53
Multicenter Clinical Outcome of Gatifloxacin for Chronic Prostatitis (NIH Category II or IIIa) in Korea
Sang Don Lee1,2, Seung Ju Lee2,3, Tae Kon Hwang4, Duck Ki Yoon5, Kyu Sung Lee6, Luck Hee Sung7, Myung Soo Choo8, Bong Suk Shim2,9,
In Rae Cho2,10, Min Eui Kim2,11, Soo Bang Ryu12, Chul Sung Kim2,13, Young Gon Kim14, Chun Il Kim15, Hyun Yul Rhew16, Yong-Hyun Cho2,17
From the Department of Urology, 1Pusan National University Hospital,
2Korean Association of Urogenital Tract Infection and Inflammation, 3Daniel Urolgy Clinic,
4Kangnam St. Mary's Hospital, The Catholic University of Korea, 5Guro Hospital, Korea University,
6Samsung Medical Center, Sunkyunkwan University, 7Sanggye Paik Hospital, Inje University,
8Asan Medical Center, Ulsan University, 9Dongdaemun Hospital, Ewha Womans University,
10Ilsan Paik Hospital, Inje University, 11Bucheon Hospital, Soonchunhyang University,
12Chonnam National University Hospital, 13Chosun University Hospital, 14Chonbuk National University Hospital,
15Dongsan Medical Center, Keimyung university, 16Kosin Medical Center, Kosin university,
17St. Mary's Hospital, The Catholic University of Korea, Korea
[Abstract]
Purpose: The objective of this study was to investigate the efficacy and safety of gatifloxacin for patients
with chronic prostatitis (NIH category II or IIIa) in Korean urologic practice.
Materials and Methods: A total of 16 outpatient urology clinics at tertiary care medical centers in Korea
participated. Gatifloxacin (400 mg/day) treatment (S.D.) of 149 patients (20 patients with category II and 129 patients with category IIIa) with prostatitis (mean age 45.8±13.3 years) was carried out for 41.7 (33.1) days.
A 4-glass test according to Meares and Stamey or two glass test was carried out at study entry and one month after the end of treatment. Clinical response, safety and bacteriological response were assessed before treatment (within 48 hours of initiation of the study medication) and at one month after treatment completion.
Results: In a otal of 149 patients, the total NIH-CPSI score was significantly reduced from 20.5 to 10.0 (response rate 86.7%; 95% CI 80.2-93.2%) (p<0.05). Sub-scores of pain, urinary symptoms and impact on the quality of life were also significantly reduced from 8.9 to 3.8 (response rate 83.8%; 95% CI 76.8-90.9%), from 4.2 to 2.0 (response rate 73.3%; 95% CI 64.9-81.8%) and from 7.4 to 4.2 (response rate 79.0%; 95% CI 71.3-86.8%), respectively (p<0.05). In terms of the overall clinical efficacy assessment by investigators, out of 149 patients with prostatitis, 71.2% were assessed to be responders. Bacteriological
•Corresponding author:Yong-Hyun Cho, Dept. Urology, St. Mary’s Hospital, Catholic University,
62 Yeouido-dong, Yeongdeungpo-gu, Seoul, 150-713, South Korea
Tel: 02-3779-1024, Fax: 02-761-1626 E-mail: [email protected]
studies in expressed prostatic secretion (EPS) or post prostate massage urine (VB3) at 1 month after treatment completion demonstrated that the overall eradication rates of pathogens was 85% and the pyuria (≥10 WBC/HPF) rates in the NIH category II and IIIa were 35% and 18.6%, respectively (overall rate 20.8%). There were 16.1% of patients that presented with some adverse events considered by investigators to be related to the drug. The majority of adverse events were considered to be of mild (87.5%) or moderate (8.3%) intensity.
Conclusions: These results suggest that gatifloxacin in Korean urologic practice is well tolerated and improves the clinical outcomes in the patientswith chronic prostatitis (NIH category II or IIIa). (Korean J UTII 2007;2:53-60)
Key Words: Gatifloxacin, Efficacy, Satety, Prostatitis
INTRODUCTION
Urinary tract infections (UTIs) are among the most common types of infectious diseases in medical prac- tice and present a major problem in terms of utiliza- tion of health care resources.
1Patients with chronic prostatitis have felt a considerable discomfort and in- convenience. Even though there is a very low rate of infection in males with a prevalence of <1%, as many as 50% of men at some point in their life, are affected by prostatitis; about 25% of visits to physi- cians for male genitourinary tract complaints are attributed to one of the prostatitis syndromes.
2,3Among urogenital infections, chronic prostatitis is a common disease in urologic practice. Antibiotics have been usually prescribed to treat thisinfection/infla- mmation. Gatifloxacin is recently developed fluoroqui- nolone with a broad spectrum of antibacterial activity against Gram-positive and -negative bacteria as well as anaerobes. This drug also has activity against Myco-
plasma and Chlamydia spp..4,5Tolerability and safety profiles of new agents are initially identified during preclinical and clinical development and are generally correlated with post marketing experience. However, rare adverse events are often not recognized until more experience is collected with extensive use in a large number of patients and centers. This study was de- signed to investigate the efficacy and safety of gati-
floxacin for the patients with chronic prostatitis (NIH category II or IIIa) in Korean urologic practice.
PATIENTS AND METHODS
The entry criteria for this study included men 20 years of age or older with clinical evidence of prostatitis (NIH category II or IIIa) and no evidence of structural or functional lower genitourinary tract abnormalities. Patients with a history of antibiotic use within 14 days before study enrollment were excluded.
In all men a 4-glass test according to Meares and Stamey
6was carried out and samples of first voided urine (VB1), midstream urine (VB2), expressed pro- static secretion (EPS) and post prostate massage urine (VB3) wereobtained at study entry and one month after the end of treatment. Category II prostatitis was defined as a colony count of at least 10
4/ml pathogens in EPS or, in patients in whom EPS could not be obtained, in VB3 samples and a colony counts in VB1 and VB2 at least 10 times lower than in EPS or VB3.
A category IIIa prostatitis was defined in patients with negative cultures for uropathogenic bacteria in EPS or VB3, and where colony counts in EPS or VB3were tenfold or greater than in VB1 and VB2. We obtained approval for the study from the Institutional Review Board of each of the 16 participating centers in Korea.
All patients provided written informed consent before
enrollment in this study. The safety and efficacy of gatifloxacin in 149 patients with chronic prostatitis treated in 16 outpatient urology clinic at tertiary care medical centers in Korea were evaluated. Patients were treated with gatifloxacin, 400mg daily, for 1-8 weeks, depending on the clinical response and side effect of drug. Clinical response, safety and bacteriological res- ponse were assessed before treatment (within 48 hours of initiation of the study medication) and at one month after treatment completion.
Clinical outcomes were measured by symptom scores using a questionnaire. The clinical symptoms of prostatitis were assessed by the NIH-CPSI total and sub-scores
7at baseline and one month after the end of treatment. A positive response was defined as a more than 25% reduction of NIH-CPSI scores at one month after the end of treatment compared to baseline scores.
The overall efficacy assessment by investigator was classified as responder (cure or improvement), non- responder (persistence or aggravation) and undeter- mined. A responder was defined when all pretreatment signs and symptoms of infection/inflammation resolved or improved without the need for additional antimicro- bial therapy and no new signs or symptoms of infec- tion/inflammation. A non-responder was defined when pretreatment signs or symptoms of infection/inflamma- tion persisted or were aggravated. Bacteriological out- come in patients with category II prostatitis was classi- fied by EPS or VB3 after treatment completion as
‘eradication (<10
4CFU/ml of initial pathogen)’, ‘per- sistence (≥10
4CFU/ml of initial pathogen)’, ‘reinfec- tion (replaced by ≥10
4CFU/ml of a different patho- gen)’ and ‘relapse (reinfection with the same pathogen with at least 10
4CFU/ml)’. All patients who received at least one dose of medication were included in the safety analysis. The severity of clinical adverse events was categorized by the investigators as mild, moderate, or severe.
Statistical analysis was performed using Student’s t-test for comparisons between two groups and a
probability level of <0.05 was required for statistical significance. The exact binomial method recommended by Farrington and Manning
8was used to compute the 95% confidence intervals for the response rates of gatifloxacin on prostatitis.
RESULTS
The overall average treatment duration (S.D.) (range) of 149 patients with prostatitis (mean age 45.8±13.3 years, range 28-67 years) was 41.7 days (33.1) (7-56).
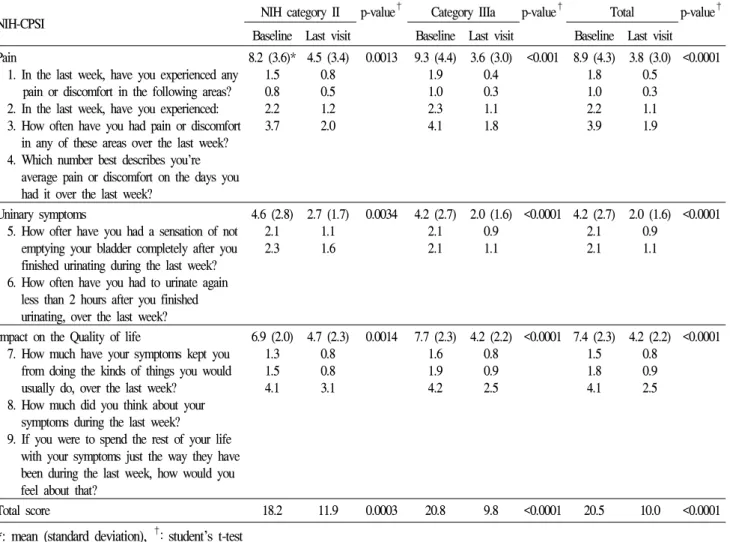
Average treatment duration (S.D.) (range) of NIH cate- gory II (mean age 48.6±8.5 years, range 34-64 years) and IIIa patients (mean age 42.5±11.5 years, range 28-67 years) were 45.6 days (32.7) (21-56) and 37.7 days (26.9) (7-56), respectively. The NIH-CPSI score before (baseline) and after (last visit) treatment is shown in table 1. In all 149 patients, the total NIH- CPSI score was reduced from 20.5 to 10.0 (response rate 86.7% 95% CI 80.2-93.2%; p<0.0001, Fig. 1) and the sub-scores of pain, urinary symptoms and impact on the quality of life were also improved from 8.9 to 3.8 (response rate 83.8%; 95% CI 76.8-90.9% p<
0.0001), from 4.2 to 2.0 (response rate 73.3%; 95% CI 64.9-81.8% p<0.0001), and from 7.4 to 4.2 (response rate 79.0%; 95% CI 71.3-86.8% p<0.0001), respecti- vely. In the NIH category II and IIIa, the total NIH- CPSI score were reduced from 18.2 to 11.9 (response rate 70.6%; 95% CI 48.9-92.2%; p=0.0003) and from 20.8 to 9.8 (response rate 89.8%; 95% CI 83.4-96.1%;
p<0.0001), respectively (Fig. 1). Sub-scores of pain, urinary symptoms, and impact on the quality of life for the NIH category II were also improved, scores changed from 8.2 to 4.5 (response rate 76.5%; 95% CI 56.3-96.6% p=0.0013), from 4.6 to 2.7 (response rate 52.9%; 95% CI 29.2-76.7% p=0.0034) and from 6.9 to 4.7 (response rate 64.7%; 95% CI 42.0-87.4% p=
0.0014). Sub-scores of pain, urinary symptoms and
impact on the qualityof life in the NIH category IIIa
were also improved, scores changed from 9.3 to 3.6
Fig. 1. NIH-CPSI total and sub-scores at baseline and last visit (one month after treatment completion). Total NIH-CPSI score in 149 patients was improved from 20.5 to 10.0 (†: response rate 86.7% 95% CI 80.2-93.2%; p<0.0001). Additionally, in 20 patients with NIH-category II and 129 patients with category IIIa, the total NIH-CPSI score was reduced from 18.2 to 11.9 (*: response rate 70.6%; 95% CI 48.9-92.2%;
p=0.0003) and from 20.8 to 9.8 (**: response rate 89.8%; 95% CI 83.4-96.1%; p<0.0001), respectively.
Table 1. NIH-CPSI score for chronic prostatitis (NIH category II and IIIa)
NIH-CPSI NIH category II p-value† Category IIIa p-value† Total p-value†
Baseline Last visit Baseline Last visit Baseline Last visit Pain
1. In the last week, have you experienced any pain or discomfort in the following areas?
2. In the last week, have you experienced:
3. How often have you had pain or discomfort in any of these areas over the last week?
4. Which number best describes you're average pain or discomfort on the days you had it over the last week?
8.2 (3.6)*
1.5 0.8 2.2 3.7
4.5 (3.4) 0.8 0.5 1.2 2.0
0.0013 9.3 (4.4) 1.9 1.0 2.3 4.1
3.6 (3.0) 0.4 0.3 1.1 1.8
<0.001 8.9 (4.3) 1.8 1.0 2.2 3.9
3.8 (3.0) 0.5 0.3 1.1 1.9
<0.0001
Uninary symptoms
5. How ofter have you had a sensation of not emptying your bladder completely after you finished urinating during the last week?
6. How often have you had to urinate again less than 2 hours after you finished urinating, over the last week?
4.6 (2.8) 2.1 2.3
2.7 (1.7) 1.1 1.6
0.0034 4.2 (2.7) 2.1 2.1
2.0 (1.6) 0.9 1.1
<0.0001 4.2 (2.7) 2.1 2.1
2.0 (1.6) 0.9 1.1
<0.0001
Impact on the Quality of life
7. How much have your symptoms kept you from doing the kinds of things you would usually do, over the last week?
8. How much did you think about your symptoms during the last week?
9. If you were to spend the rest of your life with your symptoms just the way they have been during the last week, how would you feel about that?
6.9 (2.0) 1.3 1.5 4.1
4.7 (2.3) 0.8 0.8 3.1
0.0014 7.7 (2.3) 1.6 1.9 4.2
4.2 (2.2) 0.8 0.9 2.5
<0.0001 7.4 (2.3) 1.5 1.8 4.1
4.2 (2.2) 0.8 0.9 2.5
<0.0001
Total score 18.2 11.9 0.0003 20.8 9.8 <0.0001 20.5 10.0 <0.0001
*: mean (standard deviation),
†:student’s t-test
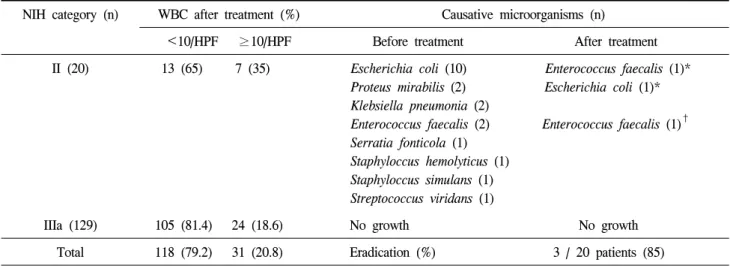
Table 2. Microbiological results before and at one month after treatment
NIH category (n) WBC after treatment (%) Causative microorganisms (n)
<10/HPF ≥10/HPF Before treatment After treatment II (20) 13 (65) 7 (35) Escherichia coli (10) Enterococcus faecalis (1)*
Proteus mirabilis (2) Escherichia coli (1)*
Klebsiella pneumonia (2)
Enterococcus faecalis (2) Enterococcus faecalis (1)† Serratia fonticola (1)
Staphyloccus hemolyticus (1) Staphyloccus simulans (1) Streptococcus viridans (1)
IIIa (129) 105 (81.4) 24 (18.6) No growth No growth Total 118 (79.2) 31 (20.8) Eradication (%) 3 / 20 patients (85)
*: eradication with reinfection, †: persistence
Table 3. Adverse events and severity related to the treatment
Adverse events No. patients (%) Intensity No. patients (%)
Nause/vomiting Headache Diarrhea Dizziness Abdominal pain*
10 (6.7) 5 (3.4) 4 (2.7) 3 (2.0) 2 (1.3)
Mild Moderate
Severe
21 (87.5) 2 (8.3) 1 (4.2)
Total 24 (16.1) 24 (100)
*: one patient withdrew medication due to drug-related gastric distress
(response rate 85.2%; 95% CI 77.8-92.6% p<0.0001), from 4.2 to 2.0 (response rate 77.3%; 95% CI 68.5- 6.0% p<0.0001), and from 7.7 to 4.2 (response rate 81.8%; 95% CI 73.8-89.9% p<0.0001). The overall clinical efficacy assessment by investigators showed that out of 149 patients, responders, non-responders and undetermined categories accounted for 71.2%, 13.4% and 15.4% of patients, respectively. For the NIH category II and IIIa, responders accounted for 50.0% and 74.4%, non-responder 30.0% and 10.9%, and undetermined 20.0% and 14.7% of patients, respectively. Bacteriological response in EPS or VB3 at one month after treatment completion is shown in table 2. The most common causative uropathogen identified in the NIH category II prostatitis was
Escherichia coli (50.0%). The overall eradication
rates of pathogens was 85%, and the pyuria (≥10 WBC/HPF) rates for the NIH category II and IIIawere 35% and 18.6%, respectively (overall rate 20.8%).
Twenty-four out of 149 patients (16.1%) reported some adverse events considered by investigators to be related to the experimental drug. The most frequent reported adverse events were nausea/vomiting (6.7%), headache (3.4%) and diarrhea (2.7%). Only one patient (0.7%) who presented with abdominal pain withdrew medication due to treatment-related gastric distress.
The majority of adverse events were considered to
be of mild (87.5%) or moderate (8.3%) intensity
(Table 3).
DISCUSSION
The treatment of UTIs has evolved over time toward the therapeutic goals of eradicating the causa- tive uropathogen, resolving the clinical manifestations, minimizing the adverse events, and preventing rein- fection.
9A variety of antimicrobials, including amoxi- cillin, trimethoprim-sulfamethoxazole, tetracycline, and fluoroquinolones, have been used successfully for the treatment of UTIs. However, concerns have been expressed regarding relapse or reinfection related to resistance of pathogens to antimicrobials. Treatment of UTIs is limited by increasing bacterial resistance to conventional antimicrobials.
10The 8-methoxy fluoroquinolones are thought to be associated with a lower degree of resistance develop- ment than older fluoroquinolones. In comparison with the older fluoroquinolones, such as ciprofloxacin, patho- gens are considered 1000-fold less likely to acquire resistance mutations to 8-methoxy fluoroquinolones, thus enhancing their bactericidal activity.
11Gatifloxacin is an 8-methoxy fluoroquinolone with good in vitro activity against clinically Gram positive and negative aerobes, atypical organisms (Chlamydia pneumoniae,
Mycoplasma pneumoniae, and Legionella pneumo- philia) and some anaerobes. It is also well-absorbedfrom the gastrointestinal tract and has a long plasma elimination half-life that allows once-daily administ- ration.
12On the basis of various advantages compared to the other older fluoroquinolones, we undertook a study to evaluate the efficacy and safety of gatiflo- xacin for chronic prostatitis, which is one of the most common problems in Korean urologic practice.
Chronic prostatitis and chronic pelvic pain syndrome are disabling conditions that are poorly understood and affect 10-14% of men of all ages and ethnic origins.
13Reports show that as many as 50% of men at some point in their life, are affected by this condition.
2Fluoroquinolones have already been used successfully in the treatment of chronic prostatitis and are recom-
mended as first-line treatment for this indication.
Because of the unique environment within the prostate, fluoroquinolones, with their favorable pharmacokinetic qualities, are considered the agents of choice. The duration of antimicrobial treatment is based on many clinical studies and fluoroquinolones are generally given for at least 4-6 weeks.
14This recommendation is based on their antibacterial activity; on their ability to penetrate into prostatic tissue, prostatic fluid, seminal fluid, and ejaculate; as well as clinical studies.
15The duration of antimicrobial therapy in this study was also followed this general rule in principle. Atypical pathogens including Chlamydia pneumoniae, Myco-
plasma pneumoniae, Ureaplasam urealyticum are notwell covered by the antibacterial activity of classical fluoroquinolones such as ciprofloxacin or ofloxacin.
Naber et al suggested that the relatively high concen- tration of gatifloxacin in prostatic and seminal fluid as compared to those of other fluoroquinolones, along with the extended antibacterial spectrum, indicate that gatifloxacin may be an appropriate therapeutic agent for chronic prostatitis.
16The NIH-CPSI
7was developed to measure outcomes
in clinical trials. This tool is used to measures the
three most important domains for patients with chronic
prostatitis: pain, voiding symptoms, and impact on the
quality of life. The sensitivity and specificity of the
CPSI in clinical trials has been confirmed in a number
of randomizedplacebo-controlled trials and its value in
epidemiological studies is also being confirmed. There
is emerging evidence that this index will also be
useful for clinicians in practice to utilize for initial
assessment and follow-up of patients presenting with
the chronic pelvic pain syndrome.
14With the above
noted advantages of the NIH-CPSI we measured the
clinical outcomes for gatifloxacin treatment in patients
with prostatitis using this tool. In this study, a total of
149 patients participated, thetotal NIH-CPSI score as
well as sub-scores of pain, urinary symptoms and
impact on the quality of life were significantly reduced.
In addition, for the NIH category II and IIIa patients, the total NIH CPSI score as well as sub- cores of pain, urinary symptoms and impact on the qualityof life were also dramatically reduced. The overall clini- cal efficacy assessment of gatifloxacin on prostatitis by investigators, even though improvement in the NIH category II group was not a great as category IIIa patients, most patients out of the total of 149 were assessed to be responders to the medication. The main limitation of this study is the absence of a control group. There is limited information from randomized controlled studies on this topic. However, to establish the role of antimicrobials, especially in category IIIa patients, a placebo or a non antimicrobial control arm is necessary.
In this bacteriological study, E. coli was by far the most common cause of NIH category II prostititis.
However, NIH category II prostititis can also be caused by other Gram positive and negative organisms such Proteus, Klebsiella, Enterococcus, Staphylococcus
and Streptococcus. The modern generations of fluoro-quinolones such as gatifloxacin have a spectrum of activity that covers these problematic bacteria.
1,4,5,12This study also demonstrated a strong bacteriological response, i.e. overall eradication rate of pathogens in NIH category II and pyuria elimination rates in NIH category II/IIIa at one month aftertreatment completion were 85% and 79.2%, respectively. Correlation of cli- nical outcome and bacteriological response included some patients who were considered to have clinical success but had bacteria or pyuria after treatment completion. This suggests that for chronic prostatitis, clinical cure and eradication of pathogens or pyuria may not always correlate.
Our findings show that treatment with fluoroqui- nolones is well tolerated and has a good safety profile;
the majority of adverse events were of mild or moderate intensity. Furthermore, fluoroquinolone-nduced adverse events have not been reported to occur with an increased frequency in the elderly.
17,18In this study,
the frequency of gatifloxacin induced adverse events was 16.1% and the majority of adverse events inclu- ding nausea, headache, diarrhea, dizziness were of mild to moderateseverity except for one patient who withdrew medication due to treatment-related gastric distress. This study found a similar safety profile when compared to previous reports.
19-22CONCLUSION
These results suggest that gatifloxacin in Korean urologic practice is safe and well tolerated and improves the clinical outcomes in patients with chronic prostatitis (NIH category II or IIIa).
ACKNOWLEDGEMENTS
This study was supported and funded by Handok- Aventis pharmacy, Seoul, Korea. We thank all the physicians who participated in this surveillance study.
REFERENCES
1. Graninger W, Wenisch C, Presterl E. Quinolones in the treatment of complicated urinary tract infection. Int J Antimicrob Agents 1994;4:29-37
2. Lipsky BA. Urinary tract infections in men. Epidemio- logy, pathophysiology, diagnosis and treatment. Ann Intern Med 1989;110:138-50
3. Roberts RO, Lieber MM, Rhodes T, Girman CJ, Bost- wick DG, Jacobsen SJ. Prevalence of a physician di- agnosis of prostatitis: the Olmstead County study of urinary symptoms and health status among men. Uro- logy 1998;51:578-84
4. Hosaka M, YaasueT, Fukuda H, Tomizawa H, Aoyama H, Hirai K. In vitro and in vivo antibacterial activities of AM-1155, a new 6-fluoro-8-methoxy quinolone. Anti- microb Agents Chemother 1992;36:2108-17
5. Miyashita N, Niki Y, Kishimoto T, Nakajima M, Ma- tsushima T. In vitro and in vivo activities of AM- 1155, a new fluoroquinolone, against Chlyamidia spp..
Antimicrob Agents Chemother 1997;41:1331-4
6. Meares EM, Stamey TA. Bacteriologic localization pat- terns in bacterial prostatitis and urethritis. Invest Urol 1968;5:492-518
7. Litwin MS, McNaughton-Collins M, Fowler Jr FJ, Nickel JC, Calhorn EA, Pontari MA, et al. The National Institutes of Health Chronic Prostatitis Symp- tom Index: development and validation of a new out- come measure. J Urol 1999;162:369-75
8. Farrington CP, Manning G. Test statistics and a sam- ple size formulae for comparative binomial trials with null hypothesis of non-zero risk difference of non-uni- ty relative risk. Stat Med 1990;9:1447-54.
9. Kunin CM. Urinary tract infections in females. Clin Infect Dis 1994;18:1-12
10. Rubin RH, Shapiro ED, Andriole VT, Davis RJ, Stamm WE. General guidelines for the evaluation of new anti-infective drugs for the treatment of urinary tract infection. Clin Infect Dis 1992;15S1:S216-27 11. Zhao X, Xu C, Domagala J, Drlica K. DNA topoiso-
merase targets of the fluoroquinolones: a strategy for avoiding bacterial resistance. Proc Natl Acad Sci USA 1997;94:13991-6
12. Mandell LA. Safety and efficacy of gatifloxacin in community-acquired pneumonia: rationale for the Tequin Clinical Experience Study (TeqCES). Diag Microbiol Infect Dis 2002;44:65-7
13. Mehik A, Hellstrom P, Lukkarinen O, Sarpola A, Jar- velin M, et al. Epidemiology of prostatitis in Finnish men: a population-based cross-sectional study. BJU Int 2000;86:443-8
14. Schaeffer AJ. NIDDK-sponcered chronic prostatitis col- laborative research network (CPCRN) 5-year data and treatment guidelines for bacterial prostatitis. Int J Anti- microb Agents 2004;24S:S49-52
15. Naber KG. Role of quinolones in treatment of chronic
bacterial prostatitis. In: Hooper DC, Wolfson JSO, edi- tors. Quinolone antimicrobial agents, 2nd ed. American Society for Microbilology: Washington DC; 1993;
285-97
16. Naber CK, Steghafner M, Kinzig-schippers M, Sauber C, Sorgel F, Stahlberg H, et al. Concentrations of gati- floxacin in plasma and urineand penetration into pro- static and seminal fluid, ejaculate, and sperm cells af- ter single oral administrations of 400 milligrams to volunteers. Antimicrob Agents Chemother 2001;45:
293-7
17. Nicolle LE. Quinolones in the aged. Drugs 1999;58:
49-51
18. Breen J, Skuba K, Grasela D. Safety and tolerability of gatifloxacin, an advanced-generation, 8-methoxy flu- oroquinolone. J Respir Dis 1999;20:S70-6
19. Naber KG, Allin DM, Clarysse L, Haworth DA, James IGV, Raini C, et al. Gatifloxacin 400mg as a single shot or 200mg once daily for 3 days is as effective as ciprofloxacin 250 mg twice daily for the treatment of patients with uncomplicated urinary tract infections.
Int J 2004;23:596-605
20. Nicodemo AC. An open label, multicenter, non-com- parative study of the efficacy and safety of oral gati- floxacin in the treatment of community-acquired pneu- monia: a Brazilian study in five centers. BJID 2003;
7:62-8
21. Stahlmann R, Lode H. Fluoroquinolones in the elderly.
Drugs Anging 2003;20:289-302
22. Naber KG, Bartnicke A, Hanus M, Milutinovic S, van Belle F, Schonwald S, et al. Gatifloxacin 200 mg or 400 mg once daily is as effective as ciprofloxacin 500 mg twice daily for the treatment of patients with acute pyelonephritis or complicated urinary tract infec- tions. Int J Antimirob Agents 2004;23S1:S41-53