사회적 지지가 치매 수발 부담과 우울증에 미치는 영향
남 일 성
한림대학교 고령사회연구소
Effects of Social Support on Caregiver Burden and Depressive Symptoms in Family Caregivers of Patients with Alzheimer’s Disease
IlSung Nam
Hallym University Aging Institute, Chuncheon, Korea
Background: Alzheimer’s disease and other forms of dementia affect an ever-growing number of individuals in the United States, and the family members in charge of caring for relatives with dementia often experience de- bilitating caregiving burden and depression as a result of this responsibility.
Methods: Using a sample of 612 family caregivers from the Resources for Enhancing Alzheimer’s Caregiver Health, this study examined perceived social support (i.e., level of satisfaction with social support received) as a protective factor of caregiving burden and depression.
Results: Regression results indicated that there was a significant negative effect of perceived social support on caregiving burden (B=-0.35, P<0.01) and depressive symptoms (B=-0.55, P<0.01). Mediation analysis results indicated a significant indirect effect of perceived social support on depressive symptoms through caregiving burden (B=-0.103, CI=-0.207/-0.035).
Discussion: These findings indicate that higher perceived social support may reduce caregiving burden, and in turn, reduce depressive symptoms. These findings provide insight into the mechanisms linking social support with depressive symptoms among caregivers.
Korean J Health Promot 2013;13(4):156-163
Keywords: Social support, Depression, Family caregivers
■ Received:December 2, 2013 ■ Accepted:December 18, 2013
■ Corresponding author:IlSung Nam, PhD
Hallym University Aging Institute, 1 Hallimdaehak-gil, Chuncheon, 200-702, Korea
Tel: +82-33-248-3091 Fax: +82-33-248-3095 E-mail: [email protected]
INTRODUCTION
Due to the debilitating nature of dementia conditions, caregivers of a family member with Alzheimer’s disease or a related dementia (ADRD) can suffer significant stress and resulting psychological morbidity, including depressive symptoms. Research has largely documented that care- giving stress increases the level of depressive symptoms.1-4) These studies point to the importance of identifying pro-
tective factors that can reduce the level of depressive symptoms. Social support has been shown to be an im- portant buffer against the negative effects of caregiving burden and depressive symptoms.5-7) This study examined the longitudinal association between social support and caregiving burden and depressive symptoms.
It is estimated that more than 5.2 million Americans have ADRD, and the annual number of new cases of de- mentia is expected to double by 2050.8) Alzheimer’s dis- ease, which accounts for 60% to 80% of all dementia cases, is a debilitating condition characterized by early symp- toms, such as memory loss, apathy, and depression, as well as, later symptoms, such as impaired judgment, dis- orientation, confusion, and difficulty walking, swallow- ing, and speaking.8) Due in large part to the devastating na-
ture of these conditions, family members who take on sub- stantial caregiving responsibilities can suffer significant stress and resulting psychological morbidity.
An extensive body of research documents that the ad- verse effects of prolonged stress due to caring for an in- dividual with ADRD has been associated with increased psychological health risk. Psychologically, caregivers are at a greater risk for depression2-4) and anxiety.1) Recent re- search has also linked depression symptoms with an in- creased incidence or emergency department visits in ADRD caregivers.9) These findings paint a striking picture of increased morbidity associated with caring for a loved one with ADRD.
The constructs of social support and caregiving burden have been extensively defined and utilized in the literature.
Social support is generally considered in light of (a) struc- tural aspects of the support network, such as the breadth and composition of one’s social support network; (b) functional types of assistance available or received, or sup- port available versus actually received; and (c) the nature of social support received, often considered in light of sat- isfaction with or reciprocity of social support.10) Caregiving burden has been conceptualized in a number of ways, in- cluding problems with the caregiver’s health, psycho- logical well-being, finances, and social life related to the strain of caregiving responsibilities and roles11) and ap- praisal of distress associated with the tasks of caring for a family member with ADRD.12)
Family caregivers of older adults often experience sub- stantial strain, or caregiver burden, as a result of their role,13) and family caregivers of individuals with ADRD are no exception.12,14) In family caregivers of older adults who do not have ADRD, social support, both in terms of the breadth of one’s social support network and the amount and quality of social support received, are asso- ciated with perceived caregiver burden such that greater social support is associated with less perceived burden.15) Similar results have been found in family caregivers of in- dividuals with ADRD. A study of female caregivers found that difficulty arranging assistance with caregiving tasks was associated with greater caregiver burden5) while a study of family caregivers in Canada found that low in- formal social support was related to higher caregiver burden.16) ADRD family caregivers who have more con- tact with individuals in their social support system also ex-
perience lower caregiver burden than caregivers who have less frequent contact with their social support system.6,11)
Social support has been found to be beneficial in care- givers, specifically in terms of depressive symptoms.17) The caregiver literature indicates that caregivers reporting higher social support from relatives and friends demon- strate lower depressive symptom levels.18) For instance, Chang, Brecht, and Carter5) found that difficulty arrang- ing assistance with caregiving tasks was related to greater depression in female ADRD family caregivers, while Brummett, Siegler, Williams, and Dilworth-Anderson19) found that both baseline social support and change in so- cial support over time were related to depressive symp- toms such that when higher social support at baseline and increasing social support over time were related to fewer depression symptoms.
In addition, the literature indicates that there are two commonly addressed and distinct social support con- structs―perceived and received support―that are dis- tinguishable in their effects on mental health.15) Perceived social support refers an individual’s belief in the avail- ability of social support, and it is often measured using in- struments, such as the Interpersonal Support Evaluation List,20) that ask participants to make evaluations of the quality of availability of social support resources. Received social support refers to whether or not social support was actually received, and it is often measured using instru- ments that report the frequency at which support was received.20) Poor perceived social support is related to poorer mental health18) and higher burden.6) In terms of re- ceived support, ADRD caregivers who have more regular contact with individuals in their social support network have higher morale and lower levels of burden6,11) than caregivers who experience less frequent contact with their social support network. In a study of family caregivers, Li and colleagues17) examined the relationship between the different types of support–perceived and received–and de- pressive symptoms in family caregivers. They found that greater perceived emotional support buffered caregiving stress and that received support was not related to depres- sion in either wives or daughters. These findings indicate that different types of social support may be differentially related to depression. Accordingly, an examination of the effects of different social support constructs on caregiving burden and depressive symptoms is necessary.
Knowing that (1) caregiving burden increases the risk of having more depressive symptoms, and (2) caregivers with more social support may reduce caregiving burden and de- pressive symptoms, the present study attempted to link the two relationships. This study first examined the effects of the two social support constructs on caregiving burden and depressive symptoms. Second, this study tested the in- direct effects of the two social support constructs on de- pressive symptoms through caregiving burden.
METHODS
1. Participants and procedures
The study sample included 612 family caregivers from the Resources for Enhancing Alzheimer’s Caregiver Health (REACH) project. The primary purpose of the REACH study was to test the effectiveness of various psy- chological interventions for caregivers of older adults with Alzheimer’s disease on their caregiving challenges. The REACH study tested nine interventions at six sites. Sites were located in six cities near major universities in U.S.
(Miami, FL, Boston, MA, Memphis, TN, Birmingham, AL, Palo Alto, CA, and Philadelphia). All sites compared intervention conditions to control conditions using ran- dom assignment. Interventions varied across sites. Three sites compared one intervention to the control condition, and three sites compared two intervention conditions to the control condition (Skill training vs. Minimal support at Birmingham; Telephone-linked care vs. Usual care at Boston; Behavioral intervention + Information and re- ferral care vs. Enhanced care at Memphis; Family-based structural multisystems in-home + Computer telephone integration system vs. Minimal support at Miami; Coping with caregiving + Enhanced support group vs. Minimal support at Palo Alto; Environmental skill building vs.
Usual care at Philadelphia). A total of 1,222 caregiver and care recipient dyads were recruited from 1996 to 2000 at the six sites, and they were followed at 6, 12, and 18 months assessment intervals. The present study uses a sub- set of the REACH data to examine the effects of social support at baseline on caregiving burden at the 6-month follow-up and depressive symptoms at the 12-month fol- low-up. Out of the 1,222 caregivers, 954 were assessed at 12 months. Additionally, we excluded 201 caregivers who
experienced a loss of their care-recipient to death during the study and 141 caregivers whose care-recipients were placed in a long-term care facility. This resulted in a final analytic sample of 612 caregivers for whom data was col- lected at baseline and at the 12-month follow-up.
2. Measures
1) Depressive symptoms
Depressive symptoms were measured by the Center for Epidemiologic Studies Depression Scale (CESD),21) which is one of the most frequently used self-report instruments for depressive symptoms in caregiver research.2-4,7) This measure consists of 20 declarative statements regarding one’s depressive symptoms to which the frequency of symptoms in the past week are indicated on a 4-point Likert-type scale ranging from 0 (rarely or none of the time) to 3 (most or almost all the time). The questions tar- get symptoms experienced during the past week and cap- ture affective, somatic, well-being, and interpersonal domains.
Responses to items are summed to create an overall score ranging from 0 to 76.
2) Social support measures
Received social support was measured pre and post be- reavement using 11 items. Participants were asked to rate how often they received emotional support using 4 items (e.g., “In the past month, how often was someone right there with you [physically] in a stressful situation?”, “In the past month, how often has someone provided comfort to you?”), informational support using 4 items (“In the past month, how often has someone made a difficult sit- uation clearer and easier to understand?”, “In the past month, how often has someone helped you understand why you did not do something well?”), and tangible sup- port using 3 items (“In the past month, how often has someone, such as a friend, neighbor, or family member pro- vided transportation for you?”, “In the past month, how of- ten has someone helped you with shopping?”). Participants were asked to rate on a 4-point scale how often they received (emotional, informational, and tangible) support from a friend, neighbor, or family member (0=Never, 1=Once in a while, 2=Fairly often, 3=Very often). Total received support scores were computed by summing the three dimensions of support (e.g., emotional, informational, and tangible) at the
Figure 1. Perceived social support mediating model on the relationship between caregiving burden and depressive symptoms
CESD Score at 12 Month Follow-up Satisfaction With
Support at Baseline
Caregiving Burden At 6 Month Follow-up a
c
b 12-month follow-up.
3) Perceived social support
Respondents were then asked about their level of sat- isfaction with the amount of each type of support they re- ceived (e.g., “In the past month, how satisfied have you been with the support received during difficult times, how others have listened, and interest and concern from oth- ers?”, “How satisfied in the last month have you been with the suggestions, clarifications, and sharing of similar experi- ences you have received from others?”, “How satisfied have you been in the last month with the help you have re- ceived with transportation, housework, yard work, and shopping?”). Participants were asked to rate on a 4-point scale their current satisfaction with the social support that they have received (0=Not at all, 1=A little, 2=Moderately, and 3=Very). Total perceived support scores were calcu- lated by summing the three types of satisfaction with the social support (e.g., emotional, information, and tangible) at the 12-month follow-up.
4) Caregiving burden
Caregiving burden was measured by subjective evalua- tion of caregivers on caregiving challenges. The REACH study asked caregivers care-recipient functional status by using the Activities of Daily Living Scale seven items (e.g., bathing, dressing, etc.)22) and the Instrumental Activities of Daily Living Scale eight items (e.g., shopping, preparing meals, etc.).23) Respondents were then asked how much each caregiving activity bothered or upset the caregivers.
Participants were asked to rate this on a 5 point scale (0=Not at all, 1=A little, 2=Moderately, 3=Very much, 4=Extremely). Total caregiving scores were calculated by summing the 15 items of the ADL and IADL bothered scores at the 6-month follow-up.
5) Covariates
The REACH Intervention assignment was used as a di- chotomous variable. Those who were assigned to any of the nine REACH interventions were coded as “Yes” and those who were assigned to any control conditions were coded as “No.” Years of caregiving and hours per day spent caregiving were included in the analysis. Study par- ticipants’ age, gender, race, income, financial hardship, ed- ucation level, and the number of people live in the home
were also included in the analysis.
3. Data analysis
We examined several effects of the perceived social sup- port (Figure 1). (1) effect of perceived social support on caregiving burden (Path a), (2) effect of perceived social support on depressive symptoms (Path c), (3) effect of per- ceived social support and caregiving burden on depressive symptoms (Path b+c), and (4) indirect effect of perceived social support on depressive symptoms through care- giving burden. All three steps were repeated using the re- ceived social support in place of the perceived social support.
First, we performed a series of multiple regression anal- yses (Path a-c) using different dependent and main in- dependent variables (e.g., caregiving burden, depressive symptoms). Given the possibility that those with depres- sive symptoms (i.e., dependent variable) may exhibit a neg- ative bias on the subjective measure of social support or caregiving burden (i.e., independent variable), all the rela- tionships were longitudinally designed such that predictors should be measured prior to the time when predicted varia- bles were measured. Accordingly, the social support meas- ures at baseline, caregiving burden at 6-month follow-up, and the CESD total scores at 12-month follow-up were used in the analysis. The estimations of the three direct effects were repeated with the two types of social support constructs.
Second, we estimated an indirect effect of social support on depressive symptoms through caregiving burden. We performed a Sobel-Goodman mediation test using STATA plug-in program sgmediation. Estimation was bootstrapped
Table 1. Demographic characteristics of caregivers (n=612)
Characteristics Mean (SD) or %
CESD total score at 12 month 11.61 (9.26) Caregiving burden at 6 month 3.46 (6.79) Sex
Male 17.32
Female 82.68
Relationship to care-recipient
Spouse 47.22
Not spouse 52.78
Age, y 61.33 (13.38)
Caregiver’s race
White 52.54
Black 27.17
Hispanic 20.29
Household income, US Dollar
<20,000 34.28
20,000-39,000 35.44
>40,000 30.28
Financial status
Difficult 27.44
Not difficult 72.56
Education level
Did not complete high school 17.32
High school graduate 57.68
College graduate 25.00
Number of people living in the home 1.98 (1.34) REACH Intervention participation
Yes 74.84
No 25.16
Hours per day spent for caregiving 12.08 (7.16) Years of caregiving for care recipient 4.26 (4.19) Abbreviations: CESD, Center for Epidemiologic Studies Depression Scale; REACH, Resources for Enhancing Alzheimer’s Caregiver Health.
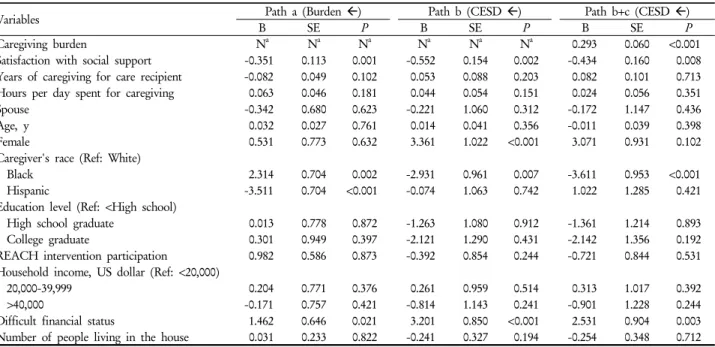
Table 2. Regression results predicting CESD at 12 month follow-up and caregiving burden at 6 month follow-upa
Variables Path a (Burden Å) Path b (CESD Å) Path b+c (CESD Å)
B SE P B SE P B SE P
Caregiving burden Na Na Na Na Na Na 0.293 0.060 <0.001
Satisfaction with social support -0.351 0.113 0.001 -0.552 0.154 0.002 -0.434 0.160 0.008 Years of caregiving for care recipient -0.082 0.049 0.102 0.053 0.088 0.203 0.082 0.101 0.713
Hours per day spent for caregiving 0.063 0.046 0.181 0.044 0.054 0.151 0.024 0.056 0.351
Spouse -0.342 0.680 0.623 -0.221 1.060 0.312 -0.172 1.147 0.436
Age, y 0.032 0.027 0.761 0.014 0.041 0.356 -0.011 0.039 0.398
Female 0.531 0.773 0.632 3.361 1.022 <0.001 3.071 0.931 0.102
Caregiver's race (Ref: White)
Black 2.314 0.704 0.002 -2.931 0.961 0.007 -3.611 0.953 <0.001
Hispanic -3.511 0.704 <0.001 -0.074 1.063 0.742 1.022 1.285 0.421
Education level (Ref: <High school)
High school graduate 0.013 0.778 0.872 -1.263 1.080 0.912 -1.361 1.214 0.893
College graduate 0.301 0.949 0.397 -2.121 1.290 0.431 -2.142 1.356 0.192
REACH intervention participation 0.982 0.586 0.873 -0.392 0.854 0.244 -0.721 0.844 0.531 Household income, US dollar (Ref: <20,000)
20,000-39,999 0.204 0.771 0.376 0.261 0.959 0.514 0.313 1.017 0.392
>40,000 -0.171 0.757 0.421 -0.814 1.143 0.241 -0.901 1.228 0.244
Difficult financial status 1.462 0.646 0.021 3.201 0.850 <0.001 2.531 0.904 0.003
Number of people living in the house 0.031 0.233 0.822 -0.241 0.327 0.194 -0.254 0.348 0.712 Abbreviations: CESD, Center for Epidemiologic Studies Depression Scale; REACH, Resources for Enhancing Alzheimer’s Caregiver Health.
aAssessed by multiple regression analyses.
with 1,000 replications. We reported the coefficient and upper and lower confidence intervals of the indirect effect estimation. If the intervals do not contain 0, this indicates that the coefficient of the indirect effect is significant.
RESULTS
1. Demographic information (Table 1)
Demographic information on the 612 caregivers is pro- vided (Table 1). Participants were predominantly female and white. The average age was 61.3 years (SD=13.38, range=28–89). The average number of hours caring for care recipient per day was 12.08 (SD=7.16, range=0–24), and the average number of years spent caregiving was 4.26 (SD=4.19, range=0-40). Nearly half (47.22%) of the care- givers in our analytic sample were spouse caregivers while an additional 52.78% were non-spouse caregivers, includ- ing children, other relatives, and friends.
2. Effects of social support on caregiving burden (Path a)
There was a significant effect of satisfaction with social support on caregiving burden such that caregivers report- ing higher satisfaction with social support are less likely to have higher caregiving burden scores (B=-0.351, P<0.01).
Table 3. Indirect effect of satisfaction with social support at baseline on CESD at 12m through satisfaction with support at 6-month follow-upa
Observed coefficient Bias Bootstrap SE 95% CI (L/U)
Percentile CI Bias-corrected CI
Indirect effect -0.103 -0.003 0.043 -0.204 -0.033 -0.207 -0.035
Direct effect -0.469 -0.006 0.165 -0.806 -0.138 -0.818 -0.153
Abbreviations: CESD, Center for Epidemiologic Studies Depression Scale; SE, standard error; CI, confidence interval; L, lower; U, upper.
aAssessed by Sobel-Goodman mediation test. Standard error was bootstrapped with 1,000 replications.
Black caregivers were more likely to demonstrate higher caregiving burden than white caregivers (B=2.314, P<0.01), whereas Hispanic caregivers were less likely to have higher caregiving burden scores than white caregivers (B=-3.511, P<0.001). Additionally, caregivers reporting financial hard- ship were more likely to have higher caregiving burden levels (B=1.462, P<0.05). However, there was no significant effect of received social support on caregiving burden (Table 2).
3. Effects of social support on CESD total score (Path c)
There was a significant effect of satisfaction with social support on depressive symptom levels such that caregivers reporting more satisfaction with social support were less likely to present higher level of depressive symptom scores (B=-0.55, P<0.01). Black and male caregivers reported statistically higher depressive symptom levels than white and female caregivers. Additionally, caregivers reporting financial hardship showed higher levels of depressive symp- toms than caregivers without financial hardship (B=3.20, P<0.001). However, there was no significant effect of received social support on depressive symptom level (Table 2).
4. Effects of social support and caregiving burden on CESD total score (Path b+c)
Caregivers reporting higher burden showed higher levels of depressive symptom (B=0.29, P<0.001). Consistent with the results above, black and male caregivers reported statisti- cally higher depressive symptom levels than white and fe- male caregivers (Table 2). Additionally, caregivers reporting financial hardship showed higher levels of depressive symp- toms than caregivers without financial hardship (B=2.53, P<0.01). However, there was no significant effect of received social support on depressive symptom levels (Table 2).
5. Effects of social support on CESD total score through caregiving burden
Having found that satisfaction with social support sig- nificantly predicted caregiving burden, and caregiving burden significantly predicted depressive symptom levels, we tested an indirect effect of satisfaction with social sup- port on depressive symptoms level through caregiving burden (see Table 3). The results showed that there was a significant indirect effect (B=-0.103, CI=-0.207/-0.035).
DISCUSSION
Dementia caregiving is a challenging responsibility that can lead to negative psychological outcomes. While social support is increasingly becoming a focus of attention, little is known about its effect on caregiving burden and psycho- logical outcomes. Using regression and mediation analysis, the current study found a longitudinally significant effect of satisfaction with social support on caregiving burden and depressive symptom level such that caregivers report- ing higher satisfaction with social support demonstrated lower levels of caregiving burden and depressive symptom.
This finding supports previous studies6,11,16-19) and extends this work in two ways by: (1) using multiple measures of social support including perceived social support and re- ceived support and (2) assessing the indirect effect of sup- port on depressive symptoms through caregiving burden.
We found that less perceived social support was asso- ciated with a higher level of depressive symptoms. This finding supports recent studies reporting that only helpful support improves psychological outcomes.17,19) Interestingly, no significant association was found between received sup- port and depressive symptoms. Because the constructs of received support may include helpful, as well as, unhelpful support, it is possible that support from a family member or friend may lead to poor outcomes if the received sup-
ports are not deemed satisfactory. This finding suggests that received social support may be less critical in predict- ing depressive symptom among dementia caregivers.
This study also found that perceived support decreased the level of caregiving burden, which is consistent with previous findings.6,16) Further, we found that the decreased caregiving burden by perceived support decreased the lev- el of depressive symptom. Provision of helpful support might serve as effective points of intervention by reducing caregiving burden, in turn reducing depressive symptoms.
Likewise, no significant indirect effect was also found with the received support. In 2012, approximately 9.18% of de- mentia patients were estimated to be living in Korea.24) Many of these dementia patients are being cared for by a family member. There are programs that aim to provide support to caregivers caring for their family members with dementia. Examples of these programs include commun- ity-based respite program,25) cognitive-behavioral intervention program,26) and group psycho-education program.27) Programs such as these need to consider the most effective ways of providing support for these caregivers. Family caregivers who receive support through these programs need to feel satisfied with the supportive services received. One way to enhance the quality of support provided by these pro- grams is to educate clinicians and social workers on the best and most effective practices. Although this study has important implications for the direct and indirect effects of perceived support on depressive symptom, it is limited in that the source of social support could not be examined.
For instance, we did not know where the support care- givers received originated from―relatives or friends. It is also unclear whether received support and satisfaction with support were derived from the same source. To broaden the findings of this study, future studies should distinguish source of support.
Notwithstanding these limitations, these findings pro- vide important insights into the relationship between so- cial support and depressive symptoms, which will likely enhance our understanding of mental health among caregivers. The effects of satisfaction with social support on the level of depressive symptoms shed new light on mechanisms linking social support with depressive symptoms. Understanding the multifaceted relationships between social support and depressive symptoms is crit- ical to provide appropriate social support to caregivers at
this challenging time.
요 약
배경: 치매 환자가 점점 늘어남에 따라 가족들이 겪는 치매 수발 부담이 우울증을 유발시키는 원인으로 파악되 면서 사회적 관심의 대상이 되고 있다. 본 연구는 사회적 지지가 치매 수발 부담과 우울증에 어떻게 영향을 미치는
지 기초적인 메커니즘을 규명하는 데 목적을 두고 있다.
방법: 미국에서 실시된 치매 수발 가족들을 대상으로 한 사회심리프로그램(Resources for Enhancing Alzheimer’s Caregiver Health)에 참가한 612명의 치매 수발 가족들을
분석했다. 사회적 지지가 치매 수발 부담을 낮추고, 사회적
지지에 의해 낮춰진 치매 수발 부담이 우울증을 낮추는지 를 검증했다.
결과: 연구 결과는 연구 가설을 지지하는 것으로 나타났 다. 사회적 지지가 수발 부담을 낮추고 사회적 지지에 의 해 낮아진 수발 부담이 우울증을 낮췄다.
고찰: 본 연구 결과는 치매 수발 가족들의 사회적 지지 와 우울증이 어떻게 관련이 있는지에 관한 기본적인 메커 니즘을 검증한 것으로, 치매 수발의 맥락에서 사회적 지지 와 우울증이 어떻게 관련이 되어있는지에 관한 기초 연구
틀로서 사용될 수 있을 것이다.
중심단어: 사회적 지지, 우울증, 치매 수발 부담
REFERENCES
1. Cooper C, Balamurali TB, Livingston G. A systematic review of the prevalence and covariates of anxiety in caregivers of people with dementia. Int Psychogeriatr 2007;19(2):175-95.
2. Covinsky KE, Newcomer R, Fox P, Wood J, Sands L, Dane K, et al. Patient and caregiver characteristics associated with de- pression in caregivers of patients with dementia. J Gen Intern Med 2003;18(12):1006-14.
3. Neundorfer MM, McClendon MJ, Smyth KA, Strauss ME, McCallum TJ. Does depression prior to caregiving increase vul- nerability to depressive symptoms among caregivers of persons with Alzheimer's disease? Aging Ment Health 2005;10(6):
606-615.
4. Schulz R, Belle SH, Czaja SJ, McGinnis KA, Stevens A, Zhang S. Long-term care placement of dementia patients and caregiver health and well-being. JAMA 2004;292(8):961-7.
5. Chang BL, Brecht M, Carter PA. Predictors of Social Support and Caregiver Outcomes. Women Health 2001;33(1-2):39-61.
6. Chiou CJ, Chang HY, Chen IP, Wang HH. Social support and caregiving circumstances as predictors of caregiver burden in Taiwan. Arch Gerontol Geriatr 2009;48(3):419-424.
7. Clyburn LD, Stones MJ, Hadjistavropoulos T, Tuokko H.
Predicting caregiver burden and depression in Alzheimer's disease. J Gerontol B Psychol sci soc sci 2000;55(1):S2-S13.
8. Thies W, Bleiler L; Alzheimer's Association. 2013 Alzheimer's
disease facts and figures. Alzheimers Dement 2013;9(2):208-45.
9. Schubert CC, Boustani M, Callahan CM, Perkins AJ, Hui S, Hendrie HC. Acute Care Utilization by Dementia Caregivers Within Urban Primary Care Practices. J Gen Intern Med 2008;
23(11):1736-40.
10. Cohen S. Psychosocial models of the role of social support in the etiology of physical disease. Health Psychol 1988;7(3):269-97.
11. Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980;
20(6):649-55.
12. Vitaliano PP, Russo J, Young HM, Becker J, Maiuro RD. The screen for caregiver burden. Gerontologist 1991;31(1):76-83.
13. Pearlin LI, Mullan JT, Semple SJ, Skaff MM. Caregiving and the stress process: An overview of concepts and their measures.
Gerontologist 1990;30(5):583-94.
14. Mioshi E, Foxe D, Leslie F, Savage S, Hsieh S, Miller L, et al. The impact of dementia severity on caregiver burden in fronto- temporal dementia and Alzheimer disease. Alzheimer Dis Assoc Disord 2013;27(1):68-73.
15. Vrabec NJ. Literature review of social support and caregiver burden, 1980 to 1995. Image J Nurs Sch 1997;29(4):383-8.
16. Clyburn LD, Stones MJ, Hadjistavropoulos T, Tuokko H.
Predicting caregiver burden and depression in Alzheimer's disease. J Gerontol B Sci Soc Sci 2000;55(1):S2-S13.
17. Li LW, Seltzer MM, Greenberg JS. Social support and depres- sive symptoms: differential patterns in wife and daughter caregivers. J Gerontol B Sci Soc Sci 1997;52(4):S200-11.
18. George LK, Gwyther LP. Caregiver well-being: a multidimen- sional examination of family caregivers of demented adults.
Gerontologist 1986;26(3):253-9.
19. Brummett BH, Siegler IC, Williams RB, Hilliard TS, Dilworth- Anderson P. Associations of Social Support and 8-Year Follow-
Up Depressive Symptoms: Differences in African American and White Caregivers. Clin Gerontol 2012;35(4): 289-302.
20. Cohen S, Hoberman H. Positive events and social supports as buffers of life change stress. J Appl Soc Psychol 1983;13(2):
99-125.
21. Radloff L. The CES-D Scale: A self-report depression scale for research in the general population. Appl Psychol Meas 1977;1:
385-401.
22. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW.
Studies of illness in aged. The index of ADL: a standard measure of biological and psychological function. JAMA 1963;185:
914-9.
23. Lawton MP, Brody EM. Assessment of older people: Self-main- taining and Instrumental Activities of Daily Living. Gerontologist 1969;9(3):179-86.
24. Ministry of Health and Welfare. Ministry of Health and Welfare: prevalence of dementia. Ministry of Health and Welfare;
2012. [Accessed December 30, 2013]. http://download.mw.go.
kr/f ront_new/ modul es / downl oad. j s p?BOARD_
ID=140&CONT_SEQ=286138&FILE_SEQ=134004.
25. Chun SH, Chang SO, Kong GS, Song MR. Development and evaluation of community-based respite program for family caregivers of elder with dementia. J Korean Acad Fundam Nurs 2011;18(3):337-47.
26. Kim SY, Kim JW, Sohn SK, Min SY. The effectiveness of the group education program among the family caregivers of the de- mented elderly. Korean J Res Geron 2007;36:7-34.
27. Lee EH, Kim SH, Youn G. Effects of a cognitive-behavioral in- tervention program on reduction of care burden for the care- givers of the demented elderly patients. Korean J Res Geron 2004;13:23-36.