47
악성림프구증식질환에서 CD34양성 세포채집의 예측인자
1인제대학교 의과대학 부산백병원 내과학교실, 2진단검사의학과교실,
3울산대학교 의과대학 울산대학교병원 내과학교실
이상민
1ㆍ권민정
1ㆍ강명주
1ㆍ이은주
1ㆍ이원식
1ㆍ손창학
1이자영
2ㆍ이정녀
2ㆍ김 혁
3ㆍ주영돈
1
Factors to Predict Autologous CD34 Positive Cells Harvest in the Patients with Malignant Lymphoproliferative Disorder
Sang Min Lee, M.D.1, Min-Jeong Kwon, M.D.1, Myung Joo Kang, M.D.1, Eun Joo Lee, M.D.1, Won Sik Lee, M.D.1, Chang Hak Sohn, M.D.1, Ja Young Lee, M.D.2,
Jeong Nyeo Lee, M.D.2, Hawk Kim, M.D.3 and Young Don Joo, M.D.1
1Department of Internal Medicine and 2Labatory Medicine, Busan Paik Hospital, Inje University College of Medicine, Busan,
3Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea
Background: Autologous peripheral blood stem cell transplantation (PBSCT) has been used as a major treatment strateg for malignant lymphoproliferative disorder. The number of CD34 positive cells in the harvested product is a very important factor for achieving successful transplantation. We studied the fac- tors that can predict the number of CD34 positive cells in the harvested product of multiple myeloma (MM) and Non-Hodgkin’s lymphoma (NHL) patients after mobilizing them with chemotherapy plus G-CSF.
Methods: A total of 69 patients (MM 25 patients, NHL 44 patients) with malignant lymphoproliferative disorder had been mobilizedwith chemotherapy and granulocyte colony-stimulating growth factor from January, 2003 to July, 2008. We analyzed the clinical characteristics, the peripheral blood (PB) parameters and the number of CD34 positve cells in the PB and their correlation with the yield of PBPCs collected from the mobilized patients.
Results: The total number of leukapheresis sessions was 134 (mean: 1.94 session per patient), and the mean number of harvested CD34 positive cell per patient was 12.47×106/kg. The number of harvested CD34 positive cells was correlated with the patient’s height, the number of peripheral blood hematopoietic progenitor cells (HPC) and the number of PB CD34 positive cells at the harvest (P<0.05). But the num- ber of PB CD34 positive cell was the only significant factor for the quantity of harvested CD34 positive cells on the linear regression analysis (P<0.05). More than 23.7/μL PB CD34 positive cells were needed to harvest 3×106/kg CD34 positive cells, according to the ROC curve (P<0.05).
Conclusion: The number of PB CD34 positive cells (≥23.7/μL) at the harvest might be the predictor of harvesting more than 3×106/kg CD34 positive cell for autologous PBSCT in patients with malignant lymphoproliferative disorder. (Korean J Hematol 2009;44:47-52.)
Key Words: CD34 positive cell, Mobilization, Harvest
접수:2008년 12월 4일, 수정:2009년 1월 22일 승인:2009년 1월 30일
교신저자:주영돈, 부산시 부산진구 개금동
614-735, 인제대학교 의과대학 부산백병원 내 과(혈액종양내과)
Tel: 051-890-6270, Fax: 051-895-6977 E-mail: [email protected]
본 논문은 2004년도 인제대학교 학술연구조성비 보조에 의 한 것임.
Correspondence to:Young Don Joo, M.D.
Department of Internal Medicine, Busan Paik Hospital, Inje University College of Medicine
Gaegum-dong, Busangin-gu, Busan 614-735, Korea Tel: +82-51-890-6270, Fax: +82-51-895-6977 E-mail: [email protected]
Table 1. The characteristics of all patients (n=69)
Agz (yrs, mean) 50.44 (15∼70)
Gender
Male 36
Femal e33
M:F ratio 1:0.91
Body weight (kg) (mean) 61.14 (44∼88)
Height (cm) (mean) 163.13 (143∼186)
Disease (%)
Non-Hodgkin’s lymphoma 44 (63.8)
Multiple myeloma 25 (36.2)
Chemotherapies before mobilization (mean)
Non-Hodgkin’s lymphoma 6.39 (1∼11)
Multiple myeloma 4.62 (1∼12)
Interval from diagnosis
to mobilization (days, mean) 349.7 (38∼1834) 서 론
고용량 항암화학요법 및 자가조혈모세포이식은 다 양한 악성 혈액질환의 치료에 사용되고 있다.1,2) 1979 년 이전까지는 고용량 항암화학요법에 따른 골수기능 억제를 회복시키기 위한 수단으로 자가골수이식을 사 용하였다.3) 1980년대 이후 백혈구분반술(leukaphere- sis)로 말초혈액내 조혈모세포를 채집할 수 있게 되었 다. 골수채집과 달리 전신마취나 반복천자에 따른 어 려움이 없으며 말초조혈모세포 채집은 이식 후 빠른 생착을 나타내었다. 이 때문에 말초혈액 조혈모세포이 식은 골수이식을 대체할 수 있는 방법으로 인식되었
다.4,5) 그리고 자가 말초혈액 조혈모세포이식은 이식편
대숙주반응이 없고, 이식 후 과립구와 혈소판의 회복 이 빨라서 시행 건수가 증가하는 추세에 있다.6,7) 성공적인 자가말초혈액 조혈모세포이식을 위해서는 충분한 수의 CD34양성 세포를 채집하는 것이 필수적 인 요소이다. 정상적인 혈액내 CD34양성 세포수는 매 우 적지만, 항암요법 후 과립구 집락촉진인자(granulo- cyte colony-stimulating factor, G-CSF)를 투여하는 가 동화 요법을 시행하면 CD34양성 세포를 골수에서 말 초혈액으로 이동시켜서 말초혈액 내 CD34양성 세포수 를 증가시킬 수 있다.8)
악성림프구증식질환에서 가동화 요법은 다양한 항 암제를 투여한 후 CD34양성 세포를 채집하기 전까지 과립구 집락촉진인자를 일정기간 사용하는데 CD34양 성 세포의 채집에 필요한 과립구 집락촉진인자의 사용 기간이 정해져 있지 않고 채집 가능한 시점에 대한 기 준이 명확하지 않다. 이에 저자는 자가 조혈모세포이 식이 필요한 악성림프종과 다발성골수종을 가진 악성 림프구증식질환 환자들을 대상으로 가동화요법 후 백 혈구분반술의 회수, 채집 시 말초혈액 내 혈구수 등의 요소들을 채집된 CD34양성 세포수와 비교 분석하여 상관관계 및 통계적 유의성을 조사하였다.
대상 및 방법
1. 대상
2003년 1월부터 2008년 7월까지 악성림프종 또는 다발성골수종으로 고용량항암화학요법 및 자가 말초 혈액 조혈모세포이식을 시행받은 총 69명을 대상으로 자가조혈모세포 채집 결과를 후향적으로 분석하였다 (Table 1).
대상환자 선정조건은 항암제 감수성을 보이는 고위 험 또는 재발성 악성림프종과 진행된 다발성골수종 환 자로 15세부터 70세까지, 기대생존기간 3개월 이상, 활 력징후 Eastern Cooperative Oncology Group (ECOG) 0
∼2, 혈청 크레아티닌 1.5mg/dL이하, 말초혈액 백혈구 수 4,000/μL이상, 혈소판수 100,000/μL이상, 혈청 AST/ALT가 정상값의 2배이하, 진행된 심부전이나 호 흡부전이 없는 환자로 하였다.
2. 방법
1) 가동화요법
가동화를 위한 항암화학요법시행 후, 말초혈액 내 백혈구수가 1,000/μL이하로 감소하면 과립구 집락촉 진인자(G-CSF) 10μg/kg/day을 매일 투여하고 말초혈 액내 백혈구수가 1,000/μL이상 상승하면 절대호중구 수, 미성숙세포를 분석하는 Immature Myeloid Information (IMI) channel을 이용한 조혈전구세포수 (hematopoietic progenitor cell, HPC)와 CD34양성 세포 수 등을 측정하고, CD34양성 세포를 백혈구성분채집 술을 이용하여 채집하였다.
2) 말초혈액 내 혈구수 측정
과립구 집락촉진인자를 투여하기 시작한 날로부터 말초혈액 내 혈구수는 혈액자동분석기 SE9000 (Sys- mex Corp, Kobe, Japan)과 LH 750 (Beckman Coulter Inc, Fullerton, CA, USA)을 사용하여 매일 1회씩 측정 되었다.
3) 말초혈액 CD34양성 세포채집
말초혈액 백혈구수가 1,000/μL이상으로 상승하는 첫날부터 성분채집기 Fenwal CS-3000 Plus (Baxter Healthcare, Deerfield, IL, USA)와 Cobe spectra (Cobe
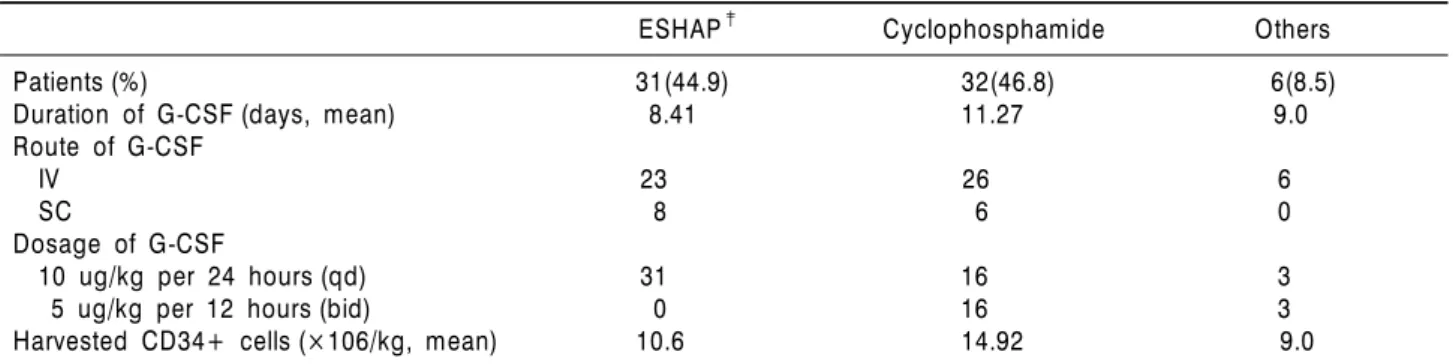
Table 2. The findings of G-CSF† between mobilization regimens for CD34+cell harvest
ESHAP‡ Cyclophosphamide Others
Patients (%) 31(44.9) 32(46.8) 6(8.5)
Duration of G-CSF (days, mean) 8.41 11.27 9.0
Route of G-CSF
IV 23 26 6
SC 8 6 0
Dosage of G-CSF
10 ug/kg per 24 hours (qd) 31 16 3
5 ug/kg per 12 hours (bid) 0 16 3
Harvested CD34+ cells (×106/kg, mean) 10.6 14.92 9.0
†: G-CSF, granulocyte-colony stimulating factor; ‡: ESHAP, etoposide, methylprednisolone, cytarabine, cisplatin
Table 3. Peripheral blood findings at the time of CD34+
cell harvest (n=69)
Blood cells Mean (range)
WBC (×103/μL) 14.78 (1.32∼75.59)
Neutrophil 10.32 (0.56∼61.23)
Lymphocyte 0.87 (0.06∼4.5)
Monocyte 1.14 (0∼4.96)
HPC†(/μL) 60.85 (4∼304)
CD34+ cell (/μL) 99.76 (61∼763.5)
†: HPC, hematopoietic progenitor cell BCT Inc. Lakexood. CO, USA)를 이용하여 대용량 말
초혈액 조혈모세포 채집술을 시행하였다. 채집술에 사 용된 두 기계글간의 collection coefficiency는 비슷하다 고 알려져 있다.9)
4) CD34양성 세포 숫자 측정
채집 시 말초혈액 내 CD34양성 세포 숫자와 채집된 CD34양성 세포 숫자는 Stem-Kit (Beckman Coulter Inc, Fullerton, CA, USA)와 BD Trucount (Becton Dic- kinson, Mountainview, CA, USA)로 형광염색한 후에 유세포분석기 EPICS XL (Beckman Coulter Inc, Fullerton, CA, USA)와 FACS Caliber (Becton Dickin- son, Mountainview, CA, USA)을 이용하여 측정하였다.
3. 통계분석방법
환자의 임상적 특성, 채집 시 말초혈액소견, 가동화 요법 및 백혈구성분채집술 등에 대한 통계분석은 SPSS (version 12K)를 이용하였고, 유의수준은 0.05이하로 하였다. 다양한 요소들의 상호관련성은 Pearson 상관 계수를 이용하여 분석하였고, 채집 완료된 CD34양성 조혈모세포수와 관련이 있는 환자 특성과 말초혈액소 견에 대해서는 선형회귀분석으로 통계학적 의미를 평 가하였다.
결 과
1. 대상환자의 특성
대상환자는 총 69명이며, 연령분포는 15세에서 70세 로써 평균 53세이고, 남녀성비는 1:0.9 (36:33)였다. 대 상질환은 악성림프종(미만성 거대 B세포 림프종)이 44예, 다발성골수종이 25예였다. 진단 후 가동화까지 소요된 시간간격은 38일에서 1,834일로 평균 349.7일 이었다. 가동화이전 항암화학요법의 평균횟수는 악성
림프종이 6회, 다발성골수종이 5.04회였다(Table 1).
2. 가동화요법
가동화요법을 위한 항암화학요법으로 Cyclophosph- amide 단독사용이 32예, Etoposide, Methylpredniso- lone, Cytarabine, Cisplatin (ESHAP) 복합사용이 31예, 기타 6예였다. 과립구 집락촉진인자로 Filgrastim 58예, Lenograstim 11예를 사용하였고, 투여경로는 정맥주사 55예, 피하주사 14예이며, 투여일은 3일에서 23일로 평 균 9.82일이었다. 투여방법은 10μ/kg/day을 하루 1회 주사(n=50)하거나 5μ/kg/day 하루 2회 주사(n=19)하 였다(Table 2).
3. 말초혈액 조혈모세포채집
전체 69명의 환자에서 총 134회의 백혈구분반술이 시행되었고, 환자당 평균 1.94회를 시행하였다. 최대량 의 채집이 이루어진 시점에서 말초혈액 내 조혈전구세 포와 CD34양성 세포를 포함한 혈구수는 Table 3과 같 다. 환자당 채집완료된 CD34양성 전체세포수의 합계 에 대한 평균은 평균 12.47×106/kg이었다(1.8∼50×
106/kg). 질병별로는 악성림프종이 13.07×106/kg (1.9
Table 5. The efficacy of CD34+cell harvest (n=61)
Correlation coefficient for CD34+cell harvest
Pearson correlation coefficient P-value
Height -0.297 0.014
HPC 0.419 0.010
PB†CD34+cell 0.266 0.038
Linear regression for CD34+harvest (R2=0.485)
Estimated coefficient (B) Standard error P-value
Height -0.197 0.129 0.141
HPC -0.010 0.026 0.698
PB CD34+cell 0.058 0.020 0.008
†: PB, peripheral blood
Table 4. The results of CD34+cell harvest (n=69) Leukapheresis Patients (%)† Mean CD34+cells
(×106/kg, range)
1st 69 (100) 7.54 (0∼27)
2nd 46 (66.67) 6.39 (0.2∼34.8)
3rd 14 (20.29) 2.87 (0.2∼14.8)
4th 3 (4.34) 0.66 (0.3∼0.9)
5th 2 (2.9) 1 (0.3∼1.7)
†: Total harvest=134, mean harvest per patient=1.94
∼36.8), 다발성골수종이 11.4×106/kg (1.8∼50)였다.
채집이 1회만 시행된 43예에서 CD34양성 세포수는 평 균 7.54×106/kg이었고, 채집회수가 증가될수록 CD34 양성 세포수의 단위 채집량은 감소하였다(Table 4).
대상환자의 특성과 말초혈액소견을 대상으로 채집 된 CD34양성 세포와의 상관관계를 분석하였다. 통계 학적 의미(P<0.05)가 있는 상관계수를 나타내는 요소 는 환자의 신장, 채집 시 말초혈액 내 조혈전구세포수 와 CD34양성 세포수였다(Table 5). 이들을 대상으로 다시 선형회귀분석을 시행하여 CD34양성 세포채집에 통계적으로 유의하게 영향을 주는 요소로서 채집 시 말초혈액 내 CD34양성 세포수이었고(P=0.008), 환자 의 신장과 채집 시 말초혈액 내 조혈전구세포수는 통 계적인 유의성이 없었다(Table 5). Receiver operating characteristics (ROC) 곡선을 이용하여 분석한 결과, 3.0×106/kg이상의 CD34양성 세포 채집을 예측하기 위한 최소한의 채혈 시 말초혈액 내 CD34양성 세포수 는 23.7/μL이었다. 이때 영역이 0.817, 민감도는 0.83, 특이도는 0.87이었다(P=0.004).
고 찰
악성림프종과 다발성골수종 환자에서 고용량 항암화 학요법과 자가조혈모세포이식은 표준항암화학요법만 을 사용한 환자군보다 향상된 치료성적을 보이고 있 다.4) 성공적인 자가조혈모세포이식을 위해서는 2∼
5×106/kg 이상의 CD34양성 세포가 필요하다.10,11) 자 가조혈모세포의 공급원으로써 생착과 골수기능 회복 에 유리한 말초혈액 조혈모세포를 골수대신 이용하는 것이 보편화되고 있다. 하지만 정상적인 말초혈액에 존재하는 CD34양성 세포수는 약 3.0/μL이므로, 충분 한 세포수를 확보하기 위해서는 골수 내 조혈모세포를 말초혈액으로 이동시키는 가동화 요법이 필요하다. 따 라서 가동화 요법 후 효과적으로 말초혈액 내 CD34양 성 세포를 채집하기 위해서는 채집방법 및 시기에 대 한 이해가 필요하다.12,13)
가동화 기전은 조혈미세환경과 세포표면부착물질의 변화 등으로 이해하고 있지만 명확하게 정립되어 있지 않다. 가동화되는 CD34양성 세포수를 증가시키기 위 해 granulocyte macrocyte-colony stimulating factor (GM-CSF),15,16) G-CSF, Interleukin-3, stem cell factor (SCF) 등의 집락촉진인자가 사용되고 있다.12,17,18) 그리 고 가동화요법에 따른 CD34양성 세포 채집량은 나이, 성별, 체중과 신장, 진단질환, 항암제 종류 및 용량, 방 사선 치료, 골수침범여부 등 여러 가지 요소에 의해 영 향을 받는다.19,20)
일반적으로 말초혈액 CD34양성 세포의 채집은 항암 제 투여 후 말초혈액 내 백혈구 또는 중성구 수치가 최저에 도달한 시점에 과립구 집락촉진인자를 투여하 여 말초혈액 내 CD34양성 세포수가 최고에 도달하였
다고 예상되는 시점에서 채집을 한다.8) 그러나 가동화 에 따른 말초혈액 내 CD34양성 세포수치는 최고점에 서 유지되는 기간이 매우 짧고, 개인간 차이가 존재한 다. 그리고 가동화를 통한 조혈모세포 채집 회수의 증 가는 종양의 오염도를 높일 수 있으므로 채집회수를 최소화하면서 목표하는 적정량의 CD34양성 세포를 채 집하기 위해서는 최적의 채집시기를 결정하여야 한다.
채집시기를 예측하기 위해 유세포분석법이 도입되기 전부터 채집 전 말초혈액 내 총백혈구수와 단핵구수 등이 이용되고 있지만, 채집된 CD34양성 세포수와 상 관관계가 낮았다.13,21) CFU-GM 배양검사는 채집된 CD34양성 세포와의 상관관계가 우수하지만, 숙련도, 장비, 2주 이상 배양시간과 검사기관에 따른 변이 등이 제한요소이다.22) 따라서 말초혈액 내 CD34양성 세포 수와 세포표면의 화학적 구성성분차이를 이용한 조혈 전구세포(hematopoietic progenitor cell, HPC)수가 새로 운 예측인자로 연구되고 있다. 채집 시 말초혈액 내 CD34양성 세포수는 채집된 CD34양성 세포수와 우수 한 상관관계를 보이지만, 숙련도, 고가의 검사비용, 2 시간 이상의 분석시간 등이 제한요소이다.23-25) 혈구자 동분석기에 탑재된 IMI (immature cell information) channel을 이용하여 가동화에 따른 미성숙 세포수를 측정하는 방법은 별도의 장비나 비용, 검사시간 등이 필요하지 않으며 이들 미성숙세포는 조혈전구세포로 대표된다.20)
본 연구에서는 나이, 성별, 신체조건, 질환, 가동화요 법 등의 특성을 분석하였고, 백혈구분반술 시행 회수 와 매번 채집된 CD34양성 세포 수를 비교하였다. 채집 완료된 CD34양성 조혈모세포수를 대상으로 채집 시 말초혈액 내 총백혈구수, 조혈전구세포수, CD34양성 세포수와의 상관관계를 통계분석하였다. 채집된 CD34 양성 조혈모세포수와 상관관계를 나타내는 요소로 신 장, 채집 시 말초혈액 내 조혈전구세포수 및 CD34양성 세포가 있었다. 이 요소들에 대한 선형회귀분석에서 채집 시 말초혈액 내 CD34양성 세포수만이 통계적 의 미를 보이고 있다(P=0.008). 그리고 성공적인 자가조 혈모세포이식에 필요한 3×106/kg 이상의 CD34양성 세포채집을 예측할 수 있는 채집시 말초혈액 내 CD34 양성 세포수는 23.7/μL 이상임을 ROC곡선으로 확인 하였다(P=0.004).
요 약
배경: 악성림프종과 다발성골수종 환자에서 고용량
항암화학요법 및 자가조혈모세포이식을 성공적으로 시행하기 위해서는 충분한 조혈모세포수가 필요하다.
방법: 총 69명을 대상으로 자가조혈모세포 채집 결 과를 후향적으로 분석하였다.
결과: 항암화학요법 및 집락촉진인자를 이용하는 가 동화요법 시 CD34양성 세포 채집시기를 예측할 수 있 는 상관관계인자로는 환자의 신장, 채집 시 말초혈액 내 조혈전구세포수 및 CD34양성 세포수 등이 있었지 만, CD34양성 세포수만이 의미가 있었다(P=0.008). 그 리고 자가조혈모세포이식에 필요한 3×106/kg 이상의 CD34양성 세포채집을 예측할 수 있는 채집 시 말초혈 액 내 CD34양성 세포수는 23.7/μL이상이었다(P=
0.004).
결론: 가동화요법 후 채집 시 말초혈액에서 23.7/μL 이상의 CD34양성 세포수의 측정은 채집시기 예측에 도움이 될 것으로 판단되었으며, 조혈전구세포 유용성 에 대해서는 앞으로 추가적인 연구가 필요한 것으로 판단되었다.
참 고 문 헌
1) Shipp MA, Abeloff MD, Antman KH, et al. Interna- tional Consensus Conference On High-Dose Therapy With Hematopoietic Stem Cell Transplantation In Aggressive non-Hodgkin's lymphomas, report of the jury. J Clin Oncol 1999;17:423-9.
2) Attal M, Harousseau JL, Stoppa AM, et al. A pro- spective, randomized trial of autologous bone mar- row transplantation and chemotherapy in multiple myeloma. Intergroupe Francais du Myélome. N Engl J Med 1996;335:91-7.
3) Goldman JM. Autografting cryopreserved buffy coat cells for chronic granulocytic leukaemia in transfor- mation. Exp Hematol 1979;7(5 Suppl):389-97.
4) Schwartzberg L, Birch R, Blanco R, et al. Rapid and sustained hematopoietic reconstitution by peripheral blood stem cell infusion alone following high-dose chemotherapy. Bone Marrow Transplant 1993;11:
369-74.
5) Russell NH, Hunter A, Rogers S, Hanley J, Anderson D. Peripheral blood stem cells as an alternative to marrow for allogeneic transplantation. Lancet 1993;
341:1482.
6) Rowley SD. Processing of hematopoietic stem cell components for transplantation: variations in cur- rent practice. Transfusion 1998;38:1-4.
7) Kessinger A, Armitage JO, Landmark JD, Smith DM,
Weisenburger DD. Autologous peripheral hemato- poietic stem cell transplantation restores hemato- poietic function following marrow ablative therapy.
Blood 1988;71:723-7.
8) Dicke KA, Hood D, Hanks S. Peripheral blood stem cell collection after mobilization with intensive che- motherapy and growth factors. J Hematother 1994;3:
141-4.
9) Yang SM, Liu KY, Lu DP. Comparison of the effect of Cobe Spectra and Fenwal CS 3000 plus blood cell separators in collection of peripheral blood stem cell components. Zhongquo Shi Yan Xue Ye Xue Za Zhi 2005;13:245-9.
10) Demirer T, Buckner CD, Bensinger WI. Optimiza- tion of peripheral blood stem cell mobilization. Stem Cells 1996;14:106-16.
11) Bender JG, To LB, Williams S, Schwartzberg LS.
Defining a therapeutic dose of peripheral blood stem cells. J Hematother 1992;1:329-41.
12) Sutherland HJ, Eaves CJ, Lansdorp PM, Phillips GL, Hogge DE. Kinetics of committed and primitive blood progenitor mobilization after chemotherapy and growth factor treatment and their use in auto- transplants. Blood 1994;83:3808-14.
13) Keung YK, Cobos E, Dunn D, et al. Determining fac- tors for the outcome of peripheral blood progenitor cells harvests. J Clin Apher 1996;11:23-6.
14) Pérez-Simón JA, Caballero MD, Corral M, et al. Min- imal number of circulating CD34+ cells to ensure successful leukapheresis and engraftment in autolo- gous peripheral blood progenitor cell transplanta- tion. Transfusion 1998;38:385-91.
15) Socinski MA, Cannistra SA, Elias A, Antman KH, S- chnipper L, Griffin JD. Granulocyte-macrophage col- ony stimulating factor expands the circulating hae- mopoietic progenitor cell compartment in man.
Lancet 1988;1:1194-8.
16) Haas R, Hohaus S, Egerer G, Ehrhardt R, Witt B, Hunstein W. Recombinant human granulocyte-m- acrophage colony-stimulating factor (rhGM-CSF) s- ubsequent to chemotherapy improves collection of blood stem cells for autografting in patients not eligi- ble for bone marrow harvest. Bone Marrow Trans- plant 1992;9:459-65.
17) Brugger W, Bross K, Frisch J, et al. Mobilization of peripheral blood progenitor cells by sequential ad- ministration of interleukin-3 and granulocyte-macro- phage colony-stimulating factor following poly- chemotherapy with etoposide, ifosfamide, and cis- platin. Blood 1992;79:1193-200.
18) Teshima T, Harada M, Takamatsu Y, et al. Granulo- cyte colony-stimulating factor (G-CSF)-induced mobi- lization of circulating haemopoietic stem cells. Br J Haematol 1993;84:570-3.
19) Haas R, Mohle R, Frühauf S, et al. Patient character- istics associated with successful mobilizing and auto- grafting of peripheral blood progenitor cells in ma- lignant lymphoma. Blood 1994;83:3787-94.
20) Kotasek D, Shepherd KM, Sage RE, et al. Factors af- fecting blood stem cell collections following high-dose cyclophosphamide mobilization in lymphoma, myelo- ma and solid tumors. Bone Marrow Transplant 1992;9:11-7.
21) Schwella N, Siegert W, Beyer J, et al. Autografting with blood progenitor cells: predictive value of pre- apheresis blood cell counts on progenitor cell harvest and correlation of the reinfused cell dose with hema- topoietic reconstitution. Ann Hematol 1995;71:227- 34.
22) Hillyer CD, Tiegerman KO, Berkman EM. Increase in circulating colony-forming units-granulocyte-ma- crophage during large-volume leukapheresis: evalua- tion of a new cell separator. Transfusion 1991;31:32 7-32.
23) Mohle R, Murea S, Pförsich M, Witt B, Haas R.
Estimation of the progenitor cell yield in a leukaphe- resis product by previous measurement of CD34+
cells in the peripheral blood. Vox Sang 1996;71:90- 6.
24) Remes K, Matinlauri I, Grenman S, et al. Daily meas- urements of blood CD34+ cells after stem cell mobi- lization predict stem cell yield and posttransplant hematopoietic recovery. J Hematother 1997;6:13-9.
25) Schots R, Van Riet I, Damiaens S, et al. The absolute number of circulating CD34+ cells predicts the num- ber of hematopoietic stem cells that can be collected by apheresis. Bone Marrow Transplant 1996;17:509- 15.