Index terms Thyroid Disease
Positron Emission Tomography Ultrasound
Malignancy
INTRODUCTION
Incidental thyroid lesions (ITLs) detected on 18F-fluorodeoxy- glucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) are defined as incidentally found abnor- malities in the thyroid gland on 18F-FDG PET/CT in patients with non-thyroidal disease (1). 18F-FDG PET/CT is increasingly used to evaluate localization, stage of primary index tumors,
and follow-up for primary and metastatic lesions in patients with various kinds of malignancies (2). The current widespread use of 18F-FDG PET/CT in patients with non-thyroidal malig- nancies has resulted in an increase in detection of ITLs. The strategy for managing these lesions is important for predicting patient prognosis and cost-effectiveness.
Ultrasound (US) and subsequent US-guided fine needle aspi- ration (US-FNA) are widely recommended for evaluating ITLs
J Korean Soc Radiol 2014;71(3):111-119 http://dx.doi.org/10.3348/jksr.2014.71.3.111
Received May 14, 2014; Accepted June 18, 2014 Corresponding author: Jung Hee Shin, MD Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 135-710, Korea.
Tel. 82-2-3410-6420 Fax. 82-2-3410-0049 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
Purpose: To evaluate the clinical implications of subsequent ultrasound (US) for in- cidental thyroid lesions (ITLs) detected on positron emission tomography/computed tomography (PET/CT) in patients with non-thyroidal cancer.
Materials and Methods: We retrospectively searched for ITLs in 2703 patients with non-thyroidal cancer on 3226 PET/CT examinations. We divided the patients into two groups: US-performed and US-not performed groups. Diagnostic performance of US in detecting malignancy was analyzed according to the PET/CT findings.
Results: The incidence of ITLs on PET/CT in patients with non-thyroidal cancer was 8.4% (226/2703). Death rate from disease and stage were not significantly different between the groups. The malignant rate of ITLs that had cytopathology was 39%
(22/57). All malignancies were primary thyroid cancers except for one metastasis.
Overall diagnostic performance of US was 87% sensitivity, 66% specificity, 66%
positive predictive value (PPV), and 89% negative predictive value (NPV). The diag- nostic performance of US according to the PET/CT findings was probable benign on PET/CT (n = 9): 100% specificity, 100% NPV; suspicious malignant on PET/CT (n = 22): 75% sensitivity, 90% specificity, 90% PPV, 75% NPV; and undetermined on PET/CT (n = 26): 100% sensitivity, 94% specificity, 91% PPV, 100% NPV.
Conclusion: ITLs did not affect the prognosis of patients with non-thyroidal cancer whether subsequent US was performed or not. Subsequent US may be unnecessary for ITLs with probable benign findings on PET/CT.
Incidental Thyroid Lesions Detected on
18F-Fluorodeoxyglucose Positron Emission Tomography/CT in Patients with Non-Thyroidal Cancer: Clinical Implications and the Value of Ultrasound
1비갑상선암 환자에서 시행한 18F-Fluorodeoxyglucose Positron Emission Tomography/CT에서 발견된 갑상선 우연종에 대한 초음파의 임상적 가치에 대한 연구1
Kwang Hwi Lee, MD
1,2, Jung Hee Shin, MD
1, Boo-Kyung Han, MD
1, Eun Young Ko, MD
1, Eun Sook Ko, MD
1, Soo Yeon Hahn, MD
1, Joon Young Choi, MD
3Departments of 1Radiology, 3Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Department of Radiology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea
performance of US to detect malignancy as follows: sensitivity, specificity, positive predictive value (PPV) and negative predic- tive value (NPV), according to the 18F-FDG PET/CT findings.
18F-FDG PET/CT
All patients fasted for at least 6 hours prior to the 18F-FDG PET/
CT examinations but were allowed to drink water. The 18F-FDG PET/CT scans were performed using a GE Discovery LS PET/CT scanner (GE Healthcare, Milwaukee, WI, USA). A whole-body CT scan was performed using a continuous spiral technique with an eight-slice helical CT that had a gantry rotation speed of 0.8 second. The acquisition protocol of the CT scan was as follows:
40−120 mAs adjusted by body weight, 140 kVp, a section slice width of 5 mm, and a table feed of 5 mm per rotation. Neither in- travenous nor oral contrast agent was used. After the CT scan was obtained, PET imaging was obtained at 60 ± 5 minutes after intra- venous injection of 370 MBq 18F-FDG. We reconstructed PET images using CT data for attenuation correction and image fusion and an ordered subset expectation maximization algorithm (28 subsets, two iterations) with Gaussian smoothing filter (full width at half maximum = 5.45 mm). The trans-axial images were scanned in a 128 × 128 matrix (pixel size = 4.29 × 4.29 mm) with a slice thickness of 4.25 mm. Commercial software (Xeleris, GE Healthcare, Milwaukee, WI, USA) was applied to exactly co-reg- ister the separate CT and PET scan data.
We divided 18F-FDG uptake into two patterns of focal: 18F- FDG uptake in less than a lobe of the thyroid gland or diffuse:
18F-FDG uptake in near or an entire thyroid gland. When we con- sidered 18F-FDG uptake as abnormal on the visual analysis, we drew three-dimensional regions of interest to quantify the maxi- mum standardized uptake value (SUVmax) normalized for body weight. ITLs were defined as an increase in 18F-FDG up- take on PET and/or an abnormal attenuated lesion on CT in any portion of the thyroid gland, regardless of a focal or diffuse pat- tern. A thyroid incidentaloma was defined as a focal lesion that revealed focal 18F-FDG uptake on PET or a nodule on CT. The
18F-FDG PET/CT findings were retrospectively classified into three categories of suspicious for malignant: unilateral/focal 18F- FDG uptake with SUVmax > 4.2; probably benign: bilateral/dif- fuse 18F-FDG uptake with SUVmax < 1.3 or no discernible thy- roid nodule on CT; and undetermined: categorized into neither suspicious for malignant nor probably benign (6).
to enhance diagnostic accuracy (3). However, the question aris- es if such a strategy is sensible in patients with underlying ma- lignancies and various PET/CT findings. When abnormal le- sions of the thyroid gland are present on 18F-FDG PET/CT, patients with non-thyroidal malignancies are justified for fur- ther evaluation, as compared to the healthy screening popula- tion. Therefore, subsequent US or US-FNA could possibly be overused. Sensitivity and specificity of 18F-FDG PET/CT to dif- ferentiate malignancies from benign thyroid lesions have been reported to be 60−80% and 66−91%, respectively (2). Although the diagnostic value of 18F-FDG PET/CT and US for abnormal thyroid lesions has been reported in many studies (3-5), no re- port has evaluated the diagnostic value of subsequent US ac- cording to 18F-FDG PET/CT findings for ITLs, particularly in patients with non-thyroidal malignancies, which are frequently encountered in clinical practice.
The purpose of this study was to evaluate the clinical implica- tions and value of subsequent US for ITLs detected on 18F-FDG PET/CT in patients with non-thyroidal cancer according to 18F- FDG PET/CT findings.
MATERIALS AND METHODS
Patients
This retrospective study was approved by our Institutional Re- view Board, and the informed consent requirement was waived.
A total of 3226 18F-FDG PET/CT examinations in 2703 patients with non-thyroidal cancer were performed between March 2006 and March 2008 at the nuclear medicine department of our institution. The patients underwent 18F-FDG PET/CT for cancer staging before treatment, detection of distant metastasis, and localization of a recurrent tumor.
Patients with ITLs detected on 18F-FDG PET/CT were divid- ed into a US-performed group in which subsequent US was performed to evaluate thyroid lesions after 18F-FDG PET/CT, and a US-not performed group in which subsequent US was not performed. Subsequent US was determined at the clinician’s discretion. The two groups were compared with regard to age, death rate from disease, and non-thyroidal cancer stage.
US findings were analyzed for patients in the US-performed group who underwent surgery or sufficient clinical and radio- logic follow-up of at least 1 year. We analyzed the diagnostic
primary non-thyroid malignancy were analyzed by Pearson’s chi-square test or the Wilcoxon rank-sum test, and 3 year mor- tality rates were analyzed by Pearson’s chi-square test. The diag- nostic performance of US was analyzed by McNemar’s chi- square test. p values < 0.05 were considered significant. Numeric data are expressed as mean ± standard deviation.
RESULTS
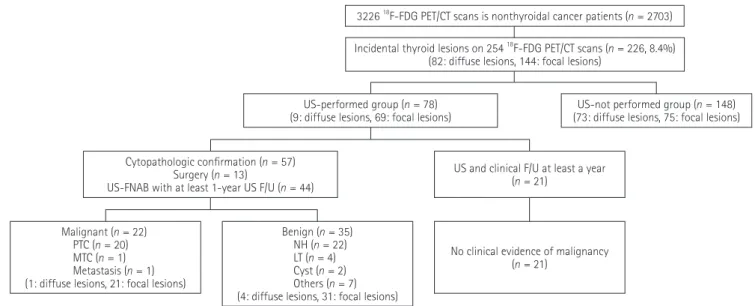
The incidence of ITLs detected on 18F-FDG PET/CT exami- nations was 8.4% (226 of 2703 patients with non-thyroidal can- cer) (Fig. 1). Among the 226 patients, 82 (36%) showed diffuse
18F-FDG uptake, and 144 (64%) had focal lesions with or with- out 18F-FDG uptake. The incidence of thyroid incidentaloma (focal lesion) on 18F-FDG PET/CT was 5.3% (144/2703).
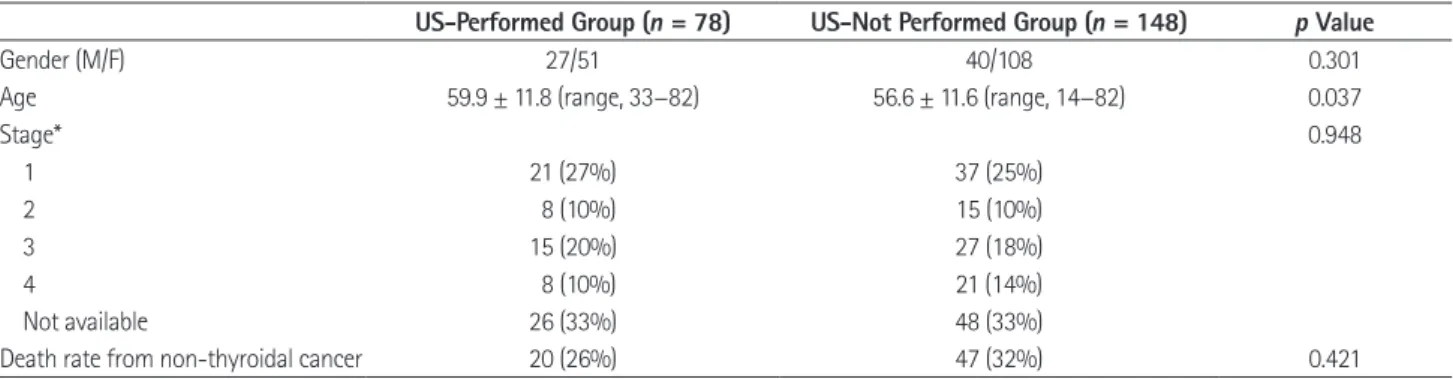
Of the 226 patients with ITLs, the US-performed group was composed of 78 (35%) and the US-not performed group was comprised of 148 (65%). The US-performed group included 27 males and 51 females (mean age, 59.9 ± 11.8 years; range, 33−82 years). The US-not performed group was 40 males and 108 fe- males (mean age, 56.6 ± 11.6 years; range, 14−82 years). The age of patients in the US-performed group was significantly older than that in the US-not performed group (p = 0.037), but sex and stage of non-thyroidal malignancies were not significantly different between the two groups (Table 1). The 3-year mortality US and US-FNA
US examinations were performed using high-resolution US equipment (IU22; Philips Medical Systems, Bothell, WA, USA or HDI 5000; Advanced Technology Laboratories, Bothell, WA, USA) with 5−12 MHz linear array transducers by one of seven board-certified radiologists. US examinations included an eval- uation of the whole thyroid gland and the lateral neck compart- ments (levels I, II, III, IV, or V). The US diagnosis was divided into “suspicious for malignant” and “probably benign”. Suspi- cious for malignant US findings included taller-than-wide shape, infiltrative margin, microcalcifications, and marked hy- poechogenicity (7). We diagnosed nodules as “suspicious for malignant” if there was one or more suspicious findings.
US-FNA was performed by radiologists. Using the freehand technique and direct US visualization, a 23-gauge needle tip was placed in the targeted lesion below the center of the transducer and was advanced to the lesion along the image plane. The aspirated material was placed on appropriately labeled glass slides, smeared, and fixed in 95% ethanol. The remainder of the material within the syringe was rinsed with ethanol for processing as a cell block. The slides were sent to the pathology department for analysis.
Statistical Analysis
The statistical analysis was performed using SPSS software (SPSS Inc., Chicago, IL, USA). Patient age, sex, and staging of
Fig. 1. Flow chart of the participants in the study.
Note.-F/U = follow-up, LT = lymphocytic thyroiditis, MTC = medullary thyroid carcinoma, NH = nodular hyperplasia, PET/CT = positron emission tomography/computed tomography, PTC = papillary thyroid carcinoma, US-FNAB = ultrasound-guided fine needle aspiration, 18F-FDG =
18F-fluorodeoxyglucose
3226 18F-FDG PET/CT scans is nonthyroidal cancer patients (n = 2703) Incidental thyroid lesions on 254 18F-FDG PET/CT scans (n = 226, 8.4%)
(82: diffuse lesions, 144: focal lesions)
US-performed group (n = 78) (9: diffuse lesions, 69: focal lesions)
Cytopathologic confirmation (n = 57) Surgery (n = 13)
US-FNAB with at least 1-year US F/U (n = 44)
Malignant (n = 22) PTC (n = 20) MTC (n = 1) Metastasis (n = 1) (1: diffuse lesions, 21: focal lesions)
Benign (n = 35) NH (n = 22) LT (n = 4) Cyst (n = 2) Others (n = 7) (4: diffuse lesions, 31: focal lesions)
No clinical evidence of malignancy (n = 21)
US-not performed group (n = 148) (73: diffuse lesions, 75: focal lesions)
US and clinical F/U at least a year (n = 21)
thology was 39% (22/57). All malignancies were primary thy- roid cancers except for one metastasis arising from esophageal cancer. Of the 57 lesions with final cytopathological results, the SUVmax of malignant lesions (mean: 7.62 ± 5.22, range: 1.7−24) was significantly higher than that of benign lesions (mean: 4.05
± 2.58, range: 1.0−12.9) (p = 0.001).
The diagnostic performance of subsequent US in all ITLs with cytopathological results revealed 86.4% (19/22) sensitivity, 71.4% (25/35) specificity, 65.5% (19/29) PPV, and 89.3% (25/28) NPV to detect malignancy (Table 3). Of probable benign lesions assessed by PET/CT (n = 9), US revealed 100% (9/9) specificity and 100% (9/9) NPV and had complete agreement with the final result. Four of nine lesions revealed diffuse and bilateral 18F-FDG uptake, and five lesions revealed focal low attenuated nodules without 18F-FDG uptake, which presented an SUVmax < 2.9 in all cases (Figs. 2, 3). Of the suspicious malignant lesions assessed by PET/CT (n = 22), US revealed 75% (9/12) sensitivity, 90%
(9/10) specificity, 75% (9/12) PPV, and 90% (9/10) NPV. Of 22 patients, 21 revealed focal 18F-FDG uptake in unilateral lobes.
The other patient, who had metastasis from esophageal cancer, revealed multifocal 18F-FDG uptakes in bilateral lobes. Mean SUVmax was 7.75 (range, 2.7−24). Of the undetermined lesions assessed by PET/CT (n = 26), US revealed 100% (10/10) sensi- tivity, 94% (15/16) specificity, 91% (10/11) PPV, and 100%
(15/15) NPV, corresponding to excellent agreement with the fi- nal results (kappa value = 0.92).
DISCUSSION
The incidence of ITLs detected on 18F-FDG PET/CT for pa- rate between US-performed group (26%, 20/78) and US-not
performed group (32%, 47/148) was not significantly different (p = 0.421). Table 2 shows the origin of the primary non-thyroi- dal cancers with ITLs.
Of the 78 patients in the US-performed group, 57 had cytopa- thological results. Thirteen patients underwent total thyroidec- tomy for primary thyroid cancers, and the remaining 44 pa- tients underwent US-FNA with clinical and radiologic follow- up. The final cytopathological results revealed malignant thyroid cancers (n = 22; papillary carcinoma: 20, medullary carcinoma:
one, metastasis: one) and benign lesions (n = 35; nodular hyper- plasia: 22, lymphocytic thyroiditis: four, cyst: two, others: seven).
The malignant rate in the US-performed group that had cytopa-
Table 1. Comparison of Clinical Characteristics of the Patients with Abnormal Thyroid Lesions on PET/CT between US-Performed Group and US-Not Performed Group
US-Performed Group (n = 78) US-Not Performed Group (n = 148) p Value
Gender (M/F) 27/51 40/108 0.301
Age 59.9 ± 11.8 (range, 33−82) 56.6 ± 11.6 (range, 14−82) 0.037
Stage* 0.948
1 21 (27%) 37 (25%)
2 8 (10%) 15 (10%)
3 15 (20%) 27 (18%)
4 8 (10%) 21 (14%)
Not available 26 (33%) 48 (33%)
Death rate from non-thyroidal cancer 20 (26%) 47 (32%) 0.421
Note.-*Stage of non-thyroidal cancer.
PET/CT = positron emission tomography/computed tomography, US = ultrasound Table 2. Primary Non-Thyroidal Cancers with Incidental Thyroid Le- sions in US-Performed Group and US-Not Performed Group
US-Performed Group
(n = 78) US-Not Performed Group (n = 148)
Lung cancer 34 37
Colon cancer 9 12
Stomach cancer 9 16
Breast cancer 6 19
Cervical cancer 4 11
Endometrial cancer 2 2
Lymphoma 2 14
Liver tumor 2 1
Pancreas cancer 2 7
Bile duct tumor 1 5
Renal tumor 1 0
Ovarian cancer 1 5
Esophageal cancer 1 3
Head and neck cancer 1 8
Other 3 8
Note.-US = ultrasound
subjects (2.6%) (6). Rheingold et al. (12) suggested that a history of malignancy could be one of the major risk factors for develop- ing another kind of malignancy. The reason that the incidence of thyroid incidentalomas in the present study was relatively higher was due to the population of only patients with primary malig- nancies, compared to including healthy subjects.
In the present study, the incidence of malignant ITLs detected on 18F-FDG PET/CT was 22 (39%) of 57 patients who had final cytopathology. Other investigations revealed that it ranges from 27% to 72% (4, 6, 9, 11, 13-15). Most of the 22 patients with ma- lignancies had primary thyroid carcinomas (20 papillary carcino- tients with non-thyroid cancer was 8.4%, which was similar to the
9% reported in a previous study that investigated both focal and diffuse 18F-FDG uptake lesions in thyroid gland (3). The inci- dence of thyroid incidentalomas (focal lesions) was 5.3% in our study, which was slightly higher than the 1.2−4.3% in other re- ports in both patients with malignancies and healthy subjects (8- 11). It seemed that this difference resulted from the population in the present study, which included only patients with nonthyroidal malignancies, and previous studies. The prevalence of thyroid in- cidentalomas detected on 18F-FDG PET/CT in patients with sus- pected or known cancer (4.1%) was higher than that in healthy
Table 3. Diagnostic Performance of US to Differentiate Malignancy for Incidental Thyroid Lesions
PET/CT Findings US
Sensitivity Specificity PPV NPV
Probable benign (n = 9) - 100 (9/9) - 100 (9/9)
Suspicious malignant (n = 22) 75.0 (9/12) 90.0 (9/10) 75.0 (9/12) 90.0 (9/10)
Undetermined (n = 26) 100 (10/10) 93.8 (15/16) 90.9 (10/11) 100 (15/15)
Overall (n = 57) 86.4 (19/22) 71.4 (25/35) 65.5 (19/29) 89.3 (25/28)
Note.-NPV = negative predictive value, PET/CT = positron emission tomography/computed tomography, PPV = positive predictive value, US = ultrasound
Fig. 2. A 59-year-old female with sarcoma in the right pulmonary artery. The 18F-FDG PET/CT reveals a 2 cm low-attenuated nodule (arrowhead) with no uptake in the left lower thyroid lobe (A). Ultrasonograms show a smooth solid and cystic nodule (arrows) in the inferior pole of the left thyroid gland, which was diagnosed as a probably benign nodule (B: axial scan, C: longitudinal scan). Nodular hyperplasia was confirmed by US- guided fine needle aspiration.
Note.-PET/CT = positron emission tomography/computed tomography, US = ultrasound, 18F-FDG = 18F-fluorodeoxyglucose B
A C
study, 21 primary thyroid cancers of 22 ITLs proven to be malig- nant had focal uptake (unilateral uptake in 18 patients and bilat- eral in three patients). The other of the 22 lesions was a metasta- sis arising from esophageal cancer, which presented as diffuse and bilateral uptake in the thyroid gland, although US suggested bilateral aggressive masses. Because all primary thyroid cancers revealed focal uptake, we excluded primary thyroid cancers from incidental thyroid lesions with diffuse and bilateral uptake.
However, diffuse and bilateral uptake should be handled vigi- lantly in patients with non-thyroid cancer because this finding can indicate metastasis.
Because the mean SUVmax value of malignant lesions was higher than that of benign lesions in the current study, we purport that the SUVmax value can help distinguish malignant lesions from benign. Cohen et al. (9) reported that the average SUVmax in malignant lesions (6.92 ± 1.54) was higher than that in benign lesions (3.37 ± 0.21). In another study, the diagnostic accuracy of SUVmax using a 4.2 cut-off value was 69.5%, without adding oth- er imaging findings (3). In contrast, the SUVmax between benign mas and one medullary carcinoma), but the other one had me-
tastasis arising from esophageal cancer. Most malignant nodules detected on 18F-FDG PET/CT were well-differentiated papillary carcinomas, as reported by Deandreis et al. (5) and Pagano et al.
(16). Our study had no discrepancies to previously reported studies, although the healthy population was excluded in the present study.
Most researchers evaluate focal or diffuse uptake, unilateral or bilateral uptake, and the SUVmax value to distinguish malig- nant from benign disease for ITLs on 18F-FDG PET/CT (4, 11, 13, 16). ITLs detected by PET/CT had diffuse or focal 18F-FDG uptake patterns. The diffuse uptake pattern is more frequently benign disease, such as thyroiditis, nodular goiter, or Grave’s dis- ease (16). Focal uptake of thyroid incidentalomas is clinically more significant due to its high risk of malignancy, including primary thyroid cancer and metastasis (6, 9, 14, 15). The risk of malignancy was extremely low (1.4%) in patients with diffuse or bilateral uptake on PET scans, while focal or unilateral uptake revealed a higher risk (15%) of malignancy (11). In the present
Fig. 3. A 47-year-old female with lung cancer. The 18F-FDG PET/CT reveals a 1 cm low-attenuated nodule (arrowhead) with mild uptake (SUV: 4.1) in the right thyroid lobe, which was diagnosed as a undetermined lesion (A). A 0.7 cm irregular hypoechoic nodule (arrow) with several microcal- cifications is demonstrated on ultrasound, which was considered suspicion for malignancy (B: axial scan, C: oblique scan). Papillary thyroid carci- noma was confirmed by total thyroidectomy.
Note.-PET/CT = positron emission tomography/computed tomography, SUV = standardized uptake value, 18F-FDG = 18F-fluorodeoxyglucose B
A C
correlation among CT, sonography, and pathology. AJR Am J Roentgenol 2006;187:1349-1356
2. Bae JS, Chae BJ, Park WC, Kim JS, Kim SH, Jung SS, et al. In- cidental thyroid lesions detected by FDG-PET/CT: prevalence and risk of thyroid cancer. World J Surg Oncol 2009;7:63 3. Kang BJ, O JH, Baik JH, Jung SL, Park YH, Chung SK. Inci-
dental thyroid uptake on F-18 FDG PET/CT: correlation with ultrasonography and pathology. Ann Nucl Med 2009;23:
729-737
4. Kwak JY, Kim EK, Yun M, Cho A, Kim MJ, Son EJ, et al. Thy- roid incidentalomas identified by 18F-FDG PET: sonographic correlation. AJR Am J Roentgenol 2008;191:598-603 5. Deandreis D, Al Ghuzlan A, Auperin A, Vielh P, Caillou B,
Chami L, et al. Is (18)F-fluorodeoxyglucose-PET/CT useful for the presurgical characterization of thyroid nodules with indeterminate fine needle aspiration cytology? Thyroid 2012;22:165-172
6. Choi JY, Lee KS, Kim HJ, Shim YM, Kwon OJ, Park K, et al.
Focal thyroid lesions incidentally identified by integrated 18F-FDG PET/CT: clinical significance and improved char- acterization. J Nucl Med 2006;47:609-615
7. Moon WJ, Baek JH, Jung SL, Kim DW, Kim EK, Kim JY, et al.
Ultrasonography and the ultrasound-based management of thyroid nodules: consensus statement and recommen- dations. Korean J Radiol 2011;12:1-14
8. Chen YK, Ding HJ, Chen KT, Chen YL, Liao AC, Shen YY, et al. Prevalence and risk of cancer of focal thyroid inciden- taloma identified by 18F-fluorodeoxyglucose positron emission tomography for cancer screening in healthy sub- jects. Anticancer Res 2005;25:1421-1426
9. Cohen MS, Arslan N, Dehdashti F, Doherty GM, Lairmore TC, Brunt LM, et al. Risk of malignancy in thyroid inciden- talomas identified by fluorodeoxyglucose-positron emis- sion tomography. Surgery 2001;130:941-946
10. Kim SJ, Kim BH, Jeon YK, Kim SS, Kim IJ. Limited diagnos- tic and predictive values of dual-time-point 18F FDG PET/
CT for differentiation of incidentally detected thyroid nodules. Ann Nucl Med 2011;25:347-353
11. Are C, Hsu JF, Schoder H, Shah JP, Larson SM, Shaha AR.
FDG-PET detected thyroid incidentalomas: need for fur- ther investigation? Ann Surg Oncol 2007;14:239-247 12. Rheingold SR, Neugut AI, Meadows AT. Secondary cancers:
and malignant thyroid nodules was not significantly different in one study, although the average SUVmax of the malignant thyroid lesions was higher than that of benign thyroid lesions (4).
The American Thyroid Association guidelines recommend that diagnostic thyroid US should be performed for thyroid in- cidentalomas detected on 18F-FDG PET/CT (17). According to the recommendations with consensus among the American As- sociation of Clinical Endocrinologists, Associazione Medici En- docrinologi, and the European Thyroid Association Medical guidelines, a US evaluation should be conducted because of un- certain risk of malignancy of thyroid incidentaloma (18). How- ever, subsequent US had no additional diagnostic value for ITLs with probable benign findings on 18F-FDG PET/CT in our study.
Of 26 patients with undetermined findings on 18F-FDG PET/
CT, the diagnostic performance of US showed excellent agree- ment with the final cytopathological results. The probability (13.2%) of malignancy was much lower than when the US find- ings appeared benign, as compared with significantly higher probability (75.5%) of malignance when the US findings were suspicious for malignant (4). Therefore, subsequent US can pro- vide additional diagnostic value when ITLs have undetermined findings on 18F-FDG PET/CT.
There are several limitations in this study. First, this study had selection bias to evaluate diagnostic performances of 18F-FDG PET/CT and US because only patients who underwent US-FNA or surgery were included. Second, the 3-year survival rate be- tween US-performed and US-not performed groups may not have been sufficient to evaluate long-term mortality rates of the patients. Third, we could not define criteria for subsequent US indications in this study because the 18F-FDG PET/CT and the US results were retrospectively analyzed. Large prospective stud- ies will need to solve the limitations of the present study.
In conclusion, ITLs detected on 18F-FDG PET/CT did not af- fect patient prognosis whether US was performed or not. Because subsequent US has no additional diagnostic value in ITLs with probable benign findings on 18F-FDG PET/CT, it may be unnec- essary for ITLs with benign findings on PET/CT.
REFERENCES
1. Shetty SK, Maher MM, Hahn PF, Halpern EF, Aquino SL.
Significance of incidental thyroid lesions detected on CT:
16. Pagano L, Samà MT, Morani F, Prodam F, Rudoni M, Bold- orini R, et al. Thyroid incidentaloma identified by 18F-flu- orodeoxyglucose positron emission tomography with CT (FDG-PET/CT): clinical and pathological relevance. Clin En- docrinol (Oxf) 2011;75:528-534
17. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differen- tiated thyroid cancer. Thyroid 2009;19:1167-1214
18. Gharib H, Papini E, Paschke R, Duick DS, Valcavi R, He- gedüs L, et al. American Association of Clinical Endocri- nologists, Associazione Medici Endocrinologi, and Europe- anThyroid Association Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules. Endocr Pract 2010;16 Suppl 1:1-43
incidence, risk factors, and management. In Kufe DW, Hol- land JF, Frei E. Cancer medicine, 6th ed. Hamilton, ON: BC Decker, 2003:2623
13. de Geus-Oei LF, Pieters GF, Bonenkamp JJ, Mudde AH, Bleeker-Rovers CP, Corstens FH, et al. 18F-FDG PET reduces unnecessary hemithyroidectomies for thyroid nodules with inconclusive cytologic results. J Nucl Med 2006;47:770-775 14. Kang KW, Kim SK, Kang HS, Lee ES, Sim JS, Lee IG, et al.
Prevalence and risk of cancer of focal thyroid incidentalo- ma identified by 18F-fluorodeoxyglucose positron emis- sion tomography for metastasis evaluation and cancer screening in healthy subjects. J Clin Endocrinol Metab 2003;
88:4100-4104
15. Kim TY, Kim WB, Ryu JS, Gong G, Hong SJ, Shong YK. 18F- fluorodeoxyglucose uptake in thyroid from positron emis- sion tomogram (PET) for evaluation in cancer patients:
high prevalence of malignancy in thyroid PET incidentalo- ma. Laryngoscope 2005;115:1074-1078
비갑상선암 환자에서 시행한 18F-Fluorodeoxyglucose Positron Emission Tomography/CT에서 발견된 갑상선 우연종에 대한
초음파의 임상적 가치에 대한 연구1
이광희
1,2· 신정희
1· 한부경
1· 고은영
1· 고은숙
1· 한수연
1· 최준영
3목적: 비갑상선암을 가진 환자에게 촬영한 positron emission tomography/computed tomography (이하 PET/CT)에서 발견된 갑상선 우연종에 대한 초음파의 임상적 가치에 대해서 평가하는 것이다.
대상과 방법: 2703명의 비갑상선암을 가진 환자에게 시행한 3226 PET/CT 검사에서 후향적으로 갑상선 우연종을 검색 하였다. 대상 환자를 초음파 시행군과 비시행군으로 나누었다. PET/CT의 소견에 따라 초음파에서 암을 진단할 수 있는 능력을 평가하였다.
결과: 비갑상선암 환자에게 발견된 갑상선 우연종의 빈도는 8.4%였다(226/2703). 초음파를 시행한 군과 시행하지 않 은 군 사이에 3년 사망률에는 차이가 없었다. 갑상선 우연종의 암의 빈도는 39%였다(22/57). 모든 암은 한 명의 전이암 과 한 명의 수질암을 제외하고 모두 유두암이었다. 초음파의 진단율은 87% 민감도, 66% 특이도, 66% 양성예측도, 89%
음성예측도를 나타내었다. 양성 PET/CT 소견을 보인 우연종에서 초음파의 진단율은 100% 특이도, 100% 음성예측도를 보였고, 악성 PET/CT 소견을 보인 우연종에서 초음파의 진단율은 75% 민감도, 90% 특이도, 90% 양성예측도, 75% 음 성예측도를 보였다.
결론: 갑상선 우연종에서 초음파의 시행여부는 환자의 예후에 영향을 주지 않는다. 우연종이 PET/CT에서 양성 소견을 보일 때에는 초음파의 시행이 불필요할 수 있다.
성균관대학교 의과대학 삼성서울병원 1영상의학과, 3핵의학과, 2인제대학교 의과대학 해운대백병원 영상의학과