Review Article
봉침을 이용한 무작위배정 비교임상시험연구에서의 유해사례 보고에 대한 체계적 문헌고찰
이운섭⋅김성수
경희대학교 한의과대학 한방재활의학과교실
Reporting of Adverse Events in Randomized Controlled Trials of Bee Venom Acupuncture: A Systematic Review
Woon-Sup Yi, K.M.D., Sung-Soo Kim, K.M.D., Ph.D.
Department of Rehabilitation Medicine of Korean Medicine, College of Korean Medicine, Kyung Hee University
RECEIVED September 25, 2014 REVISED October 9, 2014 ACCEPTED October 15, 2014
CORRESPONDING TO Sung-Soo Kim, Department of Rehabilitation Medicine of Korean Medicine, Kyung Hee University Korean Medicine Hospital, 23, Kyungheedae-ro, Dongdaemun-gu, Seoul 130-872, Korea
TEL (02) 958-9215 FAX (02) 958-9104 E-mail [email protected]
Copyright © 2014 The Society of Korean Medicine Rehabilitation
Objectives Bee venom acupuncture (BVA) is emerging as a potential therapeutic option for several conditions. However, evidence regarding accurate estimates of its adverse events are not available. Therefore, by combining occurrence rates of adverse events in rel- evant randomized controlled trials (RCTs), we have aimed to give an overall estimated rate of each adverse event following BVA intervention.
Methods A systematic search for adverse events of BVA in Pubmed, Cochrane Central Register of Controlled Trials, Embase, NDSL, KoreaMed, KISS, RISS, KISTI, and KMbase was performed. For the quality assessment of the trials, we applied the CONSORT harms reporting recommendations. The overall occurrence rate of each adverse event was as- sessed as the primary outcome. The overall drop-out rate due to adverse events was as- sessed as the secondary outcome.
Results Ten RCTs reported adverse events following BVA. Two RCTs were eligible of fur- ther synthesis. Adverse events of pruritus, localized edema, and erythema occurred sig- nificantly more frequently in the BVA group compared to the control group. Data of drop-outs were available in seven RCTs. However, no comparisons showed a significant difference.
Conclusions Currently evidence of adverse events is far from sufficient for assessing a reliable, precise occurrence rate. Still, limited evidence shows a tendency that adverse events occur more frequently after the appliance of BVA compared to the control. Thus, we await well designed future studies of BVA with more proper and strict harms reporting methods. (J Korean Med Rehab 2014; 24(4):97-109)
Key words Bee venom acupuncture, Adverse events, Systematic review, Randomized controlled trials
Introduction»»»
Bee venom acupuncture (BVA), according to the World Health Organization (WHO) International Stand-
ard Terminologies on Traditional Medicine, is defined as "a special type of acupuncture performed by bee sting (or injection of episin) at a certain point or cuta- neous region"1). It has been reported that BVA might
have therapeutic effectiveness in conditions such as arthritis2,3), chronic low back pain4), adhesive capsulitis5), and cancer6). And until recent date a significant num- ber of researches assessing the effectiveness of BVA have been conducted7). But in clinical decision mak- ing, as much as information of an intervention's bene- fits is important, information of an intervention's harms is also crucial. And clinicians must be supported by a sys- tematic assessment of the balance of benefit to harm8). However, even though BVA is also well known for its risk of serious adverse events such as anaphylaxis9), compared to the evidence assessing the benefits of BVA, the evidence assessing the harms of BVA is lack- ing10). And to the best of our knowledge, no studies up to this date have intended to investigate integrated occurrence rates of adverse events following BVA in- terventions. Thus, a systematic research analyzing the harms of BVA up to date was considered necessary.
The aim of this review is to identify, evaluate, and summarize the information of adverse events of BVA in relevant randomized controlled trials (RCTs). And if appropriate, by combining occurrence rates of adverse events in trials, we aim to give a more reliable and precise overall estimated rate of each adverse event following BVA intervention11).
Methods»»»
1. Terminology for adverse events
The term "adverse event" used throughout this re- view is referred to as "an adverse outcome that occurs during or after exposure to a drug or other inter- vention and which may or may not be caused by the intervention11)." This is different from the term "adverse effect" which is referred to as "an adverse event for which the casual relation between the drug/intervention and the event is at least a reasonable possibility11)."
The terminologies used to describe adverse events
were based on the Common Terminology Criteria for Adverse Events (CTCAE) published by the U.S.
National Cancer Institute12). Terms describing adverse events which are not included in the CTCAE have been presented as similar as the terms the original ar- ticles have described them.
2. Criteria for including studies
1) Types of participants and studies
RCTs of participants of any age group were included.
Studies in English or Korean were included.
2) Types of interventions and controls
Studies which have applied any kind of BVA as an intervention were included. However, studies that have used bee venom for immunotherapy or studies that have reported events of unintentional or non-interven- tional bee stings were excluded. There were no re- strictions on the type of controls.
3) Types of outcome measures
By combining results of individual studies the power and accuracy of the outcome can be enhanced. Moreover it may reveal a consistency across studies that wouldn't be exposed if the results were presented indivi- dually13). For these reasons, we set the overall occurrence rate of each adverse event as the primary outcome.
Drop-out rates are also acknowledged as important information in reviews examining harms since "the ulti- mate decision after experiencing an adverse event is reflected in drop-outs or withdrawals"14). The overall drop-out rate due to adverse events was assessed as the secondary outcome.
There were no restrictions regarding the type or se- verity of the adverse events.
3. Search method
Databases for the search were selected based on the
"Core databases" recommended by the National Evidence-based Healthcare Collaborating Agency (NECA) of Korea13). Pubmed, Cochrane Central Register of Controlled Trials, Embase, and six Korean databases (NDSL, KoreaMed, KISS, RISS, KISTI, KMbase) were selected for the search. All databases were searched in October 2014 using the following search terms: "bee venom" OR "apipuncture" OR "bee sting therapy". For searching Korean databases the following terms in Korean, which can be translated as 'BVA', were used in conjunction with the English search terms: "봉침"
OR "봉독" OR "봉약침". Efforts to include non-pub- lished data were not made.
4. Data collection and analysis
1) Selection of studies
First, by examining the title and abstract, RCTs rele- vant to BVA were screened. RCTs were identified based on the study design classification algorithms in- troduced by Hartling et al.15) and the National Evidence- based Healthcare Collaborating Agency of Korea13). Once a RCT was identified, the full text of the study was reviewed to assess if it had met the inclusion criteria. If the identified study had properly reported any adverse event of BVA, the study was considered eligible.
2) Data extraction
Incidence rates of the adverse events and numbers of drop-outs due to adverse events were assessed. The numbers of events or drop-outs were derived from the particular study's intention to treat analysis set (i.e. the study's original participant assignment). However, if the exact number of participants who have experi- enced a certain adverse event had not been reported clearly, or if the adverse event had been presented in a non-dichotomous form which cannot be interpreted as an exact number of events (e.g. presented as a vis- ual analogue scale), the data was excluded.
3) Quality assessment of studies
Quality assessment tools usually apply only to the beneficial effects of the intervention rather than its harmful effects8). But in studies reporting harms differ- ent factors may have larger influence on the quality of the study than the factors commonly evaluated in tools assessing benefits16). Therefore, applying a quality as- sessment tool particularly designed to evaluate the quality of studies reporting harms would be a more appropriate approach.
In this review, for the quality assessment of the tri- als, we applied the 2004 CONSORT harms reporting recommendations14). However, since the CONSORT harms reporting recommendations are generally open-ended, a coding manual based on the 10 de- scriptors of the CONSORT harms reporting recom- mendation checklist developed by Smith
et al.
17) was used in conjunction with the CONSORT checklist.4) Assessment of heterogeneity
Heterogeneity was assessed using the χ2 statistic and I2 statistic with the Revman 5.2 software (Review Manager (RevMan) Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.).
5) Data analysis and synthesis
Synthesizing adverse events of different severity may lead to bias. Therefore, only adverse events reported with a measurement of severity were considered eligi- ble for synthesis. In this review, adverse events re- ported with a CTCAE grade or a Mueller grade were considered eligible. The general guideline of CTCAE (Table I) propose clinical descriptions of severity for adverse events12). The Mueller grading method (Table II) is a classification of severity for allergic reactions in- troduced by Mueller HL18,19). Only adverse events with the same CTCAE grade or Mueller grade were synthe- sized together.
The Revman 5.2 software was used for the calcula-
Grade 1 Mild;* asymptomatic or mild symptoms; clinical or diagnostic observations only; intervention not indicated.
Grade 2 Moderate; minimal, local or noninvasive intervention indicated; limiting age-appropriate instrumental ADL
†.
Grade 3 Severe or medically significant but not immediately life-threatening; hospitalization or prolongation of hospitalization indicated; disabling; limiting self care ADL
‡.
Grade 4 Life-threatening consequences; urgent intervention indicated.
Grade 5 Death related to AE.
*A Semi-colon indicates ‘or’ within the description of the grade,
†Instrumental ADL refer to preparing meals, shopping for gro- ceries or clothes, using the telephone, managing money, etc,
‡Self care ADL refer to bathing, dressing and undressing, feeding self, using the toilet, taking medications, and not bedridden.
Table I. General Guideline of CTCAE for Grading Severity of Adverse Events
Large local reaction* Swelling at site of sting with diameter > 10 cm, lasting > 24 hrs.
Grade I Generalized urticaria, itching, malaise, anxiety.
Grade II Any of the above, plus two or more of the following: angioedema, constriction in chest, nausea, vomiting, diarrhea, abdominal pain, dizziness.
Grade III Any of the above, plus two or more of the following: dyspnea, wheezing, stridor, dysphagia, dysarthria, hoarseness, weakness, confusion, fear of death.
Grade IV Any of the above, plus two or more of the following: drop of blood pressure, collapse, loss of conscious- ness, incontinence (urine, stool), cyanosis.
*Referred to as “grade 0” in certain studies
20)Table II. Classification of Allergic Reactions by Mueller HL., Modified
tions. The influence of BVA on the occurrence of ad- verse events in the intervention participants versus the occurrence of adverse events in the control participants was converted into a risk ratio with a confidence inter- val (CI) of 95%. Risk ratios were presented as a forest plot depending on its heterogeneity. If the hetero- geneity was proven to be significant (p value of the χ2 statistic <0.1 or I2≥50%), a random effect model weighted by the Mantel-Haenszel method was applied.
If the heterogeneity was proven to be not significant, a fixed effect model weighted by the Mantel-Haenszel method was applied. p<0.05 was considered as being statistically significant.
Using the Revman 5.2 software, the influence of BVA on the occurrence of drop-outs in the inter- vention participants versus the occurrence of drop-outs in the control participants was converted into a risk ra- tio with a confidence interval of 95%. Risk ratios were presented as a forest plot depending on its heteroge- neity. If the heterogeneity was proven to be significant
(p value of the χ2 statistics <0.1 or I2≥50%), a ran- dom effect model weighted by the Mantel-Haenszel method was applied. If the heterogeneity was proven to be not significant, a fixed effect model weighted by the Mantel-Haenszel method was applied. p<0.05 was considered as being statistically significant.
Results»»»
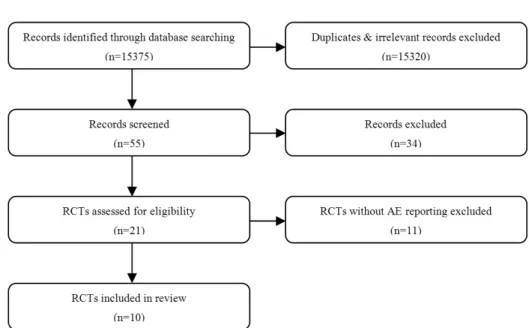
1. Results of the search (Fig. 1)
By assessing titles and abstracts of the search, rele- vant studies were screened and duplicates were removed. The full texts of the relevant studies were examined for any reports of adverse events following BVA. Ten RCTs were screened.
Fig. 1. Study flow diagram.
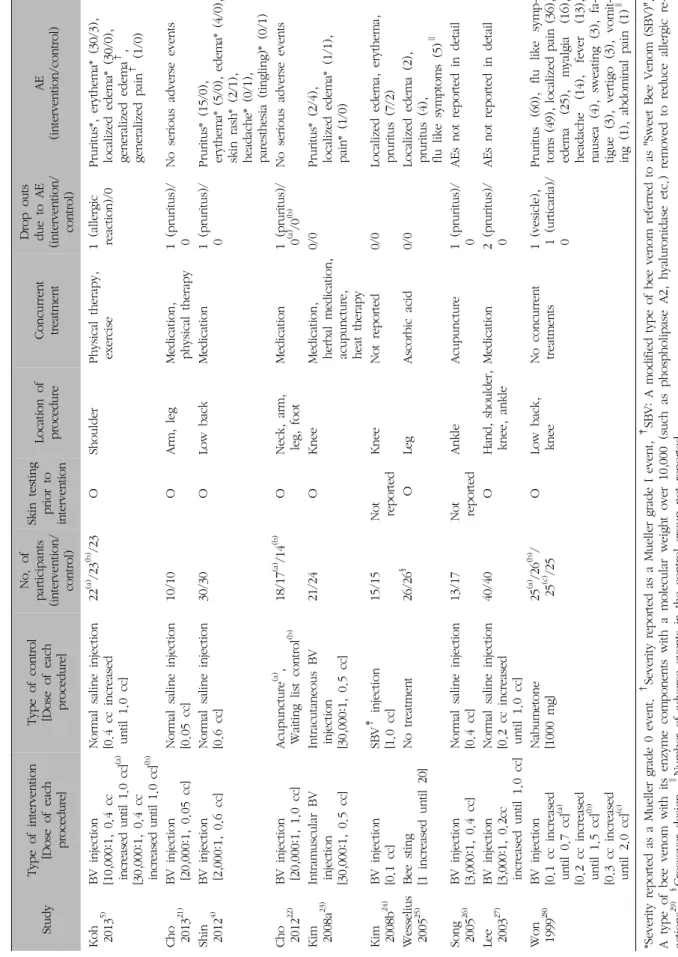
2. Characteristics of adverse events reported in RCTs (Table III)
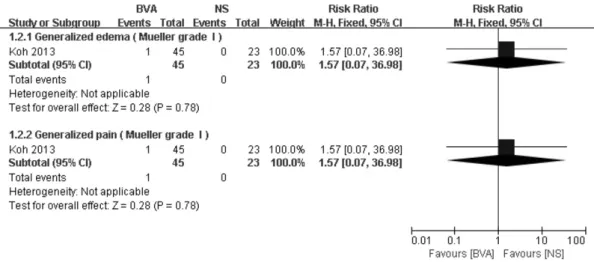
Pruritus was reported in all of the studies either as an adverse event or as a reason for drop-out. General- ized symptoms such as generalized edema, generalized pain, flu like symptoms, and fever were reported in only three studies. Of the three studies which reported generalized symptoms, a study by Koh et al. reported an event of generalized edema and pain which was categorized by the researcher as a Mueller grade I event. Severity of the other adverse events reported in the study were categorized as Mueller grade 0 events5). Of the ten studies, seven studies reported drop-outs due to adverse events. Five of the studies reported pruritus as the reason of the drop-outs.
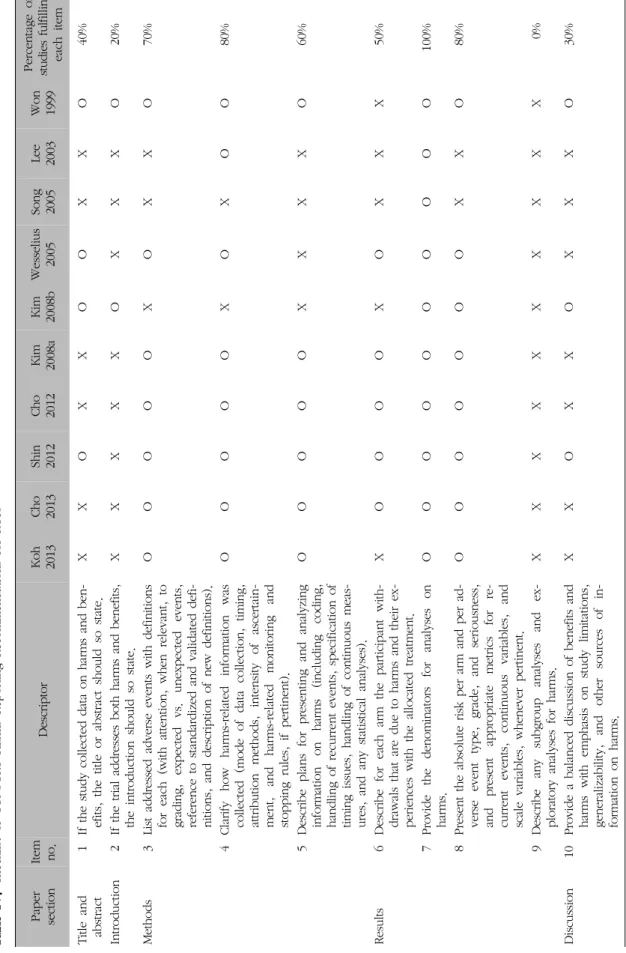
3. Quality assessment of adverse event report- ing in RCTs
The descriptors of the ten CONSORT harms report- ing recommendation items with the overview of fulfill- ment for each item are presented in Table IV. The coding manual states that the items have to be fulfilled in the section specified (e.g. introduction, results etc.)
in the recommendation. If a content of a certain item was described in another section rather than the sec- tion it should have been mentioned, even if it had ful- filled other conditions of the item, it was not counted as satisfying the item17). Recommendations four, seven, and eight were reported in 80% or more of the studies. Item four was considered as fulfilled if the study had described any information about how harms data was collected. This appeared as having a high re- porting rate since most of the studies described how they had performed a skin test prior to the trial. Item seven was satisfied if the study had reported a denom- inator for each arm. All the studies have reported this item. Only two of the ten studies (20%) addressed harms in the introduction. No studies described any subgroup analysis or exploratory analysis for harms.
But the low reporting rate of this item is consistent with other researches assessing quality of harms reporting. This is because subgroup analysis or ex- ploratory analysis for harms is rarely carried out in most RCTs17,30,31).
4. Occurrence rates of adverse events
Three RCTs reported the severity of adverse events
St udy T yp e of in te rv en tio n [D os e of e ach pr ocedur e]
Typ e of cont ro l [D os e of e ach pr ocedur e]
No . of p artic ip an ts (i nt er vent ion/ cont rol ) Sk in t es tin g pr io r to in te rven tion
Lo cat ion of pr ocedur e Concur re nt tre atm en t D rop out s due to A E (i nt er vent ion/ cont rol )
AE (i nt er vent ion/ cont ro l) Ko h 2013
5)B V i nj ect ion [10,000: 1, 0 .4 cc in cr ea se d un til 1. 0 cc ]
(a)[30,000: 1, 0 .4 cc in cr eas ed u nt il 1. 0 cc]
(b)N or m al s al in e in je ct io n [0 .4 cc in cr eas ed unt il 1.0 cc]
22
(a)/2 3
(b)/2 3 O Shoul der Phys ica l th er apy, ex er ci se 1 (alle rg ic re act ion) /0 Pr ur itus *, e ry th em a* ( 30/ 3), lo ca liz ed edem a* (30/0) , gener al ized edem a
†, gener al ized p ai n
†( 1/ 0) Cho 2013
21)B V i nj ect ion [20,000: 1, 0.05 cc] N or m al s al in e in je ct io n [0.05 cc] 10/ 10 O A rm , le g M edi cat ion, phys ic al t her ap y 1 (p ru ritu s)/ 0 N o ser ious adver se event s Shi n 2012
4)B V i nj ect ion [2,000: 1, 0.6 cc] N or m al s al in e in je ct io n [0 .6 cc] 30/ 30 O Low b ack M edi cat io n 1 (pr ur itus )/ 0 Pr ur itus * (15/ 0) , er yt he m a* (5 /0 ), e dem a* (4/0), sk in r as h* ( 2/ 1), heada che* ( 0/ 1) , par es the si a (t ingl ing) * (0 /1 ) Cho 2012
22)B V i nj ect ion [20,000: 1, 1.0 cc] Acupunct ur e
(a), W aitin g lis t co nt ro l
(b)18/ 17
(a)/14
(b)ON ec k, a rm , le g, f oot M edi cat ion 1 (pr ur itu s) / 0
(a)/0
(b)N o ser ious adver se event s Ki m 2008a
23)In tra m us cu la r B V in je ct io n [30,000: 1, 0.5 cc]
In tr acut aneous B V in je ct io n [30, 000: 1, 0.5 cc]
21/ 24 O K nee M edi cat ion, her ba l m edi cat ion, ac up unct ur e, hea t ther ap y
0/0 Pr ur itu s* ( 2/4) , lo ca liz ed e de m a* (1 /1 ), pai n* ( 1/ 0) Ki m 2008b
24)B V i nj ect ion [0 .1 cc] SB V
‡i nj ect ion [1 .0 cc] 15/ 15 N ot re p orte d K nee N ot r ep or ted 0/0 Loca liz ed edem a, er yt hem a, pr ur itus ( 7/ 2) W esse liu s 2005
25)B ee st in g [1 i ncr eas ed unt il 20] N o tr eat m ent 26/ 26
§O Leg As cor bi c aci d 0/0 Loca lized edem a (2) , pr ur itus ( 4) , flu lik e sym p to m s (5)
∥Song 2005
26)B V i nj ect ion [3,000: 1, 0.4 cc] N or m al s al in e in je ct io n [0 .4 cc] 13/ 17 N ot re p orte d A nk le A cu p un ctu re 1 (p ru ritu s)/ 0 AEs not r ep or te d in d et ai l Lee 2003
27)B V i nj ect ion [3 ,000: 1, 0 .2cc in cr eas ed unt il 1.0 cc]
N or m al s al in e in je ct io n [0 .2 cc in cr eas ed unt il 1.0 cc]
40/ 40 O H an d, s ho ul de r, knee, ankl e M edi cat ion 2 (pr ur itu s) / 0 AEs not r ep or te d in d et ai l Wo n 1999
28)B V i nj ect ion [0 .1 cc in cr eas ed unt il 0.7 cc]
(a)[0 .2 cc in cr eas ed unt il 1.5 cc]
(b)[0 .3 cc in cr eas ed unt il 2.0 cc]
(c)N abum et one [1000 m g] 25
(a)/2 6
(b)/ 25
(c)/2 5 OL ow b ac k, knee N o concur re nt tre atm en ts 1 (ves ic le ), 1 (ur tic ar ia )/ 0
Pr ur itus (60) , flu like sym p - to m s (49) , lo cal ized p ai n (36), edem a (25) , m ya lg ia (16), heada che (14), fever (13), naus ea (4), sw ea ting (3), fa - tig ue (3) , ver tig o (3), vom it- in g (1 ), a bdom in al pai n (1 )
∥*Sever ity re p or ted as a M uel le r gr ade 0 event .
†Sever ity repor ted as a M uel ler g rade I event ,
‡SB V : A m odi fied typ e of bee venom r ef er re d to a s "S w eet B ee V en om ( SBV )". A t ype of bee venom w ith its enzym e com ponent s w ith a m ol ecul ar w ei gh t over 10, 000 (such as p hos phol ip as e A 2, hyal ur oni das e et c. ) re m ov ed t o re du ce a lle rg ic re - act ions
29),
§C ros sover d es ig n,
∥N um ber o f adver se event s in th e cont ro l gr oup not r ep or te d.
T ab le III. A dver se Event s (A E) Rep or ted in RC T s
Paper se ct io n Item no. De sc ri p to r Ko h 2013 Cho 2013 Sh in 2012 Cho 2012 Ki m 2008a Ki m 2008b We ss el iu s 2005 Song 2005 Le e 2003 Wo n 1999
Per cent age of st ud ie s fu lfi lli ng ea ch ite m Ti tle a nd abs tr act 1 If t he st udy col le ct ed dat a on ha rm s and ben - ef its , the tit le o r ab st ra ct s houl d so s ta te . X X O X X O O X X O 40% In tr oduct ion 2 If t he tr ia l addr es se s bot h ha rm s and benef its , th e in tr oduct ion shoul d so s ta te . XXXXX O X X X O 20 % M et hods 3 Li st a ddr ess ed adver se event s w ith def ini tions fo r each (w ith at te nt ion, w hen re leva nt , to gr adi ng , ex p ect ed vs . unex p ect ed event s, re fe re nce to s ta ndar di zed and val idat ed def i- ni tions , and des cr ip tion of n ew d ef in iti ons ).
OOOOO X O X X O 70 % 4 C la ri fy how har m s- rel at ed inf or m at ion w as co lle ct ed (m od e of da ta co lle ct io n, tim in g, at tr ibut ion m et hods , in te ns ity of as cer ta in - m ent , and ha rm s- re la te d m oni tor ing and st oppi ng rul es , if p er tinent ).
OOOOO X O X OO 80 % 5 D es cr ib e pl an s for pr es ent ing and anal yzi ng inf or m at ion on har m s (i ncl udi ng codi ng, handl in g of r ecur re nt event s, s p eci ficat ion of tim ing is su es , handl in g of c ont inuous m ea s- ur es, and any st at is tical a nal ys es ).
OOOOO X X X X O 60 % R es ul ts 6 D es cr ibe for each ar m th e par tici p an t w ith - dr aw al s th at a re due to har m s and th ei r ex - p er ie nc es w ith t he a llo ca te d t re at m en t.
X OOOO X O X X X 50 % 7 Pr ovi de the denom in at or s fo r an al ys es on har m s. OOOOO O O O OO 100% 8 Pr es ent t he abs ol ut e ri sk per a rm a nd per ad - ver se event ty p e, gr ade, and ser iousnes s, and p res ent app ropr ia te m et ri cs for re - cur re nt event s, cont inuous var ia bl es , an d sca le var ia bl es , w henever p er tinent .
OOOOO O O X X O 80 % 9 D es cr ib e any subgr oup anal ys es and ex - p lor at or y anal yses f or h ar m s. XXXXX X X X XX 0% D is cus si on 10 Pr ovi de a bal anced di scus si on of b enef its and har m s w ith em phas is on st udy lim ita tions , gener al izabi lit y, and ot her sour ces of in - fo rm at ion on har m s.
X X O X X O X X X O 30%
Ta bl e IV . C heck lis t of CO N SO R T H ar m s Rep or ting Recom m enda tions f or R CTs
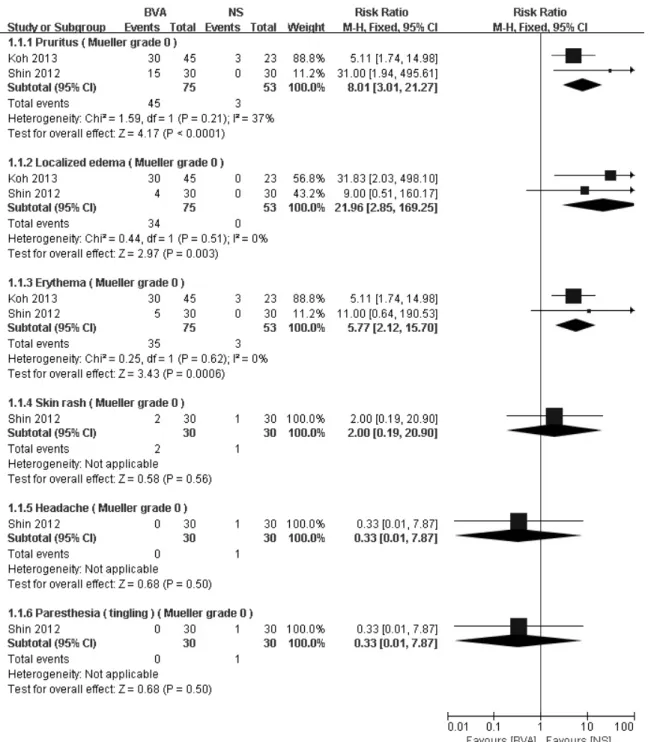
Fig. 2. Comparison: 1. adverse events of BVA versus normal saline injection, outcome 1.1 Mueller grade 0 events.
BVA: bee venom acupuncture, NS: normal saline, M-H: Mantel-Haenszel, CI: confidence interval, df: degree of freedom.
with the Mueller grading method. Two of the three RCTs compared the effect of BVA with normal saline injection as a control4,5). The other compared the effect of BVA in different depths of injection23). Only studies using normal saline as a control were included in the
synthesis. And only adverse events categorized as the same grade of severity were synthesized together.
Heterogeneity was explored in comparisons of pruritus, localized edema, and erythema. Due to non-significant heterogeneity (pruritus: χ2=1.59, I2=37%, localized ede-
Fig. 4. Comparison: 2. drop-out rates due to adverse events of BVA versus controls.
BVA: bee venom acupuncture, NS: normal saline, M-H: Mantel-Haenszel, CI: confidence interval, df: degree of freedom.
Fig. 3. Comparison: 1. adverse events of BVA versus normal saline injection, outcome 1.2 Mueller gradeⅠevents.
BVA: bee venom acupuncture, NS: normal saline, M-H: Mantel-Haenszel, CI: confidence interval, df: degree of freedom.
ma: χ2=0.44, I2=0%, erythema: χ2=0.25, I2=0%), the fixed effect model weighted by the Mantel-Haenszel method was applied. Forest plots of adverse events are presented in Fig. 2 and 3. Adverse events of pruritus
(RR=8.01, 95% CI: 3.01∼21.27, p<0.0001), localized edema (RR=21.96, 95% CI: 2.85∼169.25, p=0.003), and erythema (RR=5.77, 95% CI: 2.12∼15.70, P=0.0006) oc- curred significantly more frequently in the BVA group
compared to the control group.
5. Drop-out rates due to adverse events
In order to reduce bias, only studies which have used BV injection as the type of intervention were considered eligible for data synthesizing. Data of drop-out rates from seven trials were available. Due to low heterogeneity, (BVA versus normal saline injection:
χ2=0.30, I2=0%, BVA versus total control: χ2=0.43, I2=0%) a fixed effect model weighted by the Mantel- Haenszel method was applied (Fig. 4). However, no comparisons showed a significant difference (BVA ver- sus total control: RR=2.84, 95% CI: 0.90∼8.96, P=0.08, BVA versus normal saline injection: RR=3.17, 95% CI:
0.81∼12.44, p=0.10, BVA versus acupuncture: RR=2.84, 95% CI: 0.12∼65.34, p=0.51, BVA versus Nabumetone:
RR=1.69, 95% CI: 0.08∼34.03, p=0.73).
Discussion»»»
Many decisions in clinical practice require careful balancing of the benefits and harms32). In this review we aimed to evaluate the harms of BVA by assessing reports of adverse events and drop-out rates in RCTs.
The overall occurrence rate of each adverse event reported was the primary outcome. However, due to the small number of studies and the low reporting rate of adverse events, available data for analysis was scarce. Low reports of the severity of adverse events also reduced eligible data for synthesis. The results of the limited synthesis showed that only adverse events of pruritus, localized edema, and erythema appeared to occur significantly more frequently in the BVA group compared to the control group. Only two RCTs were included in this synthesis. And therefore it would be difficult to draw a generalized result. In addition, it must be stated that there is also a chance of bias due to differences between researchers and differences in
methods of adverse event reporting33). Therefore, we can only conclude that more validated criteria for re- porting adverse events are in need.
The overall drop-out rate due to adverse events was the secondary outcome. Drop-out rates from seven RCTs were available for the synthesis. However, no comparisons showed a significant difference. It should also be mentioned that drop-outs may occur due to a combination of reasons. And reasons other than the adverse events might attribute more to the decision whether to withdraw or not from the trial14). Pressure of the trial condition, unblinding of the intervention16), and different thresholds in deciding to continue or not8) may influence drop-out rates. The fact that pruri- tus was the reason for drop-outs in five of the seven studies indicate that most of the drop-outs might have occurred due to simple irritation rather than the harm inflicted by the adverse event.
By summarizing the reports of adverse events, we have discovered a different tendency in the reporting in RCTs compared to other study designs. For exam- ple, where several case reports have reported events of anaphylaxis34-37), among RCTs, only a study by Koh et al. reported an event more severe than a Mueller grade 0 reaction5). Two other studies reported events of flu like symptoms or fever, but such symptoms alone are difficult to be considered as an anaphylactic reaction. Certain reasons such as the originally low in- cidence rate of anaphylaxis (0.014%)38) and the rela- tively small sample size of the RCTs may explain some part of why reporting of anaphylaxis are very low in the trials. The exclusion of participants with hypersen- sitivity or high risk of anaphylaxis prior to the trial via history taking and skin testing also would have contri- buted to making anaphylaxis a highly uncommon event.
Dermatologic adverse events reported in RCTs also show a distinct characteristic compared to case reports.
Most of the dermatologic adverse events reported in RCTs were mild and temporary symptoms such as pru- ritus, localized edema, erythema, and skin rash. Only a
study by Won et al. reported a case of a vesicle and a case of urticaria28). This is different from case reports reporting much more developed dermatologic adverse events such as granulomas or plaques39-43). Considering the fact that most case reports are stating that these dermatologic events were observed weeks or months after the initial treatment, the relatively short follow up durations of RCTs could give a partial explanation of why there were no reporting of developed dermato- logic adverse events in trials.
Other limitations related to the reporting of adverse events of BVA can be pointed out. First, BVA treat- ment in general has expected features of pruritus, pain, swelling when applied. However, currently there is no consensus of to what degree it should be ac- cepted as an expected common reaction. Therefore, there would be differences in to what degree a re- searcher might consider a certain reaction as an ad- verse event and report the symptom. Criteria of ex- pected reactions of BVA built on clinical evidence are in need in conducting future researches.
Second, methods of monitoring and detecting ad- verse events are different across studies. Moreover, many studies do not even describe this information in the article. Since different methods can yield different results, this can be a source of substantial bias8). Crite- ria for monitoring and detecting adverse events in clin- ical trials are also in great need.
Third, nine of the ten studies included in this review were carried out in South Korea. A prior review of BVA had shown concerns that this could lead to pub- lication bias and location bias44).
Conclusion»»»
By conducting this review we have aimed to identi- fy, evaluate, and summarize the evidence regarding ad- verse events of BVA in RCTs. We have also aimed to give an overall estimated rate of each adverse event
that studies cannot provide individually.However, evi- dence of adverse events in RCTs up to date is far from sufficient for assessing a reliable, precise occurrence rate. Thus, we await well designed and well organized future studies which properly report adverse events of BVA. Still, limited evidence which is available shows a tendency that adverse events occur more frequently af- ter the appliance of BVA compared to the control.
Since clinical decisions applying this information may influence a patient's condition considerably, it is crucial that additional precise evidence should be provided for practice. Therefore, even though any concrete con- clusions cannot be stated with the current evidence, the fact that more research with better methodological quality is needed is evident.