A Case of Statin-Induced Interstitial Pneumonitis due to Rosuvastatin
Se Yong Kim, M.D.
1, Se Jin Kim, M.D.
1, Doran Yoon, M.D.
2, Seung Wook Hong, M.D.
2, Sehhoon Park, M.D.
2and Chan-Young Ock, M.D.
21
Department of Internal Medicine, The Armed Forces Medical Hospital, Seongnam,
2Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
Statins lower the hyperlipidemia and reduce the incidence of cardiovascular events and related mortality. A 60-year-old man who was diagnosed with a transient ischemic attack was started on acetyl-L-carnitine, cilostazol, and rosuvastatin.
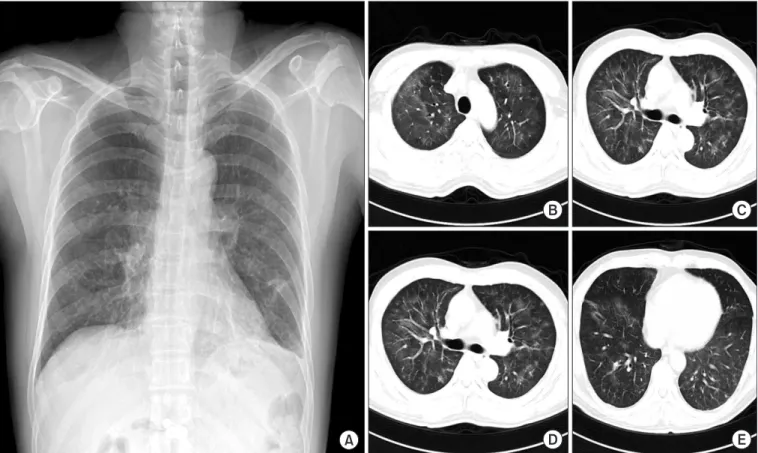
After rosuvastatin treatment for 4 weeks, the patient presented with sudden onset fever, cough, and dyspnea. His symptoms were aggravated despite empirical antibiotic treatment. All infectious pathogens were excluded based on results of culture and polymerase chain reaction of the bronchoscopic wash specimens. Chest radiography showed diffuse ground-glass opacities in both lungs, along with several subpleural ground-glass opacity nodules; and a foamy alveolar macrophage appearance was confirmed on bronchoalveolar lavage. We suspected rosuvastatin-induced lung injury, discontinued rosuvastatin and initiated prednisolone 1 mg/kg tapered over 2weeks. After initiating steroid therapy, his symptoms and radiologic findings significantly improved. We suggest that clinicians should be aware of the potential for rosuvastatin-induced lung injury.
Keywords: Rosuvastatin; Lung Diseases, Interstitial; Chemically-Induced Disorders
rosuvastatin, and pitavastatin. Statins have a low frequency of side effects including hepatotoxicity, myotoxicity, and pro- teinuria
2,3. However, adverse reactions involving the respira- tory system are uncommon. Several cases of statin-induced pulmonary toxicity have been reported
4-6. Regarding statins, most cases were associated with simvastatin, fluvastatin, and atorvastatin. Interstitial lung disease secondary to rosuvastatin is rare
7,8. In addition, rosuvastatin-induced interstitial lung dis- ease has not been reported in Korea. Herein, we will present a patient who was diagnosed with drug-induced interstitial lung disease (DILD) secondary to rosuvastatin.
Case Report
A 60-year-old man who never smoker was a professor of humanities and had no experiences of exposure to noxious materials. He has not traveled or moved anywhere in recent years. He had been diagnosed with acute hypersensitivity pneumonitis 18 months previously and was treated with a steroid therapy for 6 weeks. Cause of hypersensitivity pneu- monitis had been confirmed as being fungus derived from Copyright © 2015
The Korean Academy of Tuberculosis and Respiratory Diseases.
All rights reserved.
Introduction
Statins, hydroxymethylglutaryl CoA reductase inhibitors, are known to lower the plasma low-density lipoprotein (LDL) cholesterol level and reduce the incidence of cardiovascular events and mortality
1,2. Currently available statins include lovastatin, pravastatin, simvastatin, fluvastatin, atorvastatin,
Address for correspondence: Se Jin Kim, M.D.
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, The Armed Forces Medical Hospital, 81 Saemaeul-ro 177 beon-gil, Bundang-gu, Seongnam 463-040, Korea
Phone: 82-31-725-6037, Fax: 82-31-706-0987 E-mail: [email protected]
Received: Jan. 28, 2015 Revised: Mar. 17, 2015 Accepted: Mar. 26, 2015
cc