Imatinib-Mesylate Induced Interstitial Pneumonitis in Two CML Patients
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치
관련 문서
A chest computed tomography (CT) of the patient did not show any shadow suspected of malignancy, but adenocarcinoma was found on a transbronchial lung biopsy and on a
We report a case of interstitial pneumonitis in a patient with disseminated extranodal marginal zone B cell lymphoma after the 5th cycle of rituximab and CHOP..
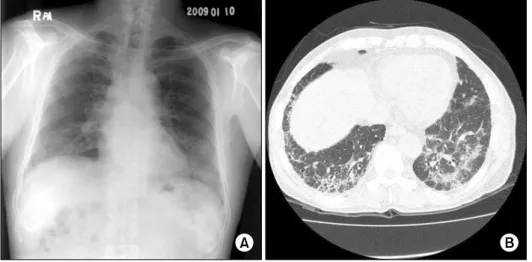
(B) A chest computed tomog- raphy obtained on the day of admission demonstrates multifocal diffuse, patchy ground glass opacity and interlobular septal thickening in both
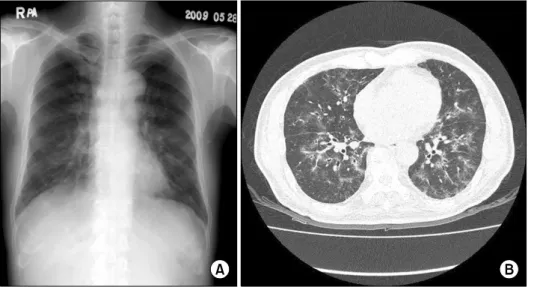
A chest computed tomography scan with a lung window set- ting shows multiple ill-defined ground glass opacities and multiple nodules with ground glass opacity (arrowheads) in the
