대한소화기학회지 2003;42:337-340
서 론
1)염증성 섬유양 용종은 위장관의 매우 드문 병변으로 섬 유 조직, 혈관, 호산구를 포함한 많은 염증세포들로 구성된 국소적인 비신생성 성장을 하는 질환이다.1-3 위장관 염증성 섬유양 용종은 주로 위에 발생하지만 드물게 소장, 대장, 식도에서도 발생한다.1,2 발생 부위에 따라 증상은 다양하 며, 위에 생기면 상복부 불쾌감으로 나타나고, 소장에 위치 할 때는 구토, 심한 복통이나 장폐색이 올 수 있으나,4-8 대 량 공장 출혈로 보고된 예는 없었다. 이에 저자들은 공장의 대량 출혈로 발견된 염증성 섬유양 용종 1예를 경험하였기
접수: 2003년 3월 27일, 승인: 2003년 8월 12일 연락처: 이진관, 681-320, 울산광역시 중구 태화동 123-3
동강병원 내과
Tel: (052) 241-1201, Fax: (052) 241-1180 E-mail: [email protected]
에 문헌 고찰과 함께 보고한다.
증 례
2)35세 남자가 내원 10일 전부터 시작된 흑색변과 내원 당 일의 혈변으로 밤 11시경 응급실에 내원하였다. 환자는 평 소 건강한 환자로 약물 복용 및 복부 손상 등 특이 병력은 없었으며, 내원당시 활력 징후는 혈압 120/80 mmHg, 맥박 분당 72회, 체온 36.5℃, 호흡 분당 20회였다. 환자는 급성 병색을 띠었고, 결막은 창백하였으며, 복부 신체검사에서 압통은 없고 종괴는 만져지지 않았으며, 직장수지검사에
Correspondence to: Jin Kwan Lee, M.D.
Department of Internal Medicine, Dongkang General Hospital 123-3 Taehwa-dong, Joong-gu, Ulsan 681-320, Korea Tel: +82-52-241-1201, Fax: +82-52-241-1180 E-mail: [email protected]
공장 출혈로 발견된 염증성 섬유양 용종 1예
울산 동강병원 내과
황만근․김정훈․박상원․박재범․이창익․이창구․이진관
A Case of Inflammatory Fibroid Polyp Presenting with Jejunal Bleeding
Man Keun Hwang, M.D., Jung Hun Kim, M.D., Sang Won Park, M.D.,
Jae Bum Park, M.D., Chang Ik Lee, M.D., Chang Gu Lee, M.D., and Jin Kwan Lee, M.D.
Department of Internal Medicine, Dongkang General Hospital, Ulsan, Korea
Inflammatory fibroid polyp occurs very rarely in the jejunum and gastrointestinal bleeding as an initial manifestation of inflammatory fibroid polyp has not been reported. We report a case of a jejunal inflammatory fibroid polyp presenting with melena for 10 days. Upper gastrointestinal endoscopic examination was negative for any active bleeding lesions and abdominal angiography failed to localize the bleeding site as well. In contrast, computed tomography of the abdomen demonstrated a segmental wall thickening of the jejunum with a tumor-like mass lesion associated with dense contrast enhancement. Consistent with this, technetium
99m red blood cells scintigraphy exhibited red cell pooling at the right upper quadrant. On exploratory laparotomy, there was an active bleeding from the site of the jejunal tumor and a segmental resection was performed. Histologically, the tumor lesion of the jejunum was consistent with inflammatory fibroid polyp. Thus, we conclude that the tumor lesion was a cause of the gastrointestinal bleeding. (Korean J Gastroenterol 2003;42:337-340)
Key Words: Inflammatory fibroid polyp; Jejunal bleeding
대한소화기학회지: 제42권 제4호, 2003 338
Fig. 1. Abdominal CT scan. It shows a segmental thickening of the proximal small bowel loop with dense contrast enhancement in the arterial phase.
Fig. 2. Red blood cells scan. It shows that red cells are localized in an area of small bowel 5 minutes after radioisotope injection.
서 종괴나 협착은 없고 혈변이 묻어 나왔다. 내원 당시 시 행한 검사실 소견은 혈색소 6.5 gm/dL, 헤마토크릿 19.5%, 적혈구 1,940,000/mm3으로 빈혈 소견을 보였고, 백혈구 13,900/mm3, 혈소판은 278,000/mm3이었다. 혈청생화학검사
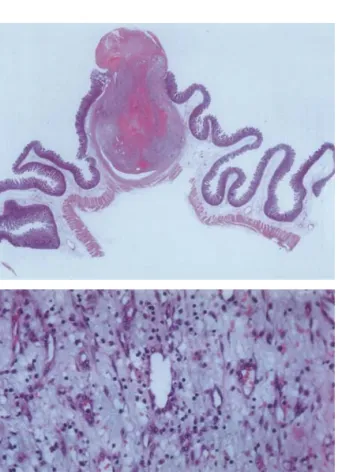
Fig. 3. Macroscopic finding of the resected specimen. It shows a dome-shaped nodular mass (1 cm in the dimension).
Fig. 4. Microscopic findings of the specimen. (A) A low power view (×15) and (B) a high power view (×200) show an inflammatory fibroid polyp composed of proliferation of blood vessels in an inflamed myxoid stroma (H&E stain).
에서 Na 136 mEq/L, K 3.8 mEq/L, BUN 26.9 mg/dL, 크레 아티닌 1.3 mg/dL, AST 11 IU/L, ALT 22 IU/L, 총 단백질 4.1 gm/dL, 알부민 2.7 gm/dL, 프로트롬빈 시간 13.9초, bleeding time은 2분, 대변잠혈반응 검사는 양성이었다. 위
A
B
황만근 외 6인. 공장 출혈로 발견된 염증성 섬유양 용종(Inflammatory Fibroid Polyp) 1예 339
비관에서는 맑은 위액만 나오고 상부위장관 내시경검사에 서 출혈은 발견되지 않았다. 내원 3시간 동안 3번의 혈변 과 혈압 90/50 mmHg, 맥박 분당 112회, 체온 37.0℃, 호흡 분당 28회로 불안정한 활력 징후를 보이고 출혈이 계속되 어 대장내시경을 시행하지 못하고 응급으로 동맥조영술을 시행하였으나 출혈 부위가 확인되지 않았다.
내원 8시간 동안 6번의 간헐적인 혈변이 있고 활력 징후 는 혈압 80/50 mmHg, 맥박 분당 120회, 체온 36.2℃, 호흡 분당 32회로 호흡 곤란이 발생하여, 수술 고려 후 출혈 부 위를 국소화하기 위해 시행한 복부 전산화 단층촬영에서 상부 공장에 7 cm 길이의 장벽 비후 소견과 1 cm 크기의 조영이 증강된 종괴가 있고, 주위 림프선 종대나 침윤은 보 이지 않았다(Fig. 1). 99mTechnetium-labelled RBC scan에서 5분이 경과할 때 소장 부위에서 출혈 소견이 관찰되어(Fig.
2) 종양에 의한 상부 공장 출혈을 의심하고 내원 10시간 후 응급 수술을 시행하였다. 수술 소견은 Treitz 인대 하방 10 cm 부위에 직경 1 cm 크기의 출혈을 동반한 종괴가 관찰 되었고, 주위 림프선 종대나 침윤은 보이지 않았다. 육안 소견에서 장관 내로 돌출된 반구 형태의 결절성 종괴로 직 경은 1 cm였고, 종괴의 절단면은 주변과 잘 구분되어 있으 며 중앙은 출혈반이 있는 노란 고형성의 종괴였으며(Fig.
3), 병리조직학적 소견은 점액성 기질, 혈관들의 증식 및 확 장, 섬유모세포와 몇 개의 림프형질세포를 보였고 중앙에 광범위한 출혈이 있었으며 부분적으로 조직화되어 있었다 (Fig. 4). 공장 부분 절제술 후 더 이상의 출혈은 없었고 특 별한 합병증 없이 퇴원하였다.
고 찰
염증성 섬유양 용종은 원인이 알려지지 않은 드문 질환 이다. Gastric submucosal granuloma with eosinophilic infiltration9로 보고된 이후 eosinophilic granuloma,4 heman- giopericytoma,10 fibroma,11 inflammatory pseudotumor,12 inf- lammatory fibroid polyp1-3,5-8,13-16
등 다양한 이름으로 불려 졌으며 현재는 inflammatory fibroid polyp(염증성 섬유양 용종)으로 널리 통용되고 있다. 위장관의 염증성 섬유양 용 종은 위, 특히 전정부에서 주로 발견되고 소장, 특히 공장 에서는 매우 드물게 발견된다.2 위장관의 염증성 섬유양 용 종 89예 중 14예가 소장에서 발견되었고, 이 중 단지 4예만 이 공장에서 발견되었으며, 4예 모두 임상적으로 장중첩 소 견을 보였다.2
병인은 확실히 밝혀지지 않았지만 세균성, 화학적, 대사 적 손상에 의한 점막 및 점막하 결합 조직의 염증반응으로 볼 수 있으며,3 약한 손상에 의한 장점막하 중간엽 조직의 조절되지 않는 증식이 원인이라는 가설도 있다.2
전 연령에서 다양하게 나타나며 중, 장년층에서 호발한 다.2 주로 단독 병변으로 나타나며, 드물게 다수 병변으로 나타나는 경우도 있다.13 육안적 형태는 폴립양 병변이 무 경성 병변보다 흔하며1,2 점막 표면에 종종 궤양이 형성되어
있고,2,14,15 크기는 0.2 cm부터 13 cm까지 다양하다.1,15
조직학적 소견은 점막하의 느슨한 결합 조직체로 구성되 어 있으며 장의 내강으로 돌출되어 있고 궤양을 동반하는 경우가 많다. 그리고 섬유 조직과 혈관망이 다양하게 분포 되어 있으며, 대부분 혈관이 잘 발달되어 있다.2 위와 소장 의 염증성 섬유양 용종 사이에 조직학적 차이가 있다. 위에 서는 자주 혈관 주위에 뚜렷한 섬유화가 있고 근육층은 거 의 침범하지 않는 반면 소장에서는 혈관 주위의 섬유화는 없고 근육층의 침범이 흔하다.15
증상은 복통이 가장 흔하며 병변 위치에 따라 종종 유문 협착 또는 소장폐색을 동반한다. 체중 감소도 나타나며 구 역, 설사, 출혈은 흔하지 않다.2,3 현재까지 대량의 위장관 출혈로 발견된 염증성 섬유양 용종의 보고는 없었다. 위장 관 출혈 중 소장 출혈은 흔하지 않으며, 현재까지 원인에 대한 체계적인 조사는 없었다. 위장관 출혈 환자의 수술 중 소장내시경검사를 시행받았던 44예 중, 13예(30%)에서는 원인을 밝히지 못했고, 15예(34%)에서는 혈관 이상, 12예 (27%)에서는 소장궤양, 2예(5%)에서는 신생물, 나머지 2예 (5%)에서는 임상적으로 큰 의미가 없는 점막 이상 등으로 보고된 바 있다.17
신체검진, 방사선학적 검사, 검사실 소견은 진단에 도움 이 되지 않고 절제된 조직의 병리조직학적 소견으로 확진 된다.5-8
치료는 절제술이 필요하며, 소장에 생기는 경우 진단이 어렵고 시험적 개복으로 확인된다. 최근 위나 대장에 생긴 병변의 치료로 내시경적 절제술이 보고되고 있으며14 악성 변화는 보고된 바 없고, 재발은 한 예에서만 보고되었다.4 본 증례는 35세 환자로서 위장관 출혈로 내원, 전산화 단층촬영 및 RBC scan에서 공장의 출혈성 종양이 의심되 어 수술을 받았으며, 병리조직학적 검사 결과 염증성 섬유 양 용종으로 확진되었다. 이 병변이 대량 위장관 출혈을 일 으킨 증례 보고는 없어 문헌 고찰과 함께 보고한다.
참 고 문 헌
1. Kim YI, Kim WH. Inflammatory fibroid polyps of gastro- intestinal tract. Evolution of histologic patterns. Am J Clin Pathol 1988;89:721-727.
2. Johnstone JM, Morson BC. Inflammatory fibroid polyp of the gastrointestinal tract. Histopathology 1978;2:349-361.
3. Helwig EB, Ranier A. A inflammatory fibroid polyp of the
The Korean Journal of Gastroenterology: Vol. 42, No. 4, 2003 340
stomach. Surg Gynecol Obstet 1953;96:355-367.
4. McGreevy P, Doberneck RC, Mcleay JM, Miller FA.
Recurrent eosinophilic infiltrate granuloma of the ileum causing intussusception in a 2-year-old child. Surgery 1967;
61:280-284.
5. Kim JS, Kwon SY, Byun KS, et al. Jejunal inflammatory fibroid polyp presenting as intussusception. A case report with review of the literature. Korean J Intern Med 1994;9:
51-54.
6. Winkler H, Zelikovski A, Gutman H, Mor C, Reiss R. Inf- lammatory fibroid polyp of the jejunum causing intussus- ception. Am J Gastroenterol 1986;81:598-601.
7. Nkanza NK, King M, Hutt MS. Intussusception due to inflammatory fibroid polyps of the ileum: a report of 12 cases from Africa. Br J Surg 1980;67:271-274.
8. Shih LN, Chang SL, Chuang SM, Kuo CF. Inflammatory fibroid polyp of the jejunum causing intussusception. Am J Gastroenterol 1997;92:162-164.
9. Vanek J. Gastric submucosal granuloma with eosinophilic infiltration. Am J Pathol 1949;25:397-411.
10. Olsen EGJ, Wellwood JM. Hemangiopericytoma of the small
intestine. A report of three cases. Br J Surg 1970;57:66-69.
11. Pheils MT. A submucous fibroma of the ileum causing intussusception. Br J Surg 1952;40:135-137.
12. LiVolsi VA, Perzin KH. Inflammatory pseudotumors (inflammtory fibrous polyps) of the small intestine: a clinicopathologic study. Am J Dig Dis 1975;20:325-336.
13. Merkel IS, Rabinovitz M, Dekker A. Cecal inflammatory fibroid polyp presenting with chronic diarrhea: a case report and review of the literature. Dig Dis Sci 1992;37:133-136.
14. Tada S, Iida M, Yao T, et al. Endoscopic removal of inflammatory fibroid polyps of the stomach. Am J Gastro- enterol 1991;86:1247-1250.
15. Shimer GR, Helwig EB. Inflammatory fibroid polyps of the intestine. Am J Clin Pathol 1984;81:708-714.
16. Navas-Palacios JJ, Colina-Ruizdelgado F, Sanchez-Larrea MD, Cortes-Cansino J. Inflammatory fibroid polyps of the gastrointestinal tract. An immunohistochemical and electron microscopic study. Cancer 1983;51:1682-1690.
17. Ress AM, Benacci JC, Sarr MG. Efficacy of intraoperative enteroscopy in diagnosis and prevention of recurrent, occult gastrointestinal bleeding. Am J Surg 1992;163:94-98.