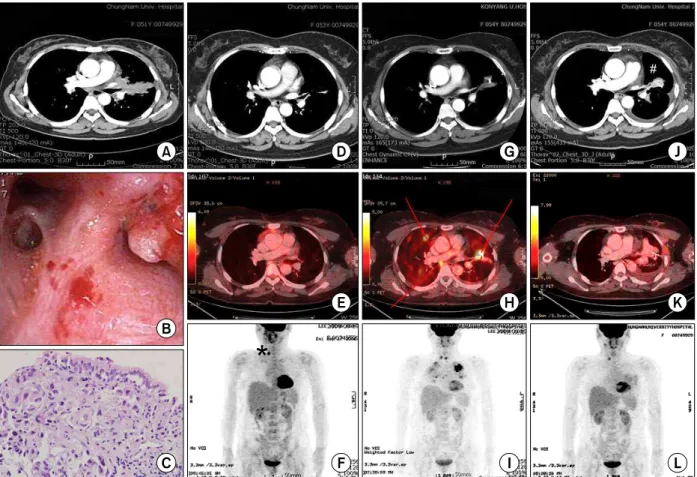
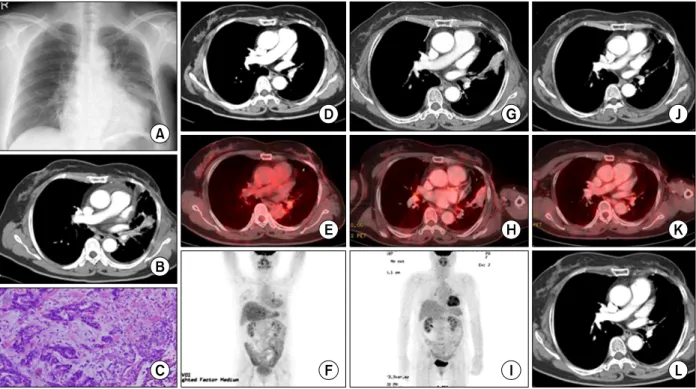
Second Complete Remission of Relapsed Stage IV Non-Small Cell Lung Cancer Following Retreatment
5
0
0
전체 글
(2)
(3)
(4)
(5)
수치
관련 문서
Purpose: Our institution has implemented two different adjuvant protocols in treating patients with non-small cell lung cancer (NSCLC): chemotherapy followed
During follow-up, three patients (one patient with pathologic stage IIB NSCLC and two patients with pathologic stage IIIA NSCLC) experienced recurrence and died as a result of
Surgical resection is the most effective treatment for early-stage non-small cell lung cancer (NSCLC), and lobectomy is the standard surgical technique for
Background: The purposes of this study were to evaluate the appropriateness of the stage migration of stage IIA non-small cell lung cancer (NSCLC) in the
Forest plot showing a comparison of recurrence-free survival between segmentectomy and lobectomy in (A) stage I and (B) stage IA non-small cell lung cancer. All of them used
Objective: We aimed to compare the prognoses of patients with pathologically true negative (P-TN) N2 and PET/CT false negative (FN) results in stage T1 non- small cell lung
Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small cell lung cancer previously treated with chemotherapy.. Shepherd FA,
The results of this study showed that FXIII activity was higher in patients with NSCLC than in the healthy group. Patients with squamous cell carcinoma and stage III and IV
