大협itJ:射線醫장!會誌 第 23~ 第 3 號 pp. 485 - 491 , 1987 Journal 01 Korean Radiological Society, 23(3) 485-491 , 1987
惡性鐵維性組織球睡에 對한 放射線學的 所見
慶熙大學校 醫科大學 放射線科學數室
朴基좋·李善和·尹 爆·成東몽·安致烈
- Abstract -
Radiologic Evaluation of Malignant Fibrous Histiocytoma
Ki 500n Park, M.D., 5un Wha Lee, M.D., Yup Yoon, M.D., Dong Wool
‘
5ung, M.D., Chi Yul Ahn, M.D.Department of Radiologι Kyung Hee University Hospital
Malignant fibrous histiocytoma is a new malignant tumor entity of histi 。이tic origin which arises as a primary tumor of the bone as well as the soft tissue
Radiologic features of 12 cases of pathologically proven intra-and extraosseous malignant fibrous histiocytoma were analyzed
The results were as follows
1. Seven cases were of soft tissue origin and 5 cases were of primary bone origin 2. Seven were male and 5 were female: Eight cases were beyond 5th decades
3. The clinical presentations of malignant fibrous histiocytoma of the soft tissue origin were a mass with rapid growth or high rate of local recurrence. The roentgen evidence of soft tissue density mass was demonstrated in 7 cases and scintigraphic evidence of cortical invasion was suggested in 2 cases
4. Malignant fibrous histiocytoma arising from bones had ill defined moth-eaten osteolytic lesion with cortical destruction, periosteal reaction and soft tissue extension
5. Among 12 cases, there were 2 cases of pulmonary metastases and 2 cases of osseeous metastases 6. In the presence of soft tissue mass with locally aggressive behavior and/or nonspecific roentgen features
of malignant bone tumor, one should consider the possibility of malignant fibrous histiocytoma
I .
績 論惡性繼維性組織球睡은 中年 以後에 好發하는 組織肉 睡무j료 病理組織學的으로 結鍾細뼈의 와정형( stor ifo • rm) 配列과 組織細뼈의 增꺼훌이 特徵이고 1-7) 臨皮的 所 見과 鍵後가 他 惡、性睡傷인 骨肉睡, 織維肉睡, 就鍾細뼈
이 논문은 1987 년 3 월 21 일에 접 수하여 1987 년 4 월 1 일에 채택되었음.
485
肉睡 等파 마료므로 1960 年代 初부터 새로운 睡場群£
로 연구되어 최근에는 하나위 獨立된 睡場으로 안정되
고 있다 1,2 , 8-10:
著者들은 慶熙大學校 醫科大學 附屬病院에서 病理組 織學的 o i료 確양된 12 例의 節骨짧系 惡、性繼維性組織球 睡을 경험하였기에 이을 文敵考察과 함께 報告하는 바 이다.
- 大행放射線醫學會誌 : 第 23월 第3 號 1987 -
ll.
對象 및 方法1) 對 象
1978 年부터
1986
年까지 慶熙大學校 醫科大學 附屬病院에 서 수술 및 病理組織學的으로 確該된 惡性繼維性 組織球睡
12
例를 對象으로 하였다.2) 方 法
總 12 例中 全例에서 單純 X 線握影을 施行하였고, 電 算化斷層擬影 (이 후 CT로 약함)
2
例, 骨신티그라고I7
例, 血管造影術을 2 例에 서 뼈行하였 다.IlI.
結 果38 歲 된 여자로 約 4 個月前부터 左예趙骨下端의 局 所痛효과 함께 睡塊가 觸知되어 來院하였다1:필純 X 線 根影上 顆骨下端흩ß 骨幹에 형좋界가 不分明한 吸收性 骨 破壞所見, 骨被의 破壞 및 骨體反應。1 觀察되었마 (Fig
l-A)
. 骨肉睡 推定하에 生檢을 施行한 결과 惡性繼維 性組織球睡으로 確該되 어 總70
Gy 의 放射線照射을 받 았다. 以後 점차 睡塊가 커져 左測下展切斷術파 뺨骨移 植術을 施行하였으냐 約 l 年後 追助檢훌時 }jjfï 및 骨轉 移에 의한 多發性의 8市結節陰影 및 左예탑lij며骨破壞所見 이 觀察되 었마 (Fig.l-B).:ffE例 2 :
54 歲 된 남자로 약
10
年前부터 左예 장단지 용ß位에 睡塊가 觸갖n되 어 2 며의 切除術을 받았으나 再發히여 來 院하였다. 血淸檢호上 알칼리성 안산효소{直가 8.7u/ß 로 增加된 외에 異常所見응 없었다. 單純 X 線嚴影上 左 總 12 例의 惡性織維性組織球睡응 骨에서 發生한5
뼈~ 장단지에 軟組織 睡塊陰影 (Fig.2-A) 이 血管造影術 例 및 軟組織에서 發生한 7 例로 이들의 性別, 年敵, 放 上 新生血管 및 睡塊內 造影齊j梁色所見이 觀察되었마 射線學的 所見 等에 관한 要約응Tabl
e 1 및 2 와 같(Fig.2
-B).
99mTc-MDP 신티그라고l 上 睡塊內 放射다. 能훌積所見 및 憐援骨願홉潤에 依한 骨被의 放射能增 J.m
tE例 報告
:ffEØl J
1 :所見이 있었마 (Fig.2-C). 血管睡 훌?斷下에 生檢을 施 行한 結果 惡性繼維性組織球睡으로 確該되어 (Fig.
2
D)
下破 切斷術을 施行하였 다.Table
1.Summary of 7 patients with
MalignantFibrous Histiocytoma of Soft Tissue Radiologic Features
Patient Age Sex Location
Soft tissue mass Cortical
invasionMetastasis Treatment (yrs)
1 57 M Knee
+Excision
2 43
M Thenar
+ (+)Lung Enblock
resection
3 54
M Leg
+ (+)Excision
4 60 F Arm
+Bone Radical
eXClslOn
5 56
M Thigh
+Enblock
resection
6
30M Thigh
+ Excision &chemotheraphy
7 61 M T
high +Excision
) positive fid
ning on scintigraphypresence of periosteal reaction
- 朴판 ì~1-外 강E ↑j;熾빠性 iJl織球8重에 對한 放射綠£양 (1낀 Nr 見
f숱例 3 :
22
歲 여자로 15 日 前부터 右뼈 大題骨下部에 痛효이 發生하여 來院하였다. 單純 X 線握影上骨被質의 破壞 및 境界가 不分明한 吸J&性 職眼性 骨破壞 所見。 1 大眼骨骨端에서 觀察되 었고 (Fig.3-A) CT 上 骨被質의 破 壞 및 壞死를 同伴한 周圍軟組織으호 波及된 睡塊를 더 正確히 얄 수 있었다HFig.3-B). 骨肉睡£로 該斷하였 무냐 骨生檢上 惡 f生觸維性組織球睡으로 確장되 었다.
99mTc-MDP 신티그라피上 病變部位에 放射能 홉積이
Table 2. Summary of 5 Patients
withMalignant Fibrous Histiocytoma of Bone
Radiology feature
Patient Age Sex Location Cortial
changeSoft tissue
Osteolytic
lesionMetastasis
Periosteal reaction Cortical destruction extension (yrs)
2 3
4
548 M Femur diaphysis
&metaphysis
Moth.eaten with
sclerosis22 M Femur diaphysis Moth.eaten
38F Femur diaphysis Moth-eaten
with sclerosis
22 M Tibia diaphysis Moth-eaten
41 F L2-4 Moth-eaten
*
presence of pathologic fracture
A
+ + +
+ + +
+ + +
Lung & bone
+* + +
+ ¥ + +
~
B
Fig.
1.Case 1:
A. A ill defined osteolytic lesion
with corticalbreak and periosteal
reactionis noted
indiaphysis of the tibia.
B. One year follow up chest P A shows multiple
nodular densities in both lung fields and a ill
defined osteolytic lesion in
left scapula,representing pulmonary
and osseousmetastases.
- 大韓放射線뽑짱會誌 : 第23썽 짜
3
跳1987 -
A B
Fig. 2. D.
There is storiform area from malignant fibrous
histiocytoma showing hyalinization resulting inseperation of plemorphic tumor cells
(H &Ex200)
‘減少펀 部位와 。l를 둘러싸눈 放射能 곁홉積。1 增加펀 홈ß 位가 觀察되었마 (Fig. 3-C). 愚者는 化學續法을 받던 중 死亡하였다.
f훈 f列 4 :
41
歲 펀 여자로3
個月 前에 發生한 廳痛을 主訴로 入院하였 다. 過去歷上7
年前 廳推骨睡場으로 放射線治 續를 받았으며 入院당시 施行한 單純X 線嚴影上 第 2 및Fig. 2. Case 2:
A. There is a rounded lobulated border of soft tissue density mass (6.5 x 5cm in size) in mid part of the
calfB. Angiogram reveals fine tumor vascularity and homogeneous tumor
staining inthe mass
C.
Bone scintigraph shows extraskeletal activi- ty within the mass and localized increased activity at adjacent cortex.
C
3H맺推體 및 推幹, 練突起의 骨被質破壞를 同伴한 隨眼 性 骨吸收性 病變 및 憐接軟組織으로 波及펀 睡塊 陰影 이 觀察되 었다 (Fig.4-A). 手術前 양斷은 再發된 骨 巨細 1泡睡이나 骨動 JW짧製n包였으나 휴推딩切除術 施行後 病理組織學的으로 骨軟骨睡。1 疑心되었다. 約 6 個月後 四股빠L揮 및 排1*不能으로 再入院時 施行한
CT
J: 病 變이 보마 머 波及되 었으며 (Fig. 4-B) 再手術後 病理 組織學的 最終該斷은 惡、性織維性組織球睡이 었다.1V.
考 察1972
年Fe
ldman 等 8)이 原發性 骨性惡性鐵維性組織 球睡에 대해 처음 報告한 이래 130 例가 報告되었고Spai ni e r
11)는 407 例의 原發性 骨健場중 15 例의 惡 性織維性組」織球睡의 짧生을 報告한 바 있다. 著者들이 經驗한 惡性織維性組織球睡 總 12 例중 7 例는 軟組織 에서, 5 例는 骨에서 發生하였다.年敵分布는 10 代에서
70
f생! 이르기까지 多樣하나11-14) 大部分 40 代以後에 好發히며 男女比는 3:2 로
男子에 많은 것으로 알려져 있 아 9 , 12 , 1시 著者들의 12 例에서도 40 歲以後가 8 例였고 男子가 7 例,女子가
5
- 488-
A
C
A
;jH~i후 外‘ }띤性織쩌E↑í組織f;J<H핀에 對한 放 Mt.Ii:장l的 Nr見
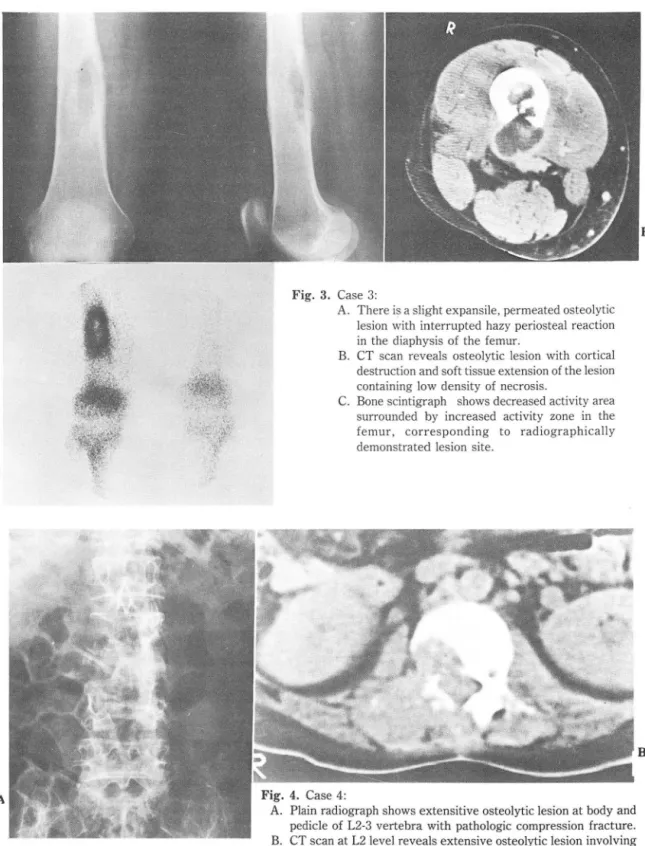
Fig. 3 . Case 3
A. There is a slig ht expansile
,permeated osteolytic lesion with interrupted hazy periosteal reaction in the diaphysis of the femur.
B. CT sc an reveals osteolytic
lesion with corticalde struction an d soft tissue exte
nsion of the lesion containing low density of necrosis.
C.
Bone scintigraph shows decreased activity area surrounded by increased activity zone
int he femur
,corresponding to radiogr aphi cally demonstrated lesion s
iteFig. 4. Case 4:
A. Plain radiograph shows extensitive osteolytic lesion at body and pedicle of L2-3 vertebra with pathologic compression fracture.
B. CT scan at L2
level reveals extensive osteolytic lesion involvingright lateral part of the body and right sided posterior arch with cortical destruction , which extend
intoepidural space and multifidus and longissimus dorsi muscles
489
B
B
- λ*!~IIÁ4‘t짧썩젠*註: 짜\23卷 잉 3 \싸 1987 -
例였다.
짧生部位는 Weiss 等 9) 은 軟組織에서 發生한 惡f生繼 維性組織球睡의 경우 上뾰, 下鼓, 後願題, 體幹 및 頭願 部 順이고 骨에 서 發生한 경우엔 그 發生頻度는 大服骨,
顆骨, 上廠骨, 骨盤骨, 助骨, 頭蓋骨, 頻面骨 및 업F骨 等 의 順이 며 長骨’의 骨幹端部에 서 好發함을 報告한 바 있
마5 , 9 , 10 ,12 , 14 , 15: 著者들의 軟組織에서 發生한 惡性繼維 性組織球睡의 경우엔 下뾰 5 例, 上關部 및 手掌部가 各 各 1 例씩 이 었고 웹·에 서 發生한 惡{生鐵維{生 組織球廳은
大腦骨 2 例, 顆骨, 上觀骨 및 ¥¥推가 各各 l 例씩 이 었으
며 長骨에서 發生한 4 例중 3 例는 骨幹部블, 1 例는 骨 幹部 및 骨幹端홈ß를 同時에 홉犯하였 다 이 러한 發生홈ß 의 差異는 著者들의 tlE例가 적 기 때문인 것으로 思料된 다.
惡性繼維↑生組織球睡응 病理組織學的으로 매우 多樣한 所見을 보이 며 그 特徵的 所見은 옮越細 R엔의 와선행
(storiform) 配列과 組織細뼈의 增植이다. 肉眼的으로 도 多樣한 所見을 보여 회색에 서 총μ객, 암갈색무로 냐 타냐고 多樣한 軟性 및 固形性휩S分을 가지 며 睡塊內 壞 死가 흔히 同伴된마 5 , 8,11 , 1 시 著者들이 經驗한 12 例중
CT를 施行한
2
例에 서 도 壞死所見。 l 觀察되 었으며 手 術 및 病理組織學的으로 숲例에서 睡째內 성힐死가 !짧認 되었다.骨에 서 發生한 경우 單純X線짧影上 骨幹홈ß에 서 境界 가 不分明한 좀이 먹은 것 같은 吸收性 겁· 破懷 所見에 同伴된 骨被磁眼이 냐 破壞所見, 憐接軟組織£로 波及된 睡塊陰影等。l 주로 觀察된다1, 8 , 11,12,14, 15: 뀔’廳反應은 거의 일어 냐지 않으나 病的 骨折 또는 骨’生檢後 輕微하 게 냐타나기도 하며 軟組織에 서 發生한 평、↑生織維性組織 球睡이 骨을 홉犯하거 냐 轉移性 骨病따에 서 骨體反應이 보마 뎌 흔한 것으j료 보교되고 있 마8 , 14 , 16: 또 드물게 는 病變의 周£잃용ß에 骨硬化가 냐타냐거냐 睡塊內 얼룩 진 모양의 ;SliJ<化가 觀察되기도 하며 8-10 , 14 , 17-20: 骨肉 睡이 냐 織維肉睡에 比해 骨便塞이 드물지 않게 同伴된
마20 ,2 시 以上의 X 線振影所見은 餘他의 惡性骨睡場에서 觀察되는 所見과 類似하며 惡性織維性組織球睡파 籃別 흡?斷을 룡용하는 i*愚으로는 협’肉健, 織維肉睡,轉移性 授,
惡、性巨大細뼈鍾, 惡、性細網細뼈睡 等이 있냐 9 , 10 , 12 ,13). 著 者들의 경우 全例에서 吸收性의 骨 빛 骨被의破壞와骨 健反應所見에 同伴된 軟組織睡塊陰影이 觀察되었고 2 例에 서는 病的骨折도 있 었으나 ;SliJ<化의 所見은 觀察되 지 않았다.
99mTc-MDP 냐 67Ga-citrate 를 이용한 신티 그라피 는 惡性繼維性組織球睡의 f쫓犯部位, I憐援 軟組織으로의 波及程度 및 骨轉移 與否等을 正確히 흘?斷할 수 있어 治 爾에 도웅을 줄 수 있마 22 , 23~ 著者들의 경우 7 例에서
99mTc-MDP 骨신터그라피를 뼈行하여 軟組~睡塊內에 서 放射能의 骨路外 훌積所見 그러고 放射能 홉積의 減
少된 홈!’位와 增 JJQ된 좀ß位의 混슴펀 樣相을 홉犯된 骨에 서 觀察하였으며 이러한 骨內 放射能 홉積의 減少 部位 는 睡塊內 骨硬塞이나 壞死所見파 關聯된 것으혹 思料 된다. 또한 軟組織에서 發生한 경우에 憐援骨被의 放射 能 홉휩增J.m所見우로 骨被위 f훌犯與否을 보마 더 표確 히 評價할 수 있었다.
血管造影術은 手術計핸j 設定에 도움이 되 며 그 所見 으로는 睡場內 血流增加, 周圍血管의 轉移, 新生 血管의 形成等이 마 24 , 25:
惡性繼維性組織球睡은 睡塊除去後 頻緊히 再發하며 8,
9) 著者들의 경우에서도 軟組織1] 서 發生한 7 例중 6 例에서 手術的 除去後 陣塊가 再發하였다.
또한 惡性織維性組織球睡은 他肉睡들처럼 轉移가 흔 히 일어 냐며 이중 1M 뺑移가 가장 않고 그외 빼巴節, n千,
副뽑, 骨等에 轉移된다 6-9 , 11-16) 著者들의 경우 總 12 例중 빠 및 뀔’轉移를 보인 것이 各各 2 例였다.
惡性織維性組織球睡에 대 한 治爾는 化學據法, 手術的 除去 및 放射線治續等이 있고 대 마수 初期 該斷後
3
年 以內에 死亡하는 것으로 알려져 있£며 빠轉移에 의 한 合佛효이 死亡의 主훨因이 된다. 數後는 愚者의 年敵。l 나 睡傷의 病理學的 形願와는 無關한 것우로 報告되고。 l 仁1 5 , 8, 9 , 11 , 14) λλ
-,
VI.
結 論著者들은 最近
8
年間 앓i 熙大學校 附屬病院에 서 手術 및 病理組織學的으로 確양된 12 例의 節骨路系 惡性繼 維性組織球睡을 經驗하여 마읍과 같은 結論을 얻었다.1. 7 例는 軟組織에서, 5 例는 骨에서 發生하였다.
2. 男女比는 7:5 였고 40 歲 以後가 8 例호 대마수 를차지하였다.
3.
軟組織에 서 發生한 惡、性織維性組織球睡은 臨 ÞR的 으로 急成長하거 나 手術的 切除後 再發된 m휠塊 j료 觸ffi 되었다. 單純X 線짧影上 全例에서 軟組織睡塊陰影所見,骨신티그라파上 2 例에서 憐接骨皮의 흡潤이 觀察되었 다.
사~;~i':f.
n
김i.\f.I:織빠‘애 組織f.,J<ß핑에 對한 放Mífil장.;(J(J fofr 見-4 _ 骨에서 發生한 경우 全例에서 境界가 不分明한 吸收性 骨 및 骨被의 破壞所見, 骨願反應 및 同伴된 軟 組織睡塊陰影이 觀察되었다.
5_ 뼈轉移가 2 ØlJ
,
骨빼移가 2 例였다.6 _ 臨똥的으로 攻짧的 碩向의 睡塊가 있 거 냐 放射線 學的무로 惡性 睡場에 의한 非特異的 骨破壞 所見이 觀 察될 째에는 惡性織維性組織球睡의 可能性도 考慮해 보 아야 할 것으로 思料된다.
REFERENCES
1. Leonard BK, Bruce W , Elwin M et al: Malignant fibrous histiocytoma of bone. Cancer 42:640-651, 1958 2. Ozzello L, 5tout AP, Murray MR: Cultural characteristics
of malignant histiocytomas and fibrous xanthomas. Cancer 16:331-343, 1963
3. 0’Brien )E, 5tout AP: Malignant fibrous xanthomas. Cancer 17:1445-1455, 1964
4. Fu Y, Babbiani G, Kaye GI et al ι↑alignant 50ft tissue tumors of probable histiocytic origin (malignant fibrous histiocytoma). General considerations and electron microscopic and tissue cu/ture studies. Cancer 35: 176-198, 1975
5. Dahlin DC, Unni KK, Matsuno T ιfalignant fibrous histiocytoma of bone fact or fancy? Cance 39: 1508-1516, 1977
6. Kahn LB, Webber B, Mills E et al: Malignant fibrous histiαytoma (malignant fibrous xanthoma: xanthosarcoma) of bone. Cancer 42:640-650, 1978
7. Miller R, Kreutner A, Kurtz 5M: Malignant fibrous Histiocytoma (Inflammatory fibrous histiocytoma). Cancer 45:179-187, 1980
8. Feldman F, Norman D: Intra and extraosseous malignant histiocytoma (malignant fibrous xanthoma). Radiology 104:497-508, 1972
9. Weiss 5W, Enzinger FM: Malignant fibrous histiocytoma Cancer 41:2250-2266. 1978
10. 5panier 55, Enneking WF, Enriquex P: Primary malignant fibrous histiocytoma of bone. Cancer 36:2084-2098, 1975 11. 5panier 55: Malignant fibrous histiocytoma of bone: Orth
Clin N Amer 8:947-961, 1977
12. Huvos A: Primary malignant fibrous histiocytoma of bone Clinicopathologic study on 18 patients. NYj Med 76:552-559, 1976
13. McCarthy EF, Matsuno T, Dorfmman HD: Malignant fibrous histiocytoma of bone; A study on 35 cases. Human Path 10:57-70, .1979
14. 5pjut 비, Fechner RE, Ackerman LV: Tumors of bone and cartilage. 1st ed Washington D.C AFIP 띠scic/e κ 1981, P1 15 이운규, 이성로, 김대영 : 악성 섬유성 조직구종. 대
한방사선의학회지.
16. Kearney MM, 50ule EH, Lvins JC: Malignant fibrous histiocytoma: A retrospective study of 167 cases. Cancer 45:167-178, 1980
17. Bhagavan B5, Dorfman HD: The significance of bone and cartilage formation in malignant fibrous histiocytoma of 50ft tissue, Cancer 49:480-488, 1982
18. 5aito R, Caines MJ: Atypical fibrous histiocytoma of the humerus. Am j Clin Pathol 68:409-415, 1977
19. Dorfman HD, Bhagavan B5: Malignant fibrous histiocytoma of 50ft tissue with mètaplastic bone and cartilagenous for mation: A new radiologic sign: Skeletal radiolgy 8 145-150, 1982
20. Mirra JM, Bullough PG, Marcove RC et al: Malignant fibrous histiocytoma and osteosarcoma in association with bone infarcts. Report of four cases, two in caison workers. j Bone joint Surg 56A: 932-940, 1974
21. Dorfman HD, Norman A, Wolff H: Fibrosarcoma com plicating bone infarction in a caison worker. j Bone joint Surg 48A:528-532, 1966
22. Zazzaro PF, Bosworth JE, Zelenak
JJ:
Gallium Scann/y in ιfFH. AjR 135:775-779, 198023. Harrowe D), Kessler 5, Jansen AA: Gallium 67 uptake by a ι1FH case report. j Nuc/ ιfed 17:630-632, 1976 24. Hudson TM, Hawkins IF, 5panier 55 et al: Angiography of
malignant fibrous histiocytoma. Radiology 131:9-15, 1979 25. Pear BL: The histiocyte in radiology: With case reports of retroperitoneal xanthogranuloma and malignant fibrous xanthoma. Am j Roentgenolgy 110:159-165, 1979