Received: July 6, 2018 Revised: September 28, 2018 Accepted: October 1, 2018 Trauma and InJury
Correspondence to Sun Pyo Kim, M.D.
Department of Emergency Medicine, Chosun University Hospital, College of Medicine, Chosun University, 365 Pilmun-daero, Dong-gu, Gwangju 61453, Korea
Tel: +82-62-220-3285 Fax: +82-62-224-3501 E-mail: [email protected]
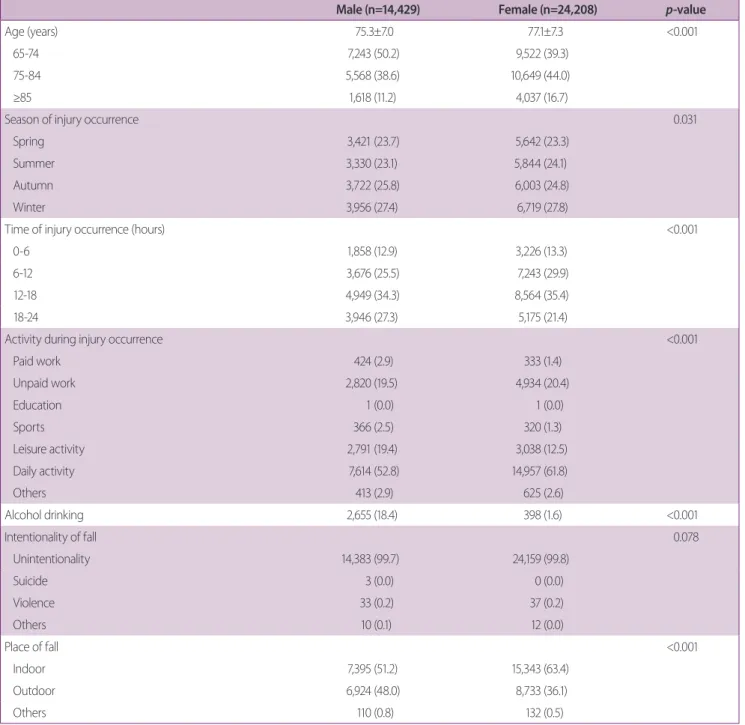
Epidemiological and Clinical
Characteristics of Elderly fall Patients Visit to the Emergency department:
a Comparison by Gender
Jun Kew Kim, M.D.
1, Sun Pyo Kim, M.D.
1, Sun Hyu Kim, M.D.
2,
Gyu Chong Cho, M.D.
3, Min Joung Kim, M.D.
4, Ji Sook Lee, M.D.
5, Chul Han, M.D.
61
Department of Emergency Medicine, Chosun University Hospital, College of Medicine, Chosun University, Gwangju, Korea
2
Department of Emergency Medicine, University of Ulsan College of Medicine, Ulsan, Korea
3
Department of Emergency Medicine, School of Medicine, Hallym University, Seoul, Korea
4
Department of Emergency Medicine, Yonsei University College of Medicine, Seoul, Korea
5
Department of Emergency Medicine, Ajou University School of Medicine, Suwon, Korea
6