192
Functional Polymorphism in the Promoter Region of Matrix Metalloproteinase-9 is Strongly Associated with Acute Myocardial Infarction
Pum Joon Kim, M.D.1, Kiyuk Chang, M.D.2, Yoon Seok Koh, M.D.1, Ki Bae Seung, M.D.1, Sang Hong Baek, M.D.1, Woo Seung Shin, M.D.2, Sang Hyun Lim, M.D.1,
Jae Hyung Kim, M.D.1, Soon Jo Hong, M.D.1 and Kyu Bo Choi, M.D.1
1Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, 2Uijeongbu St. Mary’s Hospital, Uijieongbu,Korea
ABSTRACT
Background and Objectives:Matrix metalloproteinase-9 (MMP-9) plays an important role in the genesis of atherosclerotic plaque rupture and acute coronary syndrome (ACS), including an acute myocardial infarction (AMI). A single nucleotide polymorphism (SNP) in the MMP-9 promoter (-1562C>T) has recently been identified. This study investigated whether the SNP of the MMP-9 promoter is a significant risk factor for an AMI due to plaque rupture and if SNPs affect the transcription of the gene that elevates the MMP-9 expression level. Subjects and Methods:A polymerase chain reaction, followed by a restriction fragment length poly- morphism analysis, was performed in 173 control participants and 206 AMI patients. The serum levels of MMP-9 in the groups with or without the SNP were measured, using ELISA, and compared. Results:There was a significantly higher incidence of the -1562C>T MMP-9 polymorphism in the AMI compared to the control group (27.6% vs. 17.9%, p=0.04). A multiple logistic regression analysis of the risk factors for coronary artery disease and the MMP-9 polymorphism showed the MMP-9 polymorphism to be an important factor in the prediction of an AMI (odds ratio 1.67, 95% confidence interval 1.02-2.67, p=0.04). Conclusion: The -1562C>T polymorphism in the MMP-9 promoter is a definite risk factor for an AMI, and is associated with elevated MMP-9 expression. These results suggest that a SNP in the MMP-9 promoter is strongly associated with an Acute Myocardial Infarction.
(Korean Circulation J 2005;35:192-196)
KEY WORDS:Matrix metalloproteinase-9;Polymorphism;Acute myocardial infarction.
Introduction
The rupture of an atherosclerotic plaque is a major event in the pathogenesis of an acute myocardial infarction(AMI).1)2) Plaques that are vulnerable to rupture tend to have a large lipid-rich atheromatous core, a thin fibrous cap covering the core, active inflammatory cellular infiltration, particularly in the plaque shoulders effected by strong shear stress, and a reduced smooth muscle cell density collagen content in the fibrous cap.3-6) Matrix metalloproteinases(MMPs), mainly produced by infiltrating inflammatory cells, degrade the ext- racellular matrix, thereby contributing to the weakening of
the cap and its subsequent rupture.7) Of the many MMPs, MMP-9(gelatinase B) might play an important role in matrix degradation and the subsequent rupture of the atherosclerotic plaques, owing to its broad substrate specificity and distal position in the matrix proteolytic cascade.8) MMP-9 is in- volved in the degradation of a broad spectrum of substrates, including collagen types IV, V, VII and X as well as gela- tin,9)10) and also degrades the proteoglycans and elastins, which are resistant to degradation by other MMPs, such as stro- melysin and interstitial collagenase.9)10) In contrast to the constitutive expression of MMP-2 in the non-atherosclerotic arteries, an analysis of human coronary atherectomy speci- mens revealed the uniformly active synthesis of MMP-9 in lesions from patients with unstable angina, but not in those with stable angina.8)11) Recently, a functional single nucleo- tide polymorphism in the MMP-9 promoter, with a cytosine to thymidine transition at position -1562, was found.12) Accor- ding to in vitro assays of the promoter activity, the T allele
Received:November 25, 2004 Revision Received:January 28, 2005 Accepted:February 4, 2005
Correspondence:Kiyuk Chang, M.D.,Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Uijeongbu St.
Mary’s Hospital, 65-1, Keumo-dong, Uijieongbu 480-130, Korea Tel:82-31-820-3203, Fax:82-31-821-4471
E-mail:[email protected]
had a higher promoter activity than the C allele, and was associated with an elevation in both the levels of MMP-9 expression level and serum MMP-9 in humans.12)13) However, an association of a SNP in the MMP-9 promoter with an AMI has not been reported in Korea, even though an asso- ciation of a SNP in the MMP-9 promoter with coronary artery disease and coronary artery complicated lesions have been reported.12)14) Therefore, the aim of this study was to determine if the MMP-9 -1562C>T polymorphism is a significant risk factor in patients with AMI.
Subjects and Methods
Study population
This study included 206 AMI patients(mean age 61 years, male 60.7%) and 173 control participants, with a mean age 58 years, but all were less than 70 years old; 65.3% were males. The cases consisted of first-event AMI patients admitted to the 3 participating hospitals(Kangnam St Mary’s Hospi- tal, Uijongbu St. Mary’s Hospital, and Bucheon Holy Family Hospital, all in South Korea) between January 2003 and Au- gust 2004. The diagnoses of AMI were established according to the World Health Organization criteria and Consensus Do- cument of the Joint European Society of Cardiology/Ame- rican College of Cardiology Committee for the Redefinition of a Myocardial infarction.15) This study focused on the athe- rothrombotic coronary plaques resulting from a plaque rupture.
Accordingly, all cases had elevated cardiac troponin levels and complex lesion morphology on coronary angiography, which included ulcerating plaques and intraluminal filling defects or occlusive thrombi. This study excluded those patients with normal looking coronary angiograms or previous coronary revascularization. The healthy control subjects were enrolled from those visiting one of the Health Checkup Centers of the above three participating hospitals for their regular checkup.
The control subjects had normal electrocardiogram results and no history of myocardial infarction, angina pectoris, stroke and peripheral vascular disease. The patients and control parti- cipants originated from the same geographical area, and had similar socio-economic backgrounds and ethnicities. When the clinical characteristics were considered, hypertension was defined as a systolic pressure >140 mmHg or a diastolic pressure >90 mmHg, and diabetes mellitus a fasting blood sugar level of 126 mg/dL on two or more occasions. All individuals with diabetes mellitus were type 2. The written, informed consent was obtained from all the patients and
control participants prior to commencement of the study.
Genotyping of the MMP-9 gene
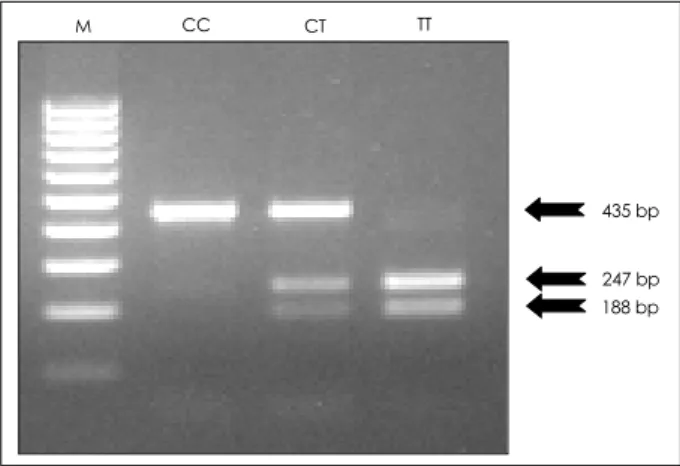
The genomic DNA was extracted from the mononuclear cells of each participant, and the specific genotypes of the MMP-9 promoter identified using a polymerase chain reac- tion followed by restriction fragment length polymorphism analysis(PCR-RFLP). For an analysis of the -1562C>T polymorphism in the MMP-9 promoter, PCR was performed using primer pairs designed to amplify the sequence from 1809 to 1374 in the promoter region. The sequences of the sense and antisense oligonucleotide primers were 5’-GCCT- GGCACATAGTAGGCCC-3’ and 5’-CTTCCTAGCCAGC- CGGCATC-3’, respectively. The resulting 435 bp amplifi- cation product was incubated with the restriction enzyme, SphI. This resulted in three potential fragments(435, 247 and 188 bp in size), which were separated on a 1.5% agarose gel and visualized using ethidium bromide. The CC homozygotes produced a single undigested band at 435 bp, whereas the CT heterozygotes showed the three bands: 435, 247 and 188 bp(Fig. 1).
Assays of serum MMP-9
The peripheral blood was drawn from all AMI patients within 24hrs of admission, and stored at -80C. A standard sandwich enzyme immunoassay was performed to measure the serum MMP-9 concentrations, using commercially availa- ble kits with a monoclonal antibody against MMP-9 accor- ding to the manufacturer’s instructions(R & D systems, MN, USA), but only on those patients with an AMI to determine the serum MMP-9 levels, according to the genotypes, at the time of plaque rupture.
Fig. 1. The three different fragments of the MMP-9 promoter. M:
methionine, CC: cytocine cytocine, CT: cytocine thymin, TT: thy- min thymin
435 bp
247 bp 188 bp
M CC CT TT
Statistical analysis
All statistical analyses were conducted between the cont- rol group and patients with AMI using the PC-SAS system (SAS Institute Inc., Cary, North Carolina, USA). The statis- tical differences in the frequency of each genotype between the groups were examined using a univariate analysis. The serum levels of MMP-9 in the AMI patients, both with and without the SNP in the MMP-9 promoter(that is, TT+CT) were compared. All the continuous variables were analyzed using paired t-tests and all the categorical variables using χ2- tests. In order to identify the independent risk factors for an AMI, a multiple logistic regression analysis, with a forward stepwise selection(Wald), was also performed. The inde- pendent variables included in the model were a SNP in the MMP-9 promoter, age, gender, body mass index, hypercholes- terolemia, and the presence of hypertension, diabetes mellitus and smoking. P<0.05 were considered significant.
Results
Characteristics of the study participants
Table 1 shows the characteristics of the AMI patients and control subjects. Among the coronary artery risk factors, age and LDL cholesterol level were the only statistically dif- ferent factors between the AMI patients and control subjects.
MMP-9 1562C>T polymorphism and AMI
The genotype frequency of the -1562C>T polymorphism in the 206 AMI patients and 173 controls was compared (Table 2). The prevalence of the genotype in each group agreed with those predicted by the Hardy-Weinberg equili- brium. While there were no TT homozygotes in the control group, four appeared in the AMI group. The frequencies of the T allele in the MMP-9 promoter were 14.3 and 8.9% in the AMI and control groups, respectively(p=0.0001). The
frequencies of the TT and CT genotype in the MMP-9 pro- moter were 26.7 and 17.9% in the AMI and control groups, respectively(p=0.0001).
Association between the MMP-9 polymorphisms and the serum level of MMP-9 in AMI patients
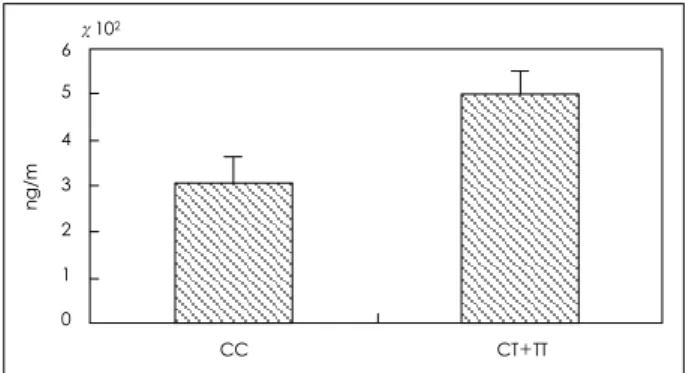
Figure 2 shows a higher plasma MMP-9 level in the group with the -1562C>T polymorphism in the MMP-9 promoter (494.8 ng/mL) than in the group without(309.5 ng/mL, p=0.04).
A multiple logistic regression analysis, with the known co- ronary artery disease risk factors and MMP-9 polymorphism, was performed. In order to determine the predictive risk fa- ctors for an AMI, a multiple logistic regression analysis, with the forward stepwise selection, using all the clinical risk factors and the MMP-9 genotypes, was performed. The most predictive risk factor for an AMI was age(odds ratio 1.80, 95% confidence interval 1.20-2.72, p=0.004), followed by
Table 2. Distribution of MMP-9 genotypes
Allele Control group AMI group p
T 031 (08.9%) 059 (14.3%)
C 315 (91.1%) 353 (85.7%) 0.0001 Genotypes
CT+TT vs. CC
CC 142 (82.1%) 151 (73.3%)
CT+TT 031 (17.9%) 055 (26.7%) 0.0001 AMI: acute myocardial infarction, T: thymin, C: cytocine, CT: cy- tocine thymin, TT: thymin thymin, CC: cytocine cytocine
Table 3. Multiple logistic regression analysis with known coronary artery risk factors and MMP-9 polymorphism (forward stepwise selection)
Variables OR 95% CI* p
Age 1.80 1.20-2.72 0.004
MMP-9 polymorphism 1.67 1.02-2.67 0.04
*: 95% confidence interval. OR: odds ratio Table 1. Characteristics of the studied subjects
Variables Control group (n=173) AMI group (n=206) Age (yrs)* 58.3±11.8 61.1±11.8
Male (%) 65.3 60.7 BMI (kg/m2) 28.3±2.90 23.9±3.40
LDL-C (mg/dL)† 120.4±37.30 129.1±35.10
Hypertension (%) 39.9 44.7
DM (%) 15.6 18.0
Smoking (%) 39.9 40.8
Values are expressed as the mean±standard deviation. AMI indicates acute myocardial infarction. BMI: body mass index, LDL-C: low density lipoprotein-cholesterol, DM: diabetes mellitus.
*: p=0.01, †: p=0.04
Fig. 2. Serum MMP-9 level according to the MMP-9 genotypes.
Serum MMP-9 level of the CC genotype: 304.5±2.19 ng/mL.
Serum MMP-9 level of the CT & TT genotypes: 494.8±3.66 ng/mL.
CC: cytocine cytocine, CT: cytocine thymin, TT: thymin thymin
ng/m
6 5 4 3 2 1 0
χ102
CC CT+TT
the SNP in the MMP-9 promoter(odds ratio 1.67, 95% con- fidence interval 1.02-2.67, p=0.04)(Table 3).
Discussion
This study showed that the -1562C>T polymorphism in the promoter region of the MMP-9 gene has a significant and independent role in the development of an acute myocardial infarction in association with increased serum MMP-9 levels in the Korean population. We found that the T allele in the MMP-9 promoter was significantly more frequent in AMI patients than in control subjects, suggesting that patients with the T allele have rupture-prone atherosclerotic plaques in their coronary arteries. Studies of human atherosclerotic specimens have demonstrated that MMP-9 can contribute to remodeling of the coronary artery plaques due to degradation of the ex- tracellular matrix, which contributes to the progression of plaques via a series of events; namely plaque rupture, micro- thrombus formation and then healing, which eventually re- sults in severe coronary artery disease.8)12)16-18)20)21) Several polymorphisms have been reported to be associated with an AMI in Koreans, including the eNOS gene polymorphism.19) However, the present study provides the first evidence of the association between a polymorphism in the MMPs and an AMI in the Korean population
MMP-9 could contribute to the development of an acute myocardial infarction by degrading a broad range of mat- rices and also some substrates resistant to degradation by other MMPs.8-10) An analysis of human coronary atherectomy specimens showed an increased MMP-9 expression in the atheromas of patients with acute coronary syndrome, but weak or absent expressions in the lesions of those with stable angina.8) Clinical studies have also shown that the serum level of MMP-9 was acutely elevated at the time of acute coronary syndrome compared with those in normal controls and pa- tients with stable angina.20)21)
Recently, Zhang et al12) reported a novel polymorphism (-1562C>T) in the promoter region of the MMP-9. The promoter region contains the 9-bp sequence(GCGCAC/TG- CC), an important regulatory element of gene expression, which appears to be a binding site for a transcription repres- sor pro-tein. The DNA-protein interaction is lost due to a C to T substitution at the polymorphism site, resulting in a T- allelic promoter, with higher promoter activity, and an in- creased level of MMP-9 synthesis. An autopsy study of the coronary arteries showed that subjects carrying this T allele
had larger complicated lesion areas than those with the CC genotype,14) suggesting the MMP-9 -1562C>T polymor- phism contributes to the development of a plaque rupture by influencing the endogenous MMP-9 production. Indeed, in this study the serum level of MMP-9 was higher in the AMI patients with the MMP-9 polymorphism than in those without.
In contrast with our results, Wang et al22) failed to show any relationship between a MMP-9 polymorphism and acute co- ronary syndrome in Caucasians. This discrepancy might have arisen from differences between the patients included in the two studies. Their study included patients with a myocardial infarction as well as those with unstable angina, which is a heterogeneous disorder from angina due to plaque rupture to that with a secondary precipitating cause. This might lead to an inappropriate selection of patients. Whereas, our study tried to include only those patients with AMI due to a plaque rupture. Furthermore, Wang’s study included those with aty- pical chest pain as the control group, which leads to the in- clusion of those with other inflammatory conditions. It can also be explained with respect to the population specificity, which suggests that a certain genetic variant may be relevant to a defined population only.
In conclusion, this study showed that a functional poly- morphism in the promoter region of the MMP-9 gene is strongly associated with an Acute Myocardial Infarction in the Korean population, which was independent of known coronary risk factors. Further study on a larger population will be required to confirm this polymorphism as a potential novel genetic marker for a plaque rupture in Koreans.
This work was supported by grants from the Korean Society of Circulation, Industrial-educational cooperation 2002 and the Cardio- Vascular Research Foundation. Asia.
REFERENCES
1) Falk E, Shah PK, Fuster V. Coronary plaque disruption. Circula- tion 1995;92:657-71.
2) Libby P. Molecular bases of acute coronary syndrome. Circula- tion 1995;91:2844-50.
3) Burleigh MC, Briggs AD, Lendon CL, Davies MJ, Born GV, Richardson PD. Collagen type I and III, collagen content, GAGs and mechanical strength of human atherosclerotic plaque caps:
span-wise variations. Atherosclerosis 1992;96:71-81.
4) Davies MJ, Richardson PD, Woolf N, Katz DR, Mann J. Risk of thrombosis in human atherosclerotic plaques: role of extracellular lipid, macrophage, and smooth muscle cell content. Br Heart J 1993;69:377-81.
5) Moreno PR, Falk E, Palacios IF, Newell JB, Fuster V, Fallan JT.
Macrophage infiltration in acute coronary syndromes: implica- tions for plaque rupture. Circulation 1994;90:775-8.
6) van der Wal AC, Becker AE, van der Loos CM, Das PK. Site of
intimal rupture or erosion of thrombosed coronary atherosclero- tic plaques is characterized by an inflammatory process irres- pective of the dominant plaque morphology. Circulation 1994;
89:36-44.
7) Shah PK, Falk E, Badimon JJ, et al. Human monocyte-derived macrophages induce collagen breakdown in fibrous caps of athe- rosclerotic plaques: potential role of matrix-degrading metallo- proteinases and implications for plaque rupture. Circulation 1995;
92:1565-9.
8) Brown DL, Hibbs MS, Kearney M, Loushin C, Isner JM. Iden- tification of 92-kD gelatinase in human coronary atherosclerotic lesions: association of active enzyme synthesis with unstable angina. Circulation 1995;91:2125-31.
9) Hibbs MS, Hoidal JR, Kang AH. Expression of a metallopro- teinase that degrades native type V collagen and denatured col- lagens by cultured human alveolar macrophages. J Clin Invest 1987;80:1644-50.
10) Wilhelm SM, Collier IE, Marmer BL, Eisen AZ, Grant GA, Goldberg GI. SV-40-transformed human lung fibroblasts secrete a 92kDa type IV collagenase which is identical to that secreted by normal human macrophages. J Biol Chem 1989;264:17213-21.
11) Galis ZS, Khatri JJ. Matrix metalloproteinases in vascular remo- deling and atherogenesis: the good, the bad, and the ugly. Circ Res 2002;90:251-62.
12) Zhang B, Ye S, Herrmann SM, et al. Functional polymorphism in the regulatory region of gelatinase B gene in the relation to se- verity of coronary atherosclerosis. Circulation 1999;99:1788-94.
13) Blankenberg S, Rupprecht HJ, Poirier O, et al. Plasma concent- ration and genetic variation of matrix metalloproteinase 9 and prognosis of patients with cardiovascular disease. Circulation 2003;107:1579-85.
14) Pöläen PJ, Karhunen PJ, Mikkelsson J, et al. Coronary artery complicated lesion area is related to functional polymorphism of matrix metalloproteinase 9 gene: an autopsy study. Arterioscler
Thromb Vasc Biol 2001;21:1446-50.
15) Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial in- farction redefined: a consensus document of The Joint European Society of Cardiology/American College of Cardiology Commi- ttee for the redefinition of myocardial infarction. J Am Coll Car- diol 2000;36:959-69.
16) Galis ZS, Sukhova GK, Lark MW, Libby P. Increased expression of matrix metalloproteinases and matrix degrading activity in vulnerable regions of human atherosclerotic plaques. J Clin In- vest 1994;94:2493-503.
17) Nomoto K, Oguchi S, Watanabe I, Kushiro T, Kanmatsuse K. In- volvement of inflammation in acute coronary syndromes assessed by levels of high-sensitivity C-reactive protein, matrix metallo- proteinase-9 and soluble vascular-cell adhesion molecule-1. J Cardiol 2003;42:201-6.
18) Pasterkamp G, Schoneveld AH, Hijnen DJ, et al. Atherosclerotic arterial remodeling and the localization of macrophages and matrix metalloproteinases 1,2 and 9 in the human coronary artery.
Atherosclerosis 2000;150:245-53.
19) Choi CJ, Lee KS, Baek SH, et al. Association of endothelial NO synthase gene Glu298Asp polumorphism with acute myocardial infarction. Korean Circ J 2001;31:973-81.
20) Inokubo Y, Hanada H, Ishizaka H, Fukushi T, Kamada T, Okum- mura K. Plasma levels of matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-1 are increased in the coronary circulation in patients with acute coronary syndrome. Am Heart J 2001;141:211-17.
21) Kai H, Ikeda H, Yasukawa H, et al. Peripheral blood levels of matrix metalloproteinase-2 and 9 are elevated in patients with acute coronary syndromes. J Am Coll Cardiol 1998;32:368-72.
22) Wang J, Warzecha D, Wilcken D, Wang XL. Polymorphism in the gelatinase B gene and the severity of coronary arterial stenosis.
Clin Sci 2001;101:87-92.