns of ocular motility impairment observed in myasthenia gravis
Patterns of motility impairment Mimicked syndrome
Unilateral abduction deficit Abducens nerve palsy
Unilateral infraduction deficit Inferior divisional oculomotor nerve palsy
Adduction, infraduction, and supraduction deficit Pupil-sparing oculomotor nerve palsy
Ptosis and supraduction deficit Superior division oculomotor nerve palsy
Hypertropia on contralateral gaze Trochlear nerve palsy
Inferior oblique palsy Brown syndrome
Unilateral or bilateral adduction deficit with/without abducting nystagmus in opposite eye Unilateral or bilateral internuclear ophthalmoplegia
Bilateral upgaze palsy Supranuclear vertical gaze palsy (eg. progressive suparnuclear palsy)
Parinaud’s syndrome
Horizontal gaze palsy Nuclear or supranuclear horizontal gaze palsy
Horizontal gaze palsy plus internuclear ophthalmoplegia One-and-a-half syndrome
Diffuse extraocular muscle weakness Chronic progressive external ophthalmoplegia
Fig. 1. Left upper eyelid retraction contralateral to a ptotic right upper eyelid be- cause of Hering’s law.
진행성 외안근마비는 병력상 서서히 진행하면서 증상의 기복이 없고, 단속운동 속도가 근무력증에 비해 더 느린 것이 감별점이다. Bell 현상 (눈을 힘껏 감을 때 눈동자가 위로 올라가는 현상) 역시 근무력증 환 자에서 없거나 감소될 수 있다. 이는 상방주시 장애 정도와 비례한다 고 알려져 있다.
11근무력증 환자에서 단속운동을 반복적으로 시킬 경우, 초기에는 정상이지만 결국 단속운동의 속도와 크기가 감소하게 된다.
12단속운 동 중 피로현상(intrasaccadic fatigue)이란 큰 단속운동 도중에 단속운 동 속도가 감소하여 서서히 시표에 도달하는 현상(Fig. 2)으로 이때 단 속운동의 기간(duration) 역시 증가한다.
13이는 연축 근섬유(twit ch fi- ber) 의 피로에 의한 것이다. 오히려 작은 단속운동의 속도는 비정상적 으로 증가하는 현상을 관찰할 수 있다. 단속운동 속도 또는 단속운동 크기에 대한 속도 역시 가변성(variability) 을 보일 수 있는데(saccadic jitter) 이는 근무력증 환자에 진단적 가치가 있다.
14단속운동의 궤적 (trajectory) 역시 변동 정도가 증가하며, 지속적 주시 후에는 단속운동 크기가 감소한다.
15긴장성 근섬유(tonic fiber)의 피로현상으로 편향된 위치에서 주시가 유지되지 못하는 경우 단속운동 후 glissadic drift가 반대 방향으로 발행하며 이를 ‘quiver’ 현상이라 한다.
16Quiver 현상은
작은 단속운동 시 더 잘 나타난다. 동일한 이유에서 지속적 편향 주시 시 주시유발 안진(gaze-evoked nystagmus)이 나타날 수 있다.
17또한, 큰 단속운동은 겨냥과소(hypometria)가 나타나는 반면, 작은 단속운동 은 겨냥 과다(hypermetria)가 나타나는데, 이는 근위약에 대한 중추 성 보상 기전에 의한 것이다.
184) 동공 및 모양체
근무력증 환자의 동공과 모양체(pupil and ciliary body) 침범에 대해 서는 아직 이론이 있다. 대부분 임상적으로 동공침범은 뚜렷하지 않 으며 , 이는 안구형 근무력증과 다른 유사 질환과의 감별에도 중요한
10° right 0°
10° left 1 sec
Fig. 2. Slow and hypometric saccades in a patient with ocular myasthenia. The patient is making saccades to follow a target (dotted line) making 20-degree steps repetitively. Black lines show his eye position (y-axis) over time (x-axis).
Occasional intrasaccadic fatigue (arrow) is shown.
Table 2. Comparison of diagnostic tests for myasthenia gravis
Test Sensitivity Specificity Advantage Disadvantage
N ot as well-studied for ophthalmoparesis as for ptosis
90% (for ptosis) 100%
(for ptosis) Office base Non invasive Inexpensive Safe Simple
G reater improvement in ptosis than seen with rest test
Sleep test 100% 100% Office base Ties up an exam room for a half hour
Non invasive Inexpensive Safe Simple
Rest test 50% 100% Much quicker than sleep test Less ptosis improvement than ice test
E drophonium or neostigmine test
OM: 86-97% OM: 83% Office base Side effect
GM: 82-100% Most useful with ptosis and ophthalmoparesis IV access
Well-studied Monitoring of pulse and blood pressure
A cetylcholine receptor antibody
OM: 25-75% -100% Most specific Less sensitive for OM than GM
GM: 80-99% Expensive
RNS OM: 15-50% OM: 89% Widely available Uncomfortable
GM: 71% Low sensitivity
P ositive test means neuromuscular junc- tion disorder, not specific for MG SFEMG OM: 62-100% (frontalis, orbicularis
oculi, superior rectus-levator complex muscle)
MG: 89% Most sensitive Uncomfortable
GM: 90% N eed experienced electrophysiologist
with special equipment
의미를 갖는다. 그럼에도 근무력증 환자에서 동공 부등(anisocoria)이 보고된 바가 있고 이는 콜린에스터라제 저해제 사용 시 호전되었다.
19동공 빛반사(pupillary light reflex)의 속도가 느려지거나,
20지속적 빛 자극 시 동공수축 (pupil constriction)의 피로 현상
21이 보고되었다. 또 한 지속적 눈모음 (convergence)으로 축동(accommodation) 피로 현상 이 유발된 예가 있으며, 이는 edrophonium 투약 후 호전되었다.
222. 진단 방법
중증근무력증은 일반적으로, 전기생리학적 검사(반복자극검사, 단일근섬유 근전도), 아세틸콜린 수용체 항체 검사, 아세틸콜린 분해 억제제에 대한 반응 등으로 진단할 수 있다. 그러나 안구형 근무력증 의 경우 상기 검사의 민감도가 전신형 근무력증에 비해 낮아 진단이 용이하지 않다. 중증근무력증의 진단법과 각각의 민감도 및 특이도 는 Table 2에 요약하였다. 여기에서는 각빙 검사(ice cube test), 수면 검 사 (sleep test), 휴식 검사(rest test)에 대해 간단하게 기술하였다.
1) 각빙 검사
각빙 검사(ice cube test)는 안구주변근육을 얼음 조각으로 국소 냉 각하여 , 안구형 근무력증을 진단하는데 빠르고, 안전하고, 저렴하면 서도 민감도와 특이도가 매우 높은 검사이다.
23-25온도가 떨어지면 아 세틸콜린에스터라제의 활동성이 감소하여 신경근 접합부에 아세틸 콜린의 양이 증가하고, 이로 인해 근무력증이 호전되는 것을 원리로
한다 . 눈을 감은 상태에서 얼음 조각을 2-5분간(안검하수에는 2분, 외 안근 마비에는 5분간) 환자의 눈꺼풀 위에 댄 뒤 안검하수와 외안근 마비의 호전 정도를 관찰한다. 얼음 조각 적용 전후로 사진을 찍어 객 관적으로 기록하는 것이 중요하다. 안검하수의 경우 2 mm 이상 호전 을 보이는 경우 근무력증을 진단할 수 있는데(Fig. 3), 보통 1분 이내에 이전 상태로 돌아간다. 각빙 검사는 외안근 마비보다는 안검하수에 서 더욱 진단적 가치가 있는데, 이는 안구 운동 제한 정도 및 안구 정렬 정도의 호전을 정확히 측정하기 어렵기 때문이다.
2) 수면 검사
환자를 어둡고 조용한 방에 30분간 수면을 취하게 한 뒤 증상의 호 전 여부를 알아보는 검사이다. 역시 검사 전후로 안검하수와 외안근 마비 등을 사진으로 찍어 객관적으로 기록해야 한다. 수면 검사(sleep test)는 안구형 근무력증 환자에서 edrophonium test보다 민감도가 더 높은 것으로 보고된 바 있다.
263) 휴식 검사
간이 수면 검사로 2-5분간 눈을 감고 난 뒤 증상의 호전 여부를 알 아보는 검사이다. 일부에서는 각빙 검사 역시 냉각에 의해서가 아니 라 눈을 감은 상태로 검사를 하므로 휴식에 의해 증상이 호전되는 것 이라는 주장이 있다. 실제 같은 방법으로 뜨거운 팩을 얼음 조각 대신 적용하였을 때도 유사한 정도의 증상 호전을 보였기 때문이다.
27휴식
A B
C
Fig. 3. Ice test. (A) Preceding the test, bilateral asymmetric upper eyelid ptosis is present, much worse on the left. (B) An ice pack is applied to the closed left eye for 2 minutes. (C) After the application of ice, the left upper eyelid ptosis is significantly improved.
검사 (rest test)와 각빙 검사를 비교한 연구에서, 정상군에서는 두 군 모 두 음성을 보인 반면, 근무력 환자군에서는 휴식 검사 시 평균 2 mm, 각빙 검사시 4.5 mm 정도로 안검하수가 호전되었다.
28근위축성 측색 경화증
고전적으로 근위축성 측색 경화증(amyotrophic lateral sclerosis, ALS) 환자는 인공호흡기로 생명이 연장된 환자를 제외하고 안구운동 이 보존된다고 알려져 있었다.
29그러나 최근 20년간 보고된 바에 의하 면 ALS에서도 다른 신경계 퇴행성 질환과 마찬가지로 다양한 정도의 안구운동장애가 있음이 밝혀졌다. 본문에서는 ALS 환자에서 보이는 단속운동 (saccade), 원활추종운동(smooth pursuit), 시선고정(ocular fixation)장애와 안근마비(ophthalmoplegia)에 대해 살펴보고 이들 안
구운동장애가 ALS와 ALS 유사 질환장애를 감별하고 정확한 진단을 하는 데 유용한지에 대해 알아보기로 한다.
1. ALS에서 단속운동장애
단속운동 (saccade)이란 선명한 시력을 유지하기 위해 시선을 빨리 이동하여 관심대상이 되는 물체를 망막의 중심오목(fovea)에 맺히게 하는 안구운동이다. 몇 가지 패러다임으로 단속운동을 검사할 수 있 는데 , 본문에서는 반사적 단속운동(reflexive: visually-guided saccade) 과 자발적 단속운동(volitional: memory-guided saccade and antisac- cade)장애에 대해 기술하였다.
1) ALS에서 반사적 단속운동장애
이전까지 ALS 환자에서 반사적(reflexive: visually-guided) 단속운
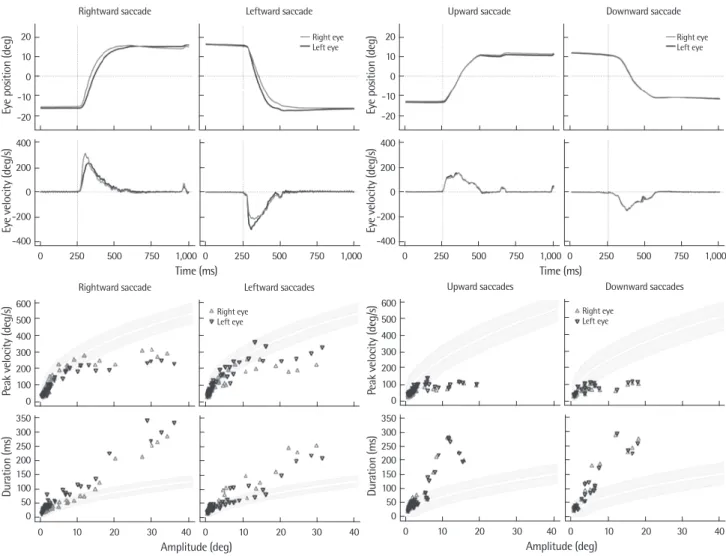
Fig. 4. Saccadic abnormalities in a 70-year-old man with bulbar onset amyotrophic lateral sclerosis. Eye movement recordings using the magnetic search coil tech- nique revealed slowing and reduced amplitude of vertical saccades. Horizontal saccades were also mildly slowed, with saccades of the adducting eye being slower than those of the abducting eye, giving the appearance of bilateral internuclear ophthalmoplegia. Shaded zones indicate the 95% prediction intervals for a group of normal control subjects, with the white line indicating the mean.
Time (ms) 20
10 0 -10 Eye position (deg) -20
Rightward saccade
400 200 0 -200 Eye velocity (deg/s)-400
0 250 500 750 1,000 0 250 500 750 1,000
Leftward saccade
Right eye Left eye
Amplitude (deg) 600
500 400 300 200 100 Peak velocity (deg/s) 0
Rightward saccade
350 300 250 200 150 100 50 0
Duration (ms)
0 10 20 30 40 0 10 20 30 40
Leftward saccades Right eye
Left eye
Amplitude (deg) 600
500 400 300 200 100 Peak velocity (deg/s) 0
Upward saccades
350 300 250 200 150 100 50 0
Duration (ms)
0 10 20 30 40 0 10 20 30 40
Downward saccades
Right eye Left eye
Time (ms) 20
10 0 -10 Eye position (deg) -20
Upward saccade
400 200 0 -200 Eye velocity (deg/s)-400
0 250 500 750 1,000 0 250 500 750 1,000 Downward saccade
Right eye Left eye
동은 정상이라고 알려져 있었다. 그러나 bulbar onset ALS환자에서 spinal onset 환자에 비해 반사적 단속운동의 최대 속도(peak velocity) 가 느려져 있음이 관찰되었으며(Fig. 4),
30특히 급속히 진행하는 ALS 환자 10명 중 2명에서 느린 단속운동이 관찰되었다.
31동일 연령 대조 군 비교에서도 9명 중 4명의 ALS 환자에서 단속운동이 느려져 있었 다 .
32단속운동의 pulse가 뇌간에서 생성됨을 고려할 때 ALS 환자에서 보이는 느린 단속운동은 뇌간 자체에 병태생리로 발생한다고 추정할 수 있다.
2) ALS에서 자발적(volitional: memory-guided and antisaccade) 단속운동장애
Memory-guided saccade는 시표를 시야의 주변부에 수초간 보여준 뒤 사라지게 한 다음 주변부에 나타났던 시표의 위치를 기억하여 바 라보게 하는 검사이다. ALS 환자는 short-term memory-guided sac- cade (시표를 수초 전에 보여 준 뒤 검사)의 반응시간(latency)이 연장 되어 있는 반면, 정확도(accuracy)는 정상이다.
33Antisaccade는 제시된 시표의 정반대 방향을 바라보게 하여 검사하는데, 예를 들면 중심에 서 10도 좌측에 시표를 보여줄 때 실제 우측 10도 위치로 단속운동을 수행하는 것이다. ALS 환자는 antisaccade의 정확도가 감소하고 반응 시간이 연장되는데,
30, 33특히 type I error (부정확한 antisaccade 후 이를 스스로 교정하지 못함)가 증가하는 것으로 알려져 있다.
30또한 type I error율은 Stroop test 및 bulbar subscore 를 포함하는 Amyotrophic
Lateral Sclerosis Functional Rating Scale과도 비례하는 것으로 나타났 다 . Antisaccade는 전두안영역(frontal eye field, FEF)과 배측외측전전 두엽 (dorsolateral prefrontal cortex, DLPC)에서 담당하는데 FEF는 주 로 antisaccade의 반응시간을, DLPC는 주로 error율을 조절한다.
34즉, ALS 환자에서 antisaccade의 장애는 이 두 영역의 장애로 인한 것으로 생각할 수 있다. 또한 DLPC는 short-term memory-guided saccade의 생성과도 관련된다고 알려져 있어,
34ALS 환자에서 나타나는 자발적 단속운동의 장애는 전두엽 기능 이상에 의한 것이라 할 수 있다. 신경 심리검사상 임상적으로 치매가 없는 ALS 환자의 50%가 전두엽 기능 이상을 보였으며,
35임상병리연구에서 ALS와 전두측두엽치매가 하나 의 질환 스펙트럼상에 있음을 시사하는 소견이 발견되었다는 점
36도 ALS 환자에서의 자발적 단속운동장애가 전두엽기능장애로부터 기 인하는 것임을 시사하는 소견이다.
2. ALS에서 원활추종운동장애
원활추종운동 (smooth pursuit)은 생리학적으로 초기 가속기(pur- suit initiation)와 유지기(pursuit maintenance)로 구분할 수 있다. 대부 분의 연구는 ALS 환자에서 원활추종운동 유지기의 속도 이득(veloci- ty gain)이 감소됨을 보고하였다.
31, 37, 38반면 Shaunak 등
33은 예측가능 한 triangular waveform stimulus를 이용하여 검사하였을 때, 원활추 종운동의 속도 이득이 정상이라 주장하였다. 또 다른 연구에서는 파 킨슨 양상을 동반한 ALS 환자에서만 속도 이득이 감소하며, 산발성
-2 -3 -4 -5 -6 -7 -8
Position (degrees)
Time (ms)
0 2,000 4,000 6,000 8,000 10,000
Fixation period Saccadic
intrusion
5 4 3 2 1 0 -1
Position (degrees)
Time (ms)
10,000 12,000 14,000 16,000 18,000 20,000
Fixation period Saccadic
intrusion
100.00
10.00
1.0 1.00E-5
VFI (s letters)
GMSIA ON (degrees)
0.00 0.50 1.00 1.50 2.00 2.50
A B
Fig. 5. (A) Saccadic intrusions, measured by their amplitude (degrees) and fixation periods (milliseconds) are depicted by arrows. The top record is from a MND patient revealing larger amplitude saccadic intrusions compared to the record below from a control subject. (B) Scatter plot highlighting the correlation between GMSIA ON and VFI (s letters). Regression coefficient, R= 0.33. GMSIA ON Geometric mean saccadic intrusion amplitude with the target stimulus on (degrees); VFI Verbal Fluency Index (seconds).
ALS 환자에서는 정상이라 보고한 바 있다.
39그러나 대부분의 ALS 환 자에서 원활추종운동의 속도 이득은 감소하며 이는 따라잡기 단속 운동 (catch-up saccade) 으로 대체되는 경향을 보인다.
40원활추종운 동은 대뇌에서 시작하여 교뇌 및 소뇌를 거치는 해부학적 경로를 통 해 이루어지며, 속도 이득은 정상 노인을 비롯하여 파킨슨 증후군, 알 츠하이머 치매, 전두측두엽치매, 소뇌 기능 이상 질환, 대사성 뇌병증 및 약물 중독 등 다양한 상황에서 감소할 수 있다.
34따라서 원활추종 운동의 속도 이득 감소가 진단 특이적이라 하기는 어렵다. 그러나 전 두안영역을 미세전기자극 하였을 때 원활추종운동의 속도 이득이 조 절되는 현상을 근거로,
41ALS 환자에서 속도 이득 감소는 전두안영역 기능 이상으로 설명할 수 있다.
3. ALS에서 시선고정장애
1) 단속운동 간섭ALS 환자에서는 사각파된떨림(square wave jerk)의 빈도가 동일 연 령 대조군에 비해 증가됨이 알려져 있다.
33특히 ALS 환자의 시선고정 (ocular fixation)장애를 정량화한 연구에서, 단속운동 간섭(saccadic intrusion)의 크기(amplitude)가 증가 할 뿐 아니라, 증가 정도는 전두엽 기능장애를 반영하는 유창성 검사와 Stroop 검사 점수와 비례함을 보고하였다 (Fig. 5).
42단속운동 간섭은 단속안구운동 경로의 이상으 로 발생한다. 실제, 문측 상구(rostral pole of superior colliculus), 중뇌 그물체 (mesencephalic reticular formation), 소뇌 꼭지핵(fastigial nucle- us)과 기저핵(basal ganglia) 병변시 단속운동 간섭이 발생하는 것으로 알려져 있다.
34문측 상구로 투사하는 전두안영역 역시 지속적 시선고 정 시 불필요한 단속운동을 억제하는 기능을 하므로 이 부위의 병변 으로도 단속운동 간섭이 유발될 수 있다.
34ALS 환자에서 단속운동 간섭의 크기와 전두엽 기능 이상 정도가 비례하는 점을 고려하였을 때 , ALS 환자에서 단속운동 간섭은 전두-상구 경로의 침범으로 발생 한다 하겠다.
2) 안진
안진 (nystagmus)은 ALS 환자에서 매우 드문 소견이다. 한 증례보고 에서 주시유발안진(gaze-evoked nystagmus)을 보인 ALS 환자가 핵상 안구마비 (supranuclear ophthalmoplegia)와 수평 안진으로 진행된 예 를 보고하였고, 안구마비 없이 주시유발안진만 있었던 예를 기술한 바 있다.
43그러나 이들 중 한 명은 부검 결과 소장의 악성종양이 발견 되어 , 안진이 부종양증후군(paraneoplastic syndrome)과 관련하여 발 생하였을 가능성을 배제하기 어렵다. 또 다른 연구에서는 하부운동 신경원 증후군(lower motor neuron syndrome) 양상을 보인 세 명의 환 자가 하방 안진(downbeat nystagmus)을 보인 사례를 보고하였다.
44그
러나 이들 중 한 명은 소뇌 위축이 있고 자세 불균형이 주증상이었으 므로 , 전기생리학적으로는 ALS에 합당하다 하더라도 다른 질환군일 가능성이 높다. 즉, ALS가 의심되는 환자에서 안진을 보일 경우에는 이를 가장할 수 있는 다른 질환을 의심하는 것이 더욱 타당할 것이다.
4. 안근마비
안근마비 (ophthalmoplegia)는 인공호흡기를 이용하여 생명이 장기 간 연장되었던 일부를 제외하면 ALS 환자에서 드문 소견이다.
29Har- vey 등
45은 외안근마비가 질환 초기에 나타나 사망전까지 완전한 외안 근마비로 진행된 증례를 보고한 바 있다. 이 환자의 부검결과에서 안 구운동핵에 광범위한 신경세포 소실과 교세포증식(gliosis)이 관찰되 었다 . ALS에서 안구운동핵은 척수운동핵에 비해 상대적으로 보존된 다고 알려져 있다.
46이를 설명하는 가설로 흥분성 글루타메이트 신경 전달물질 , 칼슘 결합 단백질, 영양 요소(trophic factor), 안드로젠 수용 체의 분포 정도의 차이가 제시되었으나, 아직 기전은 확실하지 않다.
5. ALS 유사 질환에서의 안구운동장애
1) 진행성 핵상마비ALS 환자에서도 진행성 핵상마비(progressive supranuclear palsy)에 서 보이는 느린 단속운동과 핵상안구마비를 보일 수 있을 뿐 아니
라 ,
47-50진행성 핵상마비에서 흔히 동반되는 단속운동 간섭, antisac-
cade error 증가, 원활추종운동 이득 감소를 보이므로 이와의 감별이 필요하다 .
2) 케네디 병
케네디 병(Kennedy’s disease)은 성염색체 연관 열성 유전 질환으로 구와 척수의 하부운동원을 침범하여 후발성 근위축을 유발한다. 케 네디 병은 진행속도가 상대적으로 느리고, 추체로를 침범하지 않는다 는 점에서 ALS 와 감별이 가능하다. 최근 케네디 병에서는 수직/수평 방향의 반사적 신속운동이 감소되는 반면, 다른 안구운동은 보존되 어 있음이 알려져
51ALS와의 감별이 필요하다.
REFRENCES
1. Bever CT Jr, Aquino AV, Penn AS, Lovelace RE, Rowland LP. Prognosis of ocular myasthenia. Ann Neurol 1983;14:516-519.
2. Oosterhuis HJ. The natural course of myasthenia gravis: a long term fol- low up study. J Neurol Neurosurg Psychiatry 1989;52:1121-1127.
3. Gorelick PB, Rosenberg M, Pagano RJ. Enhanced ptosis in myasthenia gravis. Arch Neurol 1981;38:531.
4. Silver S, Osserman KE. Hyperthryoidism and myasthenia gravis. J Mt Si
nai Hosp 1957;24:1214-1220.
5. Puklin JE, Sacks JG, Boshes B. Transient eyelid retraction in myasthenia
gravis. J Neurol Neurosurg Psychiatry 1976;39:44-47.
6. Breen LA, Gutmann L, Brick JF, Riggs JR. Paradoxical lid elevation with sustained upgaze: a sign of Lambert-Eaton syndrome. Muscle Nerve 1991;
14:863-866.
7. Cogan DG. Myasthenia Gravis: a review of the disease and a description of lid twitch as a characteristic sign. Arch Ophthalmol 1965;74: 217-221.
8. Osher RH, Griggs RC. Orbicularis fatigue: the ‘peek’ sign of myasthenia gravis. Arch Ophthalmol 1979;97:677-679.
9. Weinberg DA, Lesser RL, Vollmer TL. Ocular myasthenia: a protean dis- order. Surv Ophthalmol 1994;39:169-210.
10. Brust JC, List TA, Catalano LW, Lovelace R. Ocular myasthenia gravis mimicking progressive external ophthalmoplegia. Rare case of myasthe- nia associated with peripheral neuropathy and spastic paraparesis. Neu
rology 1974;24:755-760.
11. Miller NR, Griffin J, Cornblath D, Guerin C. Intact Bell’s phenomenon in a patient with myasthenia gravis and upward gaze paresis. Arch Ophthal
mol 1989;107:1117.
12. Baloh RW, Keesey JC. Saccade fatigue and response to edrophonium for the diagnosis of myasthenia gravis. Ann N Y Acad Sci 1976;274:631-641.
13. Schmidt D, Dell’Osso LF, Abel LA, Daroff RB. Myasthenia gravis: saccad- ic eye movement waveforms. Exp Neurol 1980;68:346-364.
14. Barton JJ, Sharpe JA. ‘Saccadic jitter’ is a quantitative ocular sign in myas- thenia gravis. Invest Ophthalmol Vis Sci 1995;36:1566-1572.
15. Sollberger CE, Meienberg O, Ludin HP. The contribution of oculography to early diagnosis of myasthenia gravis. A study of saccadic eye move- ments using the infrared reflection method in 22 cases. Eur Arch Psychia
try Neurol Sci 1986;236:102-108.
16. Cogan DG, Yee RD, Gittinger J. Rapid eye movements in myasthenia gra- vis. I. Clinical observations. Arch Ophthalmol 1976;94:1083-1085.
17. Spooner JW, Baloh RW. Eye movement fatigue in myasthenia gravis. Neu
rology 1979;29:29-33.
18. Yee RD, Cogan DG, Zee DS, Baloh RW, Honrubia V. Rapid eye move- ments in myasthenia gravis. II. Electro-oculographic analysis. Arch Oph
thalmol 1976;94:1465-1472.
19. Herishanu Y, Lavy S. Internal ‘ophthalmoplegia’ in myasthenia gravis.
Ophthalmologica 1971;163:302-305.
20. Yamazaki A, Ishikawa S. Abnormal pupillary responses in myasthenia gravis. A pupillographic study. Br J Ophthalmol 1976;60:575-580.
21. Dutton GN, Garson JA, Richardson RB. Pupillary fatigue in myasthenia gravis. Trans Ophthalmol Soc U K 1982;102(Pt 4):510-513.
22. Manson N, Stern G. Defects of near vision in myasthenia gravis. Lancet 1965;1:935-937.
23. Sethi KD, Rivner MH, Swift TR. Ice pack test for myasthenia gravis. Neu
rology 1987;37:1383-1385.
24. Ertas M, Arac N, Kumral K, Tuncbay T. Ice test as a simple diagnostic aid for myasthenia gravis. Acta Neurol Scand 1994;89:227-229.
25. Golnik KC, Pena R, Lee AG, Eggenberger ER. An ice test for the diagno- sis of myasthenia gravis. Ophthalmology 1999;106:1282-1286.
26. Odel JG, Winterkorn JM, Behrens MM. The sleep test for myasthenia gra- vis. A safe alternative to tensilon. J Clin Neuroophthalmol 1991;11:288- 27. Movaghar M, Slavin ML. Effect of local heat versus ice on blepharoptosis 292.
resulting from ocular myasthenia. Ophthalmology 2000;107:2209-2214.
28. Kubis KC, Danesh-Meyer HV, Savino PJ, Sergott RC. The ice test versus the rest test in myasthenia gravis. Ophthalmology 2000;107:1995-1998.
29. Mizutani T, Aki M, Shiozawa R, Unakami M, Nozawa T, Yajima K, et al.
Development of ophthalmoplegia in amyotrophic lateral sclerosis during long-term use of respirators. J Neu rol Sci 1990;99:311-319.
30. Donaghy C, Pinnock R, Abrahams S, Cardwell C, Hardiman O, Patter-
son V, et al. Slow saccades in bulbar-onset motor neurone disease. J Neu
rol 2010;257:1134-1140.
31. Leveille A, Kiernan J, Goodwin JA, Antel J. Eye movements in amyotro- phic lateral sclerosis. Arch Neurol 1982;39:684-686.
32. Ohki M, Kanayama R, Nakamura T, Okuyama T, Kimura Y, Koike Y.
Ocular abnormalities in amyotrophic lateral sclerosis. Acta Otolaryngol Suppl 1994;511:138-142.
33. Shaunak S, Orrell RW, O’Sullivan E, Hawken MB, Lane RJM, Henderson L, et al. Oculomotor function in amyotrophic lateral sclerosis: eviden ce for frontal impairment. Ann Neurol 1995;38:38-44.
34. Leigh RJ, Zee DS. The neurology of eye movements. 4 ed. New York: Ox- ford University Press; 2006.
35. Ringholz GM, Appel SH, Bradshaw M, Cooke NA, Mosnik DM, Schulz PE. Prevalence and patterns of cognitive impairment in sporadic ALS.
Neurology 2005;65:586-590.
36. Geser F, Lee VM, Trojanowski JQ. Amyotrophic lateral sclerosis and fron- totemporal lobar degeneration: a spectrum of TDP-43 proteinopathies.
Neuropathology Apr 2010;30:103-112.
37. Abel LA, Williams IM, Gibson KL, Levi L. Effects of stimulus velocity and acceleration on smooth pursuit in motor neuron disease. J Neurol 1995;242:419-424.
38. Marti-Fabregas J, Roig C. Oculomotor abnormalities in motor neuron disease. J Neurol 1993;240:475-478.
39. Gizzi M, DiRocco A, Sivak M, Cohen B. Ocular motor function in motor neuron disease. Neurology 1992;42:1037-1046.
40. Jacobs L, Bozian D, Heffner RR, Jr, Barron SA. An eye movement disor- der in amyotrophic lateral sclerosis. Neurology 1981;31:1282-1287.
41. Tanaka M, Lisberger SG. Regulation of the gain of visually guided smooth- pursuit eye movements by frontal cortex. Nature 2001;409:191-194.
42. Donaghy C, Pinnock R, Abrahams S, Cardwell C, Hardiman O, Patter- son V, et al. Ocular fixation instabilities in motor neurone disease. A marker of frontal lobe dysfunction? J Neurol 2009;256:420-426.
43. Kushner MJ, Parrish M, Burke A, Behrens M, Hays AP, Frame B, et al.
Nystagmus in motor neuron disease: clinicopathological study of two cases. Ann Neurol 1984;16:71-77.
44. Thakore NJ, Pioro EP, Rucker JC, Leigh RJ. Motor neuronopathy with dropped hands and downbeat nystagmus: a distinctive disorder? A case report. BMC Neurol 2006;6:3.
45. Harvey DG, Torack RM, Rosenbaum HE. Amyotrophic lateral sclerosis with ophthalmoplegia. A clinicopathologic study. Arch Neurol 1979;36:
615-617.
46. Kaminski HJ, Richmonds CR, Kusner LL, Mitsumoto H. Differential sus- ceptibility of the ocular motor system to disease. Ann N Y Acad Sci 2002;
956:42-54.
47. Averbuch-Heller L, Helmchen C, Horn AK, Leigh RJ, Buttner-Ennerver JA. Slow vertical saccades in motor neuron disease: correlation of struc- ture and function. Ann Neurol 1998;44:641-648.
48. Okuda B, Yamamoto T, Yamasaki M, Maya K, Imai T. Motor neuron dis- ease with slow eye movements and vertical gaze palsy. Acta Neurol Scand 1992;85:71-76.
49. Ushio M, Iwasaki S, Sugasawa K, Murofushi T. Atypical motor neuron disease with supranuclear vertical gaze palsy and slow saccades. Auris Nasus Larynx 2009;36:85-87.
50. Kobayashi M, Ikeda K, Kinoshita M, Iwasaki Y. Amyotrophic lateral scle- rosis with supranuclear ophthalmoplegia and rigidity. Neurol Res 1999;21:
661-664.
51. Thurtell MJ, Pioro EP, Leigh RJ. Abnormal eye movements in Kennedy disease. Neurology 2009;72:1528-1530.