536
Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright © 2010 The Korean Society of Cardiology CASE REPORT
DOI 10.4070 / kcj.2010.40.10.536
Open Access
Acute Myocardial Infarction by Right Coronary Artery Occlusion Presenting as Precordial ST Elevation on Electrocardiography
Sung Eun Kim, MD, Jun-Hee Lee, MD, Dae-Gyun Park, MD, Kyoo-Rok Han, MD and Dong-Jin Oh, MD
Division of Cardiology, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
ABSTRACT
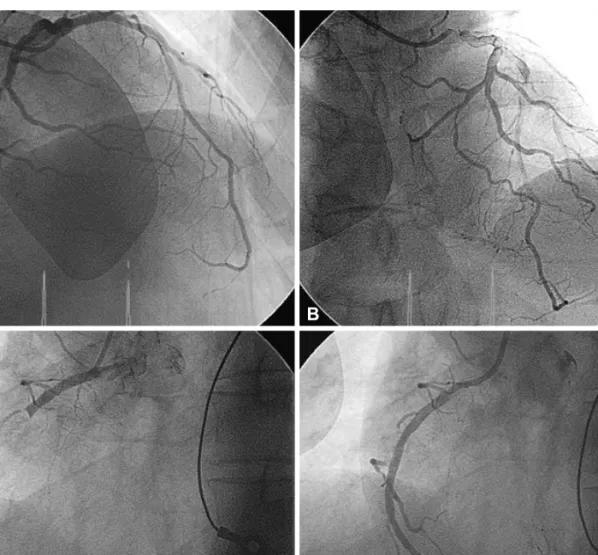
It is rare to observe ST-segment elevation in only the anterior leads and not the inferior leads during right coronary artery occlusion. We describe a case with acute myocardial infarction (MI) by right coronary artery occlusion who developed ST-seg- ment elevation only in the precordial leads V1 to V3. (Korean Circ J 2010;40:536-538)
KEY WORDS: Electrocardiography myocardial infarction.
Received: February 19, 2010 Accepted: March 26, 2010
Correspondence: Jun-Hee Lee, MD, Division of Cardiology, Depart- ment of Internal Medicine, Kangdong Sacred Heart Hospital, 445 Gil 1-dong, Gangdong-gu, Seoul 134-701, Korea
Tel: 82-2-2224-2405, Fax: 82-2-2225-2725 E-mail: [email protected]
cc