Characteristics of Hematopoitic Growth Factor, G-CSF and Its Clinical Vision
Jeonghae Park1, Jung-Ae Park1, Seok-Woo Kang2, Tae-Won Goo2 and Kyung Tae Chung1*
1Department of Clinical Laboratory Science, Dong Eui University, Busan 614-714, Korea
2Department of Agricultural Biology, National Academy of Agricultural Science, RDA, Suwon, 441-100, Korea.
Received November 17, 2011 /Revised November 25, 2011 /Accepted November 25, 2011
The production of blood cells is regulated by more than 20 different growth factors, called hema- topoitic growth factors. These factors have been produced in prokaryotic and mammalian systems for their clinical use. Glranulocyte-Colony Stimulating Factor (G-CSF) is an important therapeutic factor for cancer patients as well as patients with congenital conditions. These patients do not have enough neutrophils and have a high risk of infection. Two groups of recombinant G-CSF have been used to specially treat cancer patients after chemotherapy because chemotherapy induces neutropenia, a major side effect of chemotherapy drugs. Here, structural and biological characteristics of G-CSF are presented. In addition, the relationship between chemotherapy and neutropenia, which is a severe reduction of neutrophils in the blood, and clinical application of G-CSF is discussed. Recombinant G-CSFs are grouped in two forms. Non-glycosylated G-CSF, filgrastim, is produced inEscherichia coli and glycosylated G-CSF, lenograstim, is produced in Chinese hamster ovary cells. Differences in struc- ture and biological activity are compared and challenges for biosimilar production are also highlighted.
Key words : G-CSF, chemotherapy, filgrastim, lenograstim, biosimilar
*Corresponding author
*Tel:+82-51-890-2681, Fax:+82-51-890-2622
*E-mail : [email protected]
서 론
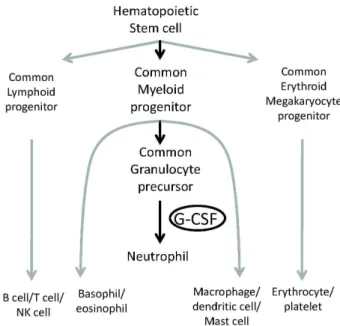
혈액세포는 골수에서 매우 빠르게 생산이 된다. 일반적으 로 2.5×108cells/min 속도로 성숙한 혈액세포가 만들어 진다 고 알려져 있다[3]. 혈액세포는 수명이 각각 다른데, 적혈구는 몇 주간 생존이 가능하나 과립구 세포(granulocyte)는 단지 몇 시간만 생존한다. 혈액세포의 생성은 골수에서 조혈모세 포(또는 조혈줄기세포)에서 여러 단계의 분화과정을 거쳐 이 루어지며 미세환경조건에서 다양한 성장과 분화자극인자들 이 이 과정을 조절한다. 이들 분화자극인자들은 당단백질로 서 ‘조혈성장인자(hematopoietic growth factor)’라고 하며 단 독으로 기능을 나타내거나 공동으로 작용하기도 한다. 이들 조혈성장인자들에는 interleukin (IL-1, IL-3)과 SCF (stem cell factor), erythropoietin (EPO), granulocyte-colony stimulat- ing factor (G-CSF), macrophage-colony stimulating factor (M-CSF), macrophage and granulocyte-colony stimulating factor (GM-CSF) 등 20여 가지 이상이 존재한다[13]. 혈구세 포 분화과정을 Fig. 1에 간략하게 나타내었으며, 다양한 조혈 성장인자들이 각 단계별로 단독 또는 공동작용을 하여 분화 를 조절한다. 이 총설에서는 G-CSF에 중점을 두고 있음으로 함축성과 강조를 위하여 G-CSF가 작용하는 중요한 단계만 표시하였으며, 또한 G-CSF의 기능, 임상적 응용, 재조합 단백 질의 생산에 주안점을 두고 기술하였다.
Fig. 1. Diagram depicted on G-CSF step in neutrophil differ- entiation during hematopoiesis.
G-CSF 기능과 구조
G-CSF는 colony-stimulating factor 3이라고도 알려져 있 으며, 여러 세포에서 생산되어 골수를 자극하여 조혈줄기세 포와 granulocyte를 생산하고 호중구세포(neutrophil)의 전 구세포와 성숙세포의 분열과 분화에 절대적으로 작용하는 조혈성장인자이다(Fig. 1). 사람 G-CSF 단백질은 granulocyte - Review -
증식인자로 1986년에 분리되었으며, cDNA도 제작되었다 [20,35]. 또한 G-CSF가 결여된 생쥐에서 심각한 호중구세포 감소증을 나타내어 그 기능을 재확인하였다[14]. G-CSF 유전 자는 chromosome 17에 존재하며, alternative splicing으로 두 종류의 단백질이 생산되는데 이들은 3 개의 아미노산 존 재 여부에 따라 나누어진다. Fig. 1은 짧은 G-CSF의 아미노 산 순서를 나타내고 있으며, 긴 G-CSF에는 Fig. 1A의 35번과 36번인 leucine과 cysteine 사이에 3 개의 아미노산 va- line-serine-glumatic acid가 첨가 되어 있다. 두 종류의 G-CSF는 기능상에서 동일한 작용을 하나 활성은 짧은 G-CSF가 높다는 보고가 있다[21].
G-CSF 구조는 역평행 알파-helix 구조를 하고 있다. 4 개의 알파-helix는 각각 A, B, C, D로 명명되었으며, Helix A은 11-39번, Helix B는 71-91번, Helix C는 100-123번, Helix D는 143-171번 사이의 아미노산으로 되어 있다. 이들 4 개 helix는 loop로 서로 연결되어 있는데 A와 B, C와 D를 연결하는 loop 가 B와 C를 연결하는 loop보다 더 길다. 이 외에 Helix A와 Helix B 사이에 짧은 Helix가 존재한다. 역평행 구조를 하고 있으나 helix들이 up-down-up-down이 아닌 up-up-down- down 배열을 하고 있다. 이러한 배열은 다른 조혈성장인자인 M-CSF, GM-CSF, IL-4에서도 발견이 되어 조혈성장인자의 공 통적인 골격 구조로 간주된다[7,26,31,36]. 두 개의 disulfide bond가 cysteine 36과 42, 64와 74 사이에 형성되어 있으며, G-CSF의 활성에 아주 중요한 것 밝혀졌다[17]. 실예로서, Cysteine 64-cystein 74 결합이 결여되면 alpha-helix의 절반이 형성되지 못하며 기능도 상실하는 것으로 알려졌다. 당쇄의 부가는 소포체에서 일어나는 N-glycosylation과 골지체(Golgi Apparatus)에서 일어나는 O-glycosylation 두 가지가 있다.
G-CSF는 소포체 내에서 일어나는 N-glycosylation을 위한 Asn-X-Ser/Thr 모티브는 존재하지 않아 N-glycosylation 당 쇄는 없는 반면에, 골지체에서 일어나는 O-glycosylation이 133번 Threonine 아미노산에 일어나 당쇄가 붙어 있다[9,37].
당쇄의 기능은 활성에는 직접적인 연관성은 없으나 안정성과 관련된 것으로 간주되며 이것에 대해선 뒤 부분에서 다시 논 의하기로 한다.
치료제로서 임상적 중요성
화학적 항암치료는 빠르게 성장하는 암세포를 표적으로 하 지만 동시적으로 빠르게 성장하는 정상 혈구세포, 점막세포, 상피세포 등에도 영향을 미쳐 이들 세포의 성장 및 증식을 억제함으로써 항암제를 투여 받는 사람에게 여러 가지 병리적 현상을 초래한다. 항암제의 작용에 따라 몇 가지 그룹으로 나 누어진다. 증식하는 암세포의 DNA에 직접적으로 작용하는 alkylating agents (알킬화 제재), DNA와 RNA의 성장을 방해 하는 antimetalolite (항대사 제재), DNA 복제를 방해하는 항
Fig. 2. G-CSF structure. A. Secondary structure of G-CSF. Signal sequence, MAGPATQSPMKLMALQLLLWHSALWTVQEA, is cleaved and not present in matured G-CSF. Numbers indicate amino acid positions of matured G-CSF for each alpha-helix domain (green letters), disulfide bonds and O-glycosylation site. B. 3-Dimensional structure was viewed by Jmol program (version 12.0.41). C. Depicted diagram of 3-Dimensional structure. ●-●: disulfide bond, ◆: O-glycosylation site.
암 항생제류, 식물 유래 세포분열 억제재, 스테로이드성 약물 등이 항암제로 사용되고 있으며, 이들 대분분은 세포증식에 필요한 DNA 복제, RNA 합성 등이 표적으로 암세포 뿐만 아 니라 정상세포에도 작용을 하며, 그 중에서도 앞서 언급한 빠 르게 성장하는 정상세포에도 크다란 손상을 준다.
순환되는 혈구는 호중구(neutrophil) 40-70%, 임파구 (lymphocyte) 20-50%, 단핵구(monocyte) 2-10%, 호산구(eosi- nophil) 1-6%, 호염기성구(basophil) 1% 미만으로 구성되어 있 다[27]. 화학적 항암치료제(chemotherapy)를 투여하게 되면 백혈구 감소증이 부작용으로 나타난다. 그 중에서도 혈구의 50% 이상을 차지하는 호중구 세포의 감소증(Neutropenia)은 심각한 부작용이다. 호중구 세포 감소증은 호중구세포가 500 cells/mm3 보다 적을 경우 또는 검사 시점에는 1,000 cells/mm3보다 적으나 향후 500 cells/mm3이하로 더욱 감소 될 것으로 예상되는 경우를 말한다. 미국의 National Cancer Institute에서 규정한 neutropenia의 등급은 Table 1과 같다[6].
화학적 항암치료에 의해 유발되는 neutropenia는 흔히 발생되 는 증상으로 고형종양(solid tumor)의 경우 약 20-40%, 혈액종 양의 경우 약 50-70%로 발생한다[28].
호중구 세포가 500 cells/mm3이하로 낮아지면 미생물 감 염 위험이 심각한 수준으로 증가한다[11]. 왜냐하면 호중구 세 포는 미생물 탐식작용을 하는 기능을 보유하고 있어 선천성 면역에 중요한 부분을 차지하기 때문이다. 또한 감염상태를 나타내는 열(fever)과 함께 나타나는 neutropenia를 febrile neutropenia (FN)라고 하며, 이 같은 경우 치사율이 9.5%로
Table 1. Grades of Neutropeniaa
Grade Absolute neutrophil count (×109/l)
0 Within normal limits
1 ≥1.5 to <2.0
2 ≥1.0 to <1.5
3 ≥0.5 to <1.0
4 <0.5
aAccording to the National Cancer Institute Common Toxicity Criteria, version 2.0.3
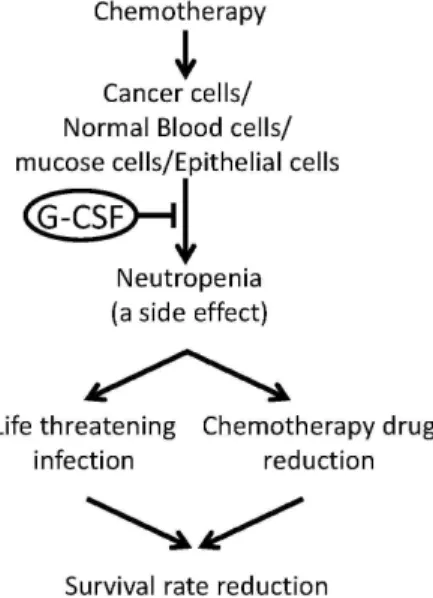
측정된 경우도 있다[4]. 암환자에게 FN이 발생하면 감염치료 가 불가피하고 따라서 FN의 억제를 위하여 항암제의 감소 역 시 피할 수 없어 항암치료가 거의 중단이 된다. 결국 감염 증가 또한 암의 악화 등으로 치사율이 증가하게 된다(Fig. 3)[15].
따라서, neutropenia가 발생한 환자에게 G-CSF를 투여하는 치료로 감소된 호중구 세포를 증식시켜 미생물에 대한 면역력 을 증가시키며 항암치료의 지연을 완화시킬 수 있다(Fig. 3).
G-CSF의 임상적 사용은 90년대 초부터 시행이 되었으며[12], 임상적 대상은 항암치료 후 neutropenia로부터 빠른 회복, 조 혈모세포 이식을 위해 공여자의 조혈모세포 증식, 조혈모세포 를 수여 받은 수혜자의 호중구 세포 회복 증대 등에 적용이 가능하다. 임상적 사용을 위하여 재조합 G-CSF가 필요하였고 1986년 재조합 G-CSF가 만들어져 상업적 사용을 위한 기반을 제공하였다[34,38].
치료제 G-CSF
여러 종류의 재조합 G-CSF가 생산되고 있으나 크게 두 종
Fig. 3. Chemotherapy-induced neutropenia and its consequence.
Recombinant G-CSF is administered to reduce neu- tropenia after chemotherapy.
류로 구별된다. 첫 번째는 Escherichia coli와 같이 세균에서 생 산되는 것과 두 번째로 Chinese hamster ovary cell에서 생산 되는 것이 있다. 세균에서 생산되는 것은 ‘Filgrastim’이라고 명명되고, Chinese hamster ovary cell에서 생산되는 것은
‘Lenograstim’이라고 명명한다. 이들 두 종류의 가장 큰 차이 점은 두 가지가 있다. 세균에서 생산되는 단백질은 세균은 진 핵세포의 소포체나 골지체에서 일어나는 당쇄부가 기능이 없 기 때문에 당단백질 합성에 제약이 있다. 따라서 Filgrastim은 사람의 G-CSF에 존재하는 O-glycosylation에 의한 당쇄가 존 재하지 않는다. 이에 반해 Lenograstim은 Chinese hamster ovary cell에서 생산됨으로 사람의 G-CSF와 같이 O-glyco- sylation에 의한 당쇄가 있으며, 분자량 대비 당쇄의 비율이 약 4%로 사람의 G-CSF과 전혀 차이가 없다[2,10,22,25]. 두 번 째의 차이점은 세균은 단백질 합성과정에서 첫 번째 아미노산 으로 진핵생물이 사용하지 않는 formylmethionine (fMet)을 사용하며, fMet은 합성된 단백질에 제거되지 않고 존재하게 된다. Filgrastim은 fMet이 G-CSF의 N-말단에 부가적으로 존 재하여 174개의 아미노산으로 구성되어 있는 것이 아니라 175 개의 아미노산으로 구성되어 있다[18,33]. 이 두 가지의 차이점 중에서 보다 논의가 심화되고 있는 것은 부가된 당쇄의 존재 여부로서 당쇄의 기능에 초점을 두고 있다. 당단백질의 당쇄 기능에 대해서는 다른 논문에서 보다 자세히 제공하기로 하고 여기서는 G-CSF의 당쇄 기능에 대해서만 설명하기로 한다.
Filgrastim과 Lenograstim의 물리적 특성을 pH와 온도 변 화에 따라 조사하였을 때 Filgrastim이 중합되는 경우가 높게 나타났으며, 이 결과는 당쇄가 당백질의 안정성에 작용을 한 다는 것을 뜻한다[23]. 또한 Filgrastim과 Lenograstim을 사 람 혈청 내에서 일정 시간 반응을 시켰을 때 단백질 분해에 대한 저항성이 Lenograstim이 높게 나타났다[24]. 이들 in vitro 실험 결과는 당쇄가 G-CSF의 in vivo에서의 안정성을 암시해 준다고 볼 수 있으며 구조분석의 실험결과도 이를 지 지해 주고 있다[8]. 그러나 이런 차이가 있음에도 불구하고 두 종류의 재조합 단백질은 세포 증식의 기능을 똑 같이 같 고 있다. Filgrastim과 Lenograstim의 생물학적 활성의 차이 가 논란이 되어 오고 있다.In vitro 호중구 세포 콜로니 형성 실험에서 Lenograstim이 약 16 배 적은 양으로도 Filgrastim 과 유사한 효과를 나타내며, 호중구 세포의 superoxide 생산 증가도 Lenograstim이 높은 것으로 보고 되었다[10].In vivo 실험결과는 동물과 사람의 경우가 다소 차이가 있는 것으로 보고되어 있다. 동물의 경우 호중구 세포 수가 두 단백질 모 두의 경우 비슷하여 활성의 차이가 없었으나, 사람의 경우 골수세포인 CD34+ 세포의 혈액으로의 이동성(mobilization) 이 Lenograstim에 의해 높게 나타난 것으로 보고 되었다[29].
따라서 G-CSF의 당쇄는 이 단백질의 안정성 뿐만 아니라 활 성에도 역할을 하는 것으로 여겨진다. 그러나 실험의 디자인 에 따라in vivo 실험 결과가 Filgrastim과 Lenograstim 두 단
백질에서 달리 나타나는 경우가 있어 임상적 사용에 대한 국 제적인 가이드 라인[1]과 활성 검정에 대한 다국적 간 검정이 진행 중에 있다[36]. 예로 현재 항암치료 후에 나타나는 neu- tropenia 치료를 위해서 유럽에서는 150 μl/kg/day의 양으 로 허가를 받아 시술하고 있으며, 일본에서는 5 μg/kg/day 양으로 시술하도록 규정되어 있다[12].
G-CSF는 조혈성장인자 중에서도 임상적으로 아주 중요한 치료제로 사용되고 있어 경제적 가치도 아주 높다. 임상적으 로는 1980년대 부터 사용이 시작되어 G-CSF의 치료방법에 대 해서는 정립이 잘 되어있다. 항암치료와 자가골수이식과 함께 G-CSF 치료를 받는 경우 대조군에 비해 백혈구 및 과립구세포 (granulocyte)의 회복속도가 빨라졌으며, 말초혈액 줄기세포 이식(peripheral-blood stem cell transplantation)의 경우에도 호중구 세포의 정착 속도 증가와 항생제 투여 감소, 입원 기간 감소와 같은 현저한 효과가 입증되었다[1,2,14,19]. 이러한 치 료 효과로 2006년 filgrastim 단일판매액이 10억 9천9백 달러 이었으며 다른 제품군의 판매액을 합산한다면 엄청난 경제성 을 가지고 있다[30].
따라서 임상적 효과 및 경제성을 바탕으로 기존의 제품 외 에도 몇몇 재조합 G-CSF 제품이 생산되어 호중구 세포 감소증 의 치료제로 유럽에서 승인을 받았으며[28], 이는 앞으로도 새 로운 재조합 G-CSF 제품이 지속적으로 개발될 가능성이 있으 며 여전히 경제적 가치가 증가될 것으로 전망된다.
Acknowledgement
본 연구는 농촌진흥청의 아젠다 프로그램 연구비 (2011DC002)에 의해 수행되었음을 감사드립니다.
References
1. Aapro, M., J. Bohlius, D. Cameron, L. Dal Lago, J. Donnelly, N. Kearney, G. Lyman, R. Pettengell, V. Tjan-Heijnen, J.
Walewski, D. Weber, and C. Zielinski. 2011. 2010 update of EORTC guidelines for the use of granulocyte-colony stim- ulating factor to reduce the incidence of chemo- therapy-induced febrile neutropenia in adult patients with lymphoproliferative disorders and solid tumours. Eur. J.
Cancer 47, 8-32.
2. Anderlini, P. 2009. Effects and safety of granulocyte col- ony-stimulating factor in healthy volunteers. Curr. Opin.
Hematol. 16, 35-40.
3. Brandt, S., W. Peters, S. Atwater, J. Kurtzberg, M. Borowitz, R. Jones, E. Shpall, R. Bast, Jr, C. Gilbert, and D. Oette. 1988.
Effect of recombinant human granulocyte-macrophage col- ony-stimulating factor on hematopoietic reconstitution after high-dose chemotherapy and autologous bone marrow transplantation. N. Engl. J. Med. 318, 869-876.
4. Cooper, K., J. Madan, S. Whyte, M. Stevenson, and R.
Akehurst. 2011. Granulocyte colony-stimulating factors for febrile neutropenia prophylaxis following chemotherapy:
systematic review and meta-analysis.BMC Cancer11, 404.
5. Cowling, G. and T. Dexter. 1992. Erythropoietin and myeloid colony stimulating factors. Trends Biotechnol. 10, 349-357.
6. Crawford, J., D. Dale, and G. Lyman. 2004. Chemotherapy-in- duced neutropenia: risks, consequences, and new directions for its management. Cancer 100, 228-237.
7. Diederichs, K., S. Jacques, T. Boone, and P. Karplus. 1991.
Low-resolution structure of recombinant human gran- ulocyte-macrophage colony stimulating factor.J. Mol. Biol. 221, 55-60.
8. Gervais, V., A. Zerial, and H. Oschkinat. 1997. NMR inves- tigations of the role of the sugar moiety in glycosylated re- combinant human granulocyte-colony-stimulating factor.
Eur. J. Biochem. 247, 386-395.
9. Hill, C., T. Osslund, and D. Eisenberg. 1993. The structure of granulocyte-colony-stimulating factor and its relationship to other growth factors. Proc. Natl. Acad. Sci. USA 90, 5167-5171.
10. Höglund, M. 1998. Glycosylated and non-glycosylated re- combinant human granulocyte colony-stimulating factor (rhG-CSF)--what is the difference?Med. Oncol. 15, 229-233.
11. Hughes, W., D. Armstrong, G. Bodey, E. Bow, A. Brown, T. Calandra, R. Feld, P. Pizzo, K. Rolston, J. Shenep, and L. Young. 2002. Guidelines for the use of antimicrobial agents in neutropenic patients with cancer.Clin. Infect. Dis. 34, 730-751.
12. Keating, G. 2011. Lenograstim: a review of its use in chemo- therapy-induced neutropenia, for acceleration of neutrophil recovery following haematopoietic stem cell transplantation and in peripheral blood stem cell mobilization. Drugs71, 679-707.
13. Kindt, T., R. Goldsby, B. Osborne, and J. Kuby. 2007. The Immune System. 6th eds. Chapter 2. W.H. Freeman, New York, NY.
14. Klumpp, T., K. Mangan, S. Goldberg, E. Pearlman, and J.
Macdonald. 1995. Granulocyte colony-stimulating factor ac- celerates neutrophil engraftment following peripheral-blood stem-cell transplantation: a prospective, randomized trial.J.
Clin. Oncol. 13, 1323-1327.
15. Kuderer, N., D. Dale, J. Crawford, L. Cosler, and G. Lyman.
2006. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients.Cancer106, 2258-2266.
16. Lieschke, G., D. Grail, G. Hodgson, D. Metcalf, E. Stanley, C. Cheers, K. Fowler, S. Basu, Y. Zhan, and A. Dunn. 1994.
Mice lacking granulocyte colony-stimulating factor have chronic neutropenia, granulocyte and macrophage progeni- tor cell deficiency, and impaired neutrophil mobilization.
Blood84, 1737-1746.
17. Lu, H., C. Clogston, L. Narhi, L. Merewether, W. Pearl, and T. Boone. 1992. Folding and oxidation of recombinant hu- man granulocyte colony stimulating factor produced in Escherichia coli. Characterization of the disulfide-reduced intermediates and cysteine-serine analogs.J. Biol. Chem. 267, 8770-8777.
18. Martin-Christin, F. 2001. Granulocyte colony stimulating fac- tors: how different are they? How to make a decision?
Anticancer Drugs 12, 185-191.
19. McQuaker, I., A. Hunter, S. Pacey, A. Haynes, A. Iqbal, and N. Russell. 1997. Low-dose filgrastim significantly enhances neutrophil recovery following autologous peripheral-blood stem-cell transplantation in patients with ymphoprolifer- ative disorders: evidence for clinical and economic benefit.
J. Clin. Oncol. 15, 451-457.
20. Nagata, S., M. Tsuchiya, S. Asano, Y. Kaziro, T. Yamazaki, O. Yamamoto, Y. Hirata, N. Kubota, M. Oheda, and H.
Nomura. 1986. Molecular cloning and expression of cDNA for human granulocyte colony-stimulating factor. Nature 319, 415-418.
21. Nagata, S., M. Tsuchiya, S. Asano, O. Yamamoto, Y. Hirata, N. Kubota, M. Oheda, H. Nomura, and T. Yamazaki. 1986.
The chromosomal gene structure and two mRNAs for hu- man granulocyte colony-stimulating factor. EMBO J. 5, 575-581.
22. Nissen, C. 1994. Glycosylation of recombinant human gran- ulocyte colony stimulating factor: implications for stability and potency. Eur. J. Cancer 30A, S12-14.
23. Oh-eda, M., M. Hasegawa, K. Hattori, H. Kuboniwa, T.
Kojima, T. Orita, K. Tomonou, T. Yamazaki, and N. Ochi.
1990. O-linked sugar chain of human granulocyte col- ony-stimulating factor protects it against polymerization and denaturation allowing it to retain its biological activity.
J. Biol. Chem. 265, 11432-11435.
24. Ono, M., M. Oh-eda, S. Kamachi, M. Kato, Y. Endo, and N. Ochi. 1992. Structure of G-CSF: significance of the sugar chain. J. Nutr. Sci. Vitaminol. (Tokyo) Spec No, 337-340.
25. Ono, M. 1994. Physicochemical and biochemical character- istics of glycosylatedrecombinant human granulocyte col- ony stimulating factor (lenograstim). Eur. J. Cancer 30A, S7-11.
26. Pandit, J., A. Bohm. J. Jancarik, R. Halenbeck, K. Koths, and S. Kim. 1992. Three-dimensional structure of dimeric hu- man recombinant macrophage colony-stimulating factor.
Science258, 1358-1362.
27. Parham, P. 2009. The Immune system, 3 eds,Garland Science, New York, NY.
28. Procopio, G., M. Niger, and I. Testa. 2011. Lecture: manage- ment of chemotherapy-induced febrile neutropenia; guide-
lines and colony stimulating factors. Neurol. Sci. [Epub ahead of print].
29. Ria, R., T. Gasparre, G. Mangialardi, A. Bruno, G. Iodice, A. Vacca, and F. Dammacco. 2010. Comparison between fil- grastim and lenograstim plus chemotherapy for mobi- lization of PBPCs. Bone Marrow Transplant45, 277-281.
30. Scrip Report. 2007. Biosimilar, Biogenerics and Follow-on Biologics. Informa UK Ltd. (http://www.scripintelligence.com/
multimedia/archive/00000/BS1342_117a.pdf)
31. Smith, L., C. Redfield, J. Boyd, G. Lawrence, R. Edwards, R. Smith, and C. Dobson. 1992. Human interleukin 4. The solution structure of a four-helix bundle protein.J. Mol. Biol.
224, 899-904.
32. Sourgens, H. and F. Lefrère. 2011. A systematic review of available clinical evidence-filgrastim compared with lenograstim. Int. J. Clin. Pharmacol. Ther. 49, 510-518.
33. Sörgel, F., H. Lerch, and T. Lauber. 2010. Physicochemical and biologic comparability of a biosimilar granulocyte col- ony-stimulating factor with its reference product.BioDrugs 24, 347-357.
34. Souza, L., T. Boone, J. Gabrilove, P. Lai, K. Zsebo, D.
Murdock, V. Chazin, J. Bruszewski, H. Lu, K. Chen, J.
Barendt, E. Platzer, M. Moore, R. Mertelsmann, and K.
Welte. 1986. Recombinant human granulocyte colony-stim- ulating factor: effects on normal and leukemic myeloid cells.
Science232, 61-65.
35. Wadhwa, M., C. Bird, M. Hamill, A. Heath, P. Matejtschuk, and R. Thorpe. 2011. The 2nd International Standard for hu- man granulocyte colony stimulating factor. J. Immunol.
Methods 367, 63-69.
36. Walter, M., W. Cook, B. Zhao, R. Jr. Cameron, S. Ealick.
R. Jr. Walter, P. Reichert, T. Nagabhushan, P. Trotta, and C. Bugg. 1992. Crystal structure of recombinant human in- terleukin-4. J. Biol. Chem.267, 20371-20376.
37. Zink, T., A. Ross, K. Lüers, C. Cieslar, R. Rudolph, and T.
Holak. 1994. Structure and dynamics of the human gran- ulocyte colony-stimulating factor determined by NMR spectroscopy. Loop mobility in a four-helix-bundle protein.
Biochemistry 33, 8453-8463.
38. Zsebo, K., A. Cohen, D. Murdock, T. Boone, H. Inoue, V.
Chazin, D. Hines, and L. Souza. 1986. Recombinant human granulocyte colony stimulating factor: molecular and bio- logical characterization. Immunobiology172, 175-184.
박정혜1․박정애1․강석우2․구태원2․정경태1*
(1동의대학교 임상병리학과, 2국립농업과학원 농업생물부)
혈액세포의 분화와 성장은 20 여종 이상의 성장인자에 의해 조절된다. 혈액세포 생산에 관여하는 인자를 조혈 성장인자(hematopoitic growth factor)라고 한다. 조혈성장인자를 임상적으로 사용하기 위해 원핵생물 또는 진핵 생물 생산 시스템에서 재조합 단백질로 생산되고 있다. 그 중에서 Glranulocyte-Colony Stimulating Factor (G-CSF)는 호중구 세포 수가 감소된 암환자와 선천성 질병을 가진 환자에게 임상적 치료제로 아주 중요한 역할을 한다. 이 환자들은 충분하지 못한 호중구 세포로 말미암아 감염에 대한 위험이 아주 높으며 치사율 또한 높다.
두 종류의 재조합 G-CSF가 항암치료 후 발생하는 부작용으로 나타나는 호중구 세포 감소증 치료에 사용되고 있 다. G-CSF의 중요성에 맞추어 G-CSF의 물리적 및 생물학적 기능에 대한 특성을 설명하였으며, 또한 항암치료와 G-CSF의 임상적 사용에 대한 연관성을 토론하였다. 마지막으로 두 종류의 재조합 G-CSF인 non-glycosylated G-CSF, filgrastim과 glycosylated G-CSF를 비교 설명하였으며, 이들 기존의 G-CSF에 비교되는 바이오시밀러에 대한 전망을 제시하였다.