https://doi.org/10.12671/jkfs.2016.29.4.233
233
Copyright ⓒ 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received May 10, 2016 Revised June 8, 2016 Accepted July 1, 2016
Address reprint requests to: Hong-Ki Park, M.D.
Department of Orthopedic Surgery, Gachon University Gil Medical Center, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, Korea
Tel: 82-32-460-3384ㆍFax: 82-32-423-3384 E-mail: [email protected]
Financial support: None. Conflict of interest: None.
전위성 관절내 종골 골절의 관혈적 정복 시 종골 후방 조면 골편 정복의 중요성
박홍기 ⋅백종륜⋅최장석⋅이상진⋅백제원
가천대 길병원 정형외과
The Significance of Calcaneal Posterior Tuberosity Fragment Reduction When Treated with Open Reduction in Displaced Intra-Articular Calcaneal Fractures
Hong-Ki Park, M.D. , Jong-Ryoon Baek, M.D., Jang-Seok Choi, M.D., Sang-Jin Lee, M.D., Je-Won Paik, M.D.
Department of Orthopedic Surgery, Gachon University Gil Medical Center, Incheon, Korea
Purpose: We attempt to evaluate the significance of calcaneal posterior tuberosity fragment reduction when treated with surgical open reduction in displaced intra-articular calcaneal fractures.
Materials and Methods: A total of 90 patients with displaced intra-articular calcaneal fracture, between January 2010 and December 2015, treated with open reduction and internal fixation were enrolled in this study. At postoperative 3 months, we evaluated the reduction state of calcaneal posterior tuberosity fragment by measuring the degree of lateral displacement of the posterior tuberosity fragment on the calcaneal axial view. Moreover, we also evaluated the difference in the calcaneal length and height with the uninjured side on the lateral view of both sides. In addition, we estimated the reduction state of the posterior facet by measuring the degree of gap and step-off on the semi-coronal view of postoperative computed tomography and estimated the restoration of calcaneal angle by measuring the difference in Böhler’s and Gissane angle with the uninjured side on the lateral view of both sides.
Results: The correlation coefficient with 3 components for evaluating the reduction state of posterior tuberosity fragment and gap and step-off of posterior facet was r=0.538, 0.467, r=0.505, 0.456, r=0.518, and 0.493, respectively, and restoration of Böhler’s and Gissane angle was r=0.647, 0.579, r=0.684, 0.630, r=0.670, and 0.628, respectively. The relationship of each component shows a significant correlation as all p-values were <0.01.
Conclusion: The precise reduction of calcaneal posterior tuberosity fragment developed by the primary fracture line was considered as an important process of anatomical reduction of calcaneal body, including the posterior facet and calcaneal angle restoration.
Key Words: Calcaneus, Intra-articular fracture, Posterior tuberosity, Anatomical reduction
서 론
종골 골절은 모든 골절의 약 2%를 차지하며, 가장 흔한 족근골 골절로 전위성 관절내 골절은 종골 골절의 약 60%-75%를 차지한다. 후방 관절 소면을 포함한 관절내 분 쇄 골절의 치료법으로 보존적 치료로는 족관절의 상당한
Fig. 1. A 57-year-old male patient, with a Sanders type III intra-articular calcaneal fracture, was treated using open reduction and internal fixation with the extensile lateral approach. (A) Preoperative x-ray and computed tomography (CT) scans. (B) Postoperative x-ray and CT scans showed inaccurate reduction of posterior tuberosity fragment (yellowish arrow line), posterior facet step-off (yellowish circle), and collapsed Böhler’s angle (yellowish line).
기능장애를 초래하여 수술적 관혈적 정복 및 내고정이 보 편화되어 있으며, 해부학적 정복을 위한 다양한 수술적 접 근 방법이 제시되고 있다.1-5)
수술 시 종골 체부의 해부학적 정복 실패를 경험한 사례 를 복기하는 과정에서 정복 술기상 먼저 시행하게 되는 종 골 후방 조면 골편의 부정확한 정복이 모든 예에서 공통된 주요한 원인 중 하나임을 확인할 수 있었고(Fig. 1), 이에 저자들은 일차 골절 선에 의한 종골 후방 조면 골편의 정 복 상태와 후방 관절 소면 정복 상태 및 종골 각도 회복의 상관관계에 대하여 알아보고자 하였다.
대상 및 방법
1. 대상
2010년 1월부터 2015년 12월까지 비개방성 관절내 종골 골절로 수술적 치료 후 수술 부위 창상 감염의 합병증이 없었던 환자 97명 중 광범위 외측 도달법이 아닌 족근동 접근법으로 시행한 4명 및 정상적인 건측과의 비교를 위하 여 양측 골절을 보인 3명은 제외하고 총 90 명의 환자를 대
상으로 후향적 분석하였다. 수상 원인은 실족 60명, 교통사 고 24명, 기타 원인이 6명이었고, 남자 71명, 여자 19명, 평균 연령은 55.4세(18-79세), 우측 59명, 좌측 31명이었으 며, 모든 환자는 술 후 1년까지 경과 추시된 상태였다. 본 연구는 가천대 길병원 임상연구윤리위원회(institutional re- view board)의 승인을 받았다.
2. 수술 방법
수술은 2명의 술자에 의해 광범위 외측 도달법을 통한 관혈적 정복 및 금속판 내고정술을 시행하였다. 복와위 자 세로 뒤꿈치 외측에 절개를 시행한 후, 피하조직과 골막을 함께 박리하고, 거골하 관절면과 종입방 관절면의 노출 및 피판의 보호를 위하여 K-강선 3-4개를 삽입하여 시야를 확 보하였다. 일차 골절 선에 의한 후방 조면 골편의 정복을 위해 종골 후상방부에 내측에서 외측으로 6.5 mm Schanz 나사를 삽입하여 나사선이 약 3 mm 외측으로 돌출된 상 태를 유지하고, 이 부위와 거골하 관절부 K-강선 사이에 견인기(distractor)를 이용하여 후방 조면 골편의 내반 및 단축을 교정하였다. 교정 정도를 영상 증폭 장치상 종골
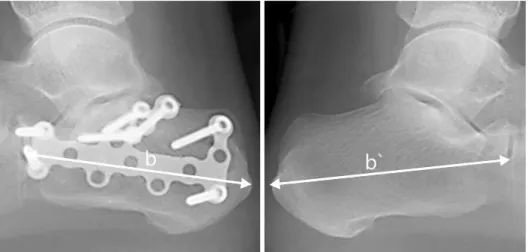
Fig. 3. The difference in the calcaneal length with the un- injured side (b-b`) is mea- sured from the most posterior point of the tuberosity to the calcaneocuboid joint on the lateral view.
Fig. 2. The degree of lateral displacement of the posterior tuberosity fragment (a) is measured as the gap between the superomedial fragment and posterior tuberosity fragment on the medial aspect of the calcaneal axial view.
축상면 영상으로 확인 후, 내측면의 정복 상태 및 후족부 의 높이 복구가 만족스럽게 이루어졌다면 이를 유지하고자 임시로 2.0 mm K-강선 2개를 후방 조면에서 재거돌기 방 향으로 삽입하였다. 그리고 관절면 관찰이 용이하도록 2개 의 작은 골막 거상기를 거골하 관절면 깊숙이 삽입, 거골 하 관절면을 이완하여 상외측 골편을 거골하 관절면에 정 복 후, K-강선으로 임시 고정하였고, 정복 상태를 Brodens 영상으로 확인하였다. 그 후 금속판 고정을 시행하고, 상외 측 골편이 작은 경우는 1-2개의 지연 나사로 추가 고정하 였다. 수술 후 단하지 석고 고정을 1주간 시행한 후 창상 상태가 양호하면 족관절 보조기를 착용하여 능동적 관절 운동을 시행하였으며, 부분적 체중 부하는 평균 6주에 시 행하였다.
3. 평가
방사선적 평가로 후방 관절 소면의 분쇄 정도는 Sander’s 분류5)를 적용하였다. 술 후 3개월 종골 축상면 영상에서 상외측 골편과 후방 조면 골편의 내측 간격을 측정하여 종 골 후방 조면 골편의 외측 전위 정도를 평가하였다. 양측 족부 외측면 영상에서 종입방 관절과 종골 후방 조면의 가 장 후방부 사이의 거리를 계측하여 종골 길이를 측정하였 고, 종입방 관절과 종골 후방 조면의 하면을 연결한 선의 수직선을 후방 관절 소면의 가장 상부로부터 계측하여 종 골 높이를 측정 후 건측과의 수치 차이로 종골 후방 조면 골편의 정복 상태를 평가하였다(Fig. 2-4). 수술 후 전산화 단층촬영을 통한 반관상면 영상에서 골절부 간격 및 층 형 성 정도를 계측하여 후방 관절 소면 정복 상태를 평가하였 고, 양측 외측면 영상에서 Böhler 각과 Gissane 각의 건측 과의 수치 차이를 측정하여 종골 각도 회복을 평가 후 비 교 분석하였다. 통계적 방법은 Pearson correlation method
를 사용하여 측정 항목 간의 상관관계를 분석하였고, IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA) 프로그램을 이용하였다.
결 과
1. 방사선적 계측치에 따른 결과
Sander’s 분류상 II 28명(IIA 10 명, IIB 11명, IIC 7명), III 43명(IIIAB 13명, IIIAC 10 명, IIIBC 20 명), IV 19명이었 으며, 종골 후방 조면 골편의 정복 상태를 평가하기 위한
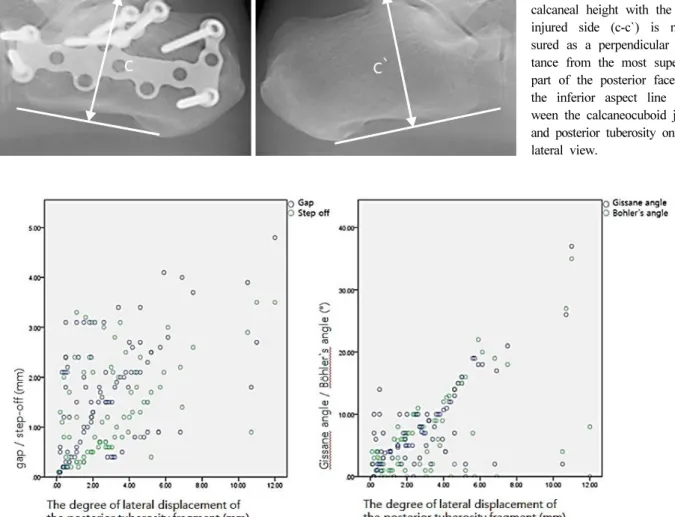
Fig. 4. The difference in the calcaneal height with the un- injured side (c-c`) is mea- sured as a perpendicular dis- tance from the most superior part of the posterior facet to the inferior aspect line bet- ween the calcaneocuboid joint and posterior tuberosity on the lateral view.
Fig. 5. The relationship between the degree of lateral displacement of the posterior tuberosity fragment and gap/step-off of posterior facet and restoration of Gissane angle/Böhler’s angle shows a significant correlation (p<0.01).
평균값은 후방 조면 골편 외측 전위 정도 3.19 mm, 건측 과의 종골 길이 차이 3.39 mm, 건측과의 종골 높이 차이 는 2.89 mm였다. 후방 관절 소면의 정복 상태를 평가하기 위한 골절부 간격은 평균 1.68 mm, 층 형성은 평균 1.30 mm였으며, 종골 각도 회복 상태를 평가한 Böhler 각도와 Gissane 각도의 건측과의 차이는 평균 6.36o, 7.32o였다.
2. 후방 관절 소면 정복 상태 및 종골 각도 회복과의 상 관관계
종골 후방 조면 골편의 정복 상태를 평가한 3가지 항목 인 후방 조면 골편 외측 전위 정도, 건측과의 종골 길이
차이 및 높이 차이와 골절부 간격 및 층 형성 간의 상관계 수는 각각 r=0.538 (p<0.01), 0.467 (p<0.01), r=0.505 (p<
0.01), 0.456 (p<0.01), r=0.518 (p<0.01), 0.493 (p<0.01)으 로, 모든 항목에서 통계적으로 의미 있는 상관관계를 보였 다. 마찬가지로 3가지 항목과 Böhler 및 Gissane 각도의 건측과의 차이를 측정한 항목 간의 상관계수는 각각 r=0.647 (p<0.01), 0.579 (p<0.01), r=0.684 (p<0.01), 0.630 (p<
0.01), r=0.670 (p<0.01), 0.628 (p<0.01)로 모든 항목에 서 통계적으로 의미 있는 상관관계를 보였다. 따라서 후방 조면 골편의 외측 전위 정도가 적고 건측과의 종골 길이 및 높이 차이가 적을수록 후방 관절 소면 골절부의 간격 및 층 형성 수치가 감소하여 후방 관절 소면 정복 상태가
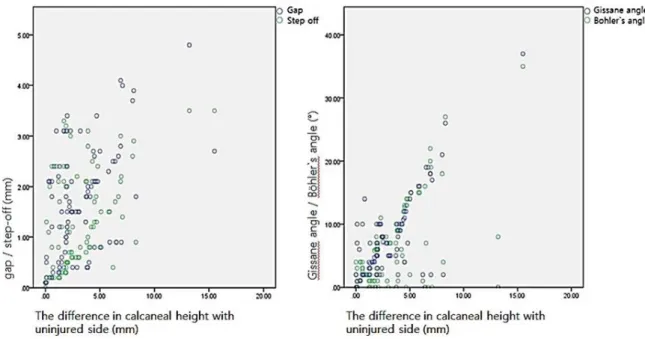
Fig. 7. The relationship between the difference in the calcaneal height with the uninjured side and gap/step-off of posterior facet and restoration of Gissane angle/Böhler’s angle shows a significant correlation (p<0.01).
Fig. 6. The relationship between the difference in calcaneal length with uninjured side and gap/step-off of posterior facet and restoration of Gissane angle/Böhler’s angle shows a significant correlation (p<0.01).
양호해지며, 건측과의 Böhler 및 Gissane 각 차이가 줄어 들어 종골 각도 또한 회복되는 것으로 볼 수 있었다(Fig.
5-7).
고 찰
전위성 관절내 종골 골절의 이상적인 치료 방법에는 아 직까지 논란이 존재한다.6-11) Randle 등12)은 메타 분석에서 수술적 치료가 더 나은 임상적 결과를 보이기는 하지만 반 드시 수술적 치료를 권유할 만한 근거는 다소 부족하다고
Fig. 8. The primary fracture line (yellowish line) produced two large fragments, SM, and posterolateral fragment (SL and PT). AL: Anterolateral fragment, SL: Superolateral fragment, SM: Superomedial fragment, PT: Posterior tuberosity frag- ment.
Fig. 9. In the semi-coronal computed tomography scan, the tuberosity tilts into the varus and acts as a wedge between SL and SM, preventing a reduction of the posterior facet. SL:
Superolateral fragment, SM: Superomedial fragment, PT: Poste- rior tuberosity fragment.
하였으며, Myerson과 Quill13)은 보존적 치료 후 거골하 관 절 통증, 종골 폭 증가, 내반 변형 및 비골건 충돌 등의 합병증이 발생하게 되면 후족부 높이 및 정렬 복구를 위해 거골하 관절 유합 및 교정 절골술이 필요하므로 초기 수술 적 치료를 권유하였다. 하지만 종골 체부 및 후방 관절 소 면의 정확한 정복은 족관절 기능 향상 및 보행의 정상화에 매우 중요하기 때문에 현재는 수술적 치료를 통한 해부학 적 정복이 점차 보편적인 치료방법으로 받아들여지고 있 다.5,14-18)
전위성 관절내 종골 골절의 병리 기전에 대한 이해는 골 절 치료를 위해 매우 중요하다. 수상 기전에 의하면 축성 부하가 족부에 가해질 시 골절 선은 족근동에서 시작하여 후방 관절 소면을 경유 후 내측면까지 진행하는 사선형 골 절 선이 형성되며, 이를 일차 골절 선(primary fracture line)이라고 한다. 일차 골절 선은 외측 Gissane 각 방향으 로부터 시작하여 때로는 거골하 전방, 중간 관절 소면 혹 은 종입방 관절면까지 진행하여 전외측 골편을 만든다. 또 한 종골 내측으로 진행하여 재거돌기 및 후방 관절 소면 내측 일부를 포함하는 상내측 골편(재거돌기 혹은 불변 골 편)과 후방 관절 소면 외측 일부(상외측 골편) 및 종골 후 방 조면 골편을 포함하는 후외측 골편으로, 2개의 큰 골편 을 형성한다(Fig. 8).15,19-23) 연속적인 외력이 가해지면 거골 하 후방 관절의 함몰을 유발하는 이차 골절선(secondary fracture line)이 발생하며, 이는 후방으로 진행하여 관절
함몰형 혹은 설상형 형태의 골절을 형성한다. 상내측 골편 은 강한 거종 골간 인대에 의해 고정되어 수상 시 전위가 드물게 발생한다. 그러나 후외측 골편 일부인 종골 후방 조면 골편은 종골의 전방 경부에서 분리 및 내반되어 종골 의 외측 벽을 방출 및 분쇄시키며, 아킬레스건에 의해 상 방으로 당겨져 족저 굴곡되고, 하퇴 삼두근의 힘에 의해 종골 경사각 및 종골 길이의 감소, 아킬레스 건의 단축이 발생한다. 전위된 종골 후방 조면 골편은 상외측 골편과 상내측 골편 사이에 쐐기 형태로 내반, 감입되어 상외측 골편의 전위를 조장시킨다(Fig. 9). 그러므로 전위된 종골 후방 조면 골편의 정확한 정복은 종골의 내측 정복 이외에 상외측 골편의 정복을 위한 공간 확보를 가능하게 하므로 후방 관절 소면의 해부학적 정복을 위한 선결 조건이라 할 수 있겠다.
족부 외측면 영상에서 측정되는 Böhler 각과 Gissane 각 은 종골 골절의 해부학적 복원의 질을 평가하는 방사선적 지표로 흔히 사용되고 있다.23) Böhler 각은 종골 후방 조 면 골편의 상방 전위 정도를 나타내며, Gissane 각은 후방 관절 소면을 포함하는 골절편의 전위 정도를 나타낸다. 따 라서 Böhler 각은 종골 후방 조면 골편의 정복 상태를 직 접적으로 반영하는 것으로 볼 수 있으며, Gissane 각 또한 후방 조면 골편의 정확한 정복이 후방 관절 소면의 해부학 적 정복을 위한 필수 조건이라는 점으로 미루어 후방 조면 골편의 정복 상태를 반영할 수 있을 것이다. 그러나 이 두
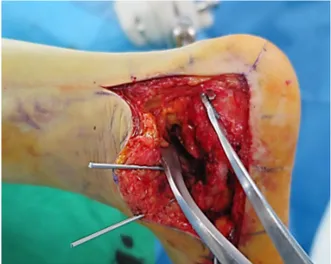
Fig. 10. We apply a distractor between the Schanz screw thread and K-wire inserted into the talar body and can achieve an effective traction of the tuberosity fragment.
가지의 종골 각도는 단지 시상면 상에서의 정복 상태를 평 가하는 지표이기에 시상면으로 골절 선이 형성된 경우에는 정상으로 측정될 수 있는 한계점이 존재하지만,19) 본 연구 를 통하여 종골 후방 조면 골편의 정복 상태와 의미 있는 상관관계가 있다는 것을 알 수 있었다.
전위된 종골 후방 조면 골편 정복을 위한 방법으로, Eastwood 등24)과 Tennent 등25)은 광범위 외측 도달법으로 접근 후, 함몰된 상외측 골편을 제거하고 재거돌기 및 종 골 후방 조면의 외측 면을 확인 후 골막 거상기를 삽입, 지렛대로 사용하여 후방 조면 골편을 아래로 내리고 내측 으로 이동시켜 정복하는 방법을 소개하였다. 재거돌기 골 편에 분쇄가 있거나 크기가 작은 경우에는 금기라고 하였 다. 문제점은 지렛대 방식으로 정복 도중 골 붕괴로 인한 단축이 초래될 수 있다는 점이다. 간접 정복 시 깊숙이 끼 어든 종골 후방 조면 골편을 조작하여 삼차원적 교정(종골 높이, 내외반 및 외측 전위 교정)을 하는 데 도움이 되는 술식으로 종골 후방에서 종축 방향으로 Schanz 나사를 삽 입하여 조작하는 방법(posterior Schanz pin, modified Westhues manoeuvre),5) 종골 외측에서 Schanz 나사를 삽입하여 조 작하는 방법(lateral Schanz pin)1) 혹은 Weber clamp를 사 용하는 방법26) 등이 있다.
저자는 앞선 수술 방법에서 기술하였듯이 6.5 mm Schanz 나사의 돌출된 일부 나사 선과 시야 확보를 위해 삽입한 거골하 관절부 K-강선 사이에 견인기를 이용하여 무리한 힘을 가하지 않고 종골 후방 조면 골편의 충분한 견인이 가능하였고(Fig. 10), 삽입해 놓은 Schanz 나사를 조작하여 내외반 변형 및 내외측 전위를 유용하게 교정할 수 있었다. Schanz 나사 삽입 또는 견인기 사용이 불가능
한 경우에는 Eastwood 등24)의 방법과 같이 후방 관절 소 면의 상외측 골편을 제거한 후 재거돌기 골편과 종골 후방 조면 골편의 외측 면을 확인하여, 골막 거상기 대신에 골 구(bone hook)를 두 골편의 내측부에 각각 거치 후 서로 반대 방향으로 견인하여 종골의 내측면 정복을 시행하였 다. 하지만 일차 골절 선이 전방으로 진행되면 전위된 종 골 후방 조면 골편의 조작이 힘들어 정복이 어려울 수 있 다. 향후 일차 골절 선이 전방 관절면을 침범한 경우 이에 대한 정복 방법에 대한 연구가 필요할 것으로 생각된다.
결 론
전위성 관절내 종골 골절에서 일차 골절 선에 의한 종골 후방 조면 골편의 정복은 후방 관절 소면의 정복 및 종골 각도 회복을 포함한 해부학적 복원을 위하여 매우 중요하 다. 따라서 수술 과정 중 종골 후방 조면 골편의 정확한 정복이 가장 먼저 이루어져야 하겠으며, 이를 위한 효과적 인 정복 술기에 대한 연구가 더 필요하겠다.
References
1) Benirschke SK, Mayo KA, Sangeorzan BJ, Hansen ST:
Results of operative treatment of calcaneal fractures. In:
Tscherne H, Schatzker J ed. Major fractures of the pilon, the talus and the calcaneus. Berlin, Springer-Verlag: 215- 227, 1993.
2) Carr JB, Hansen ST, Benirschke SK: Subtalar dis- traction bone block fusion for late complications of os calcis fractures. Foot Ankle, 9: 81-86, 1988.
3) James ET, Hunter GA: The dilemma of painful old os calcis fractures. Clin Orthop Relat Res, (177): 112-115, 1983.
4) Kitaoka HB, Schaap EJ, Chao EY, An KN: Displaced intra-articular fractures of the calcaneus treated non- operatively. Clinical results and analysis of motion and ground-reaction and temporal forces. J Bone Joint Surg Am, 76: 1531-1540, 1994.
5) Zwipp H, Tscherne H, Thermann H, Weber T: Osteo- synthesis of displaced intraarticular fractures of the calca- neus. Results in 123 cases. Clin Orthop Relat Res, (290):
76-86, 1993.
6) Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra- articular calcaneal fractures: a prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am, 84:
1733-1744, 2002.
7) Giachino AA, Uhthoff HK: Intra-articular fractures of the calcaneus. J Bone Joint Surg Am, 71: 784-787, 1989.
8) Ibrahim T, Rowsell M, Rennie W, Brown AR, Taylor GJ, Gregg PJ: Displaced intra-articular calcaneal frac- tures: 15-year follow-up of a randomised controlled trial of conservative versus operative treatment. Injury, 38: 848- 855, 2007.
9) Järvholm U, Körner L, Thorén O, Wiklund LM:
Fractures of the calcaneus. A comparison of open and closed treatment. Acta Orthop Scand, 55: 652-656, 1984.
10) Parmar HV, Triffitt PD, Gregg PJ: Intra-articular frac- tures of the calcaneum treated operatively or conserva- tively. A prospective study. J Bone Joint Surg Br, 75:
932-937, 1993.
11) Thordarson DB, Krieger LE: Operative vs. nonoperative treatment of intra-articular fractures of the calcaneus: a prospective randomized trial. Foot Ankle Int, 17: 2-9, 1996.
12) Randle JA, Kreder HJ, Stephen D, Williams J, Jaglal S, Hu R: Should calcaneal fractures be treated surgically?
A meta-analysis. Clin Orthop Relat Res, 377: 217-227, 2000.
13) Myerson M, Quill GE Jr: Late complications of frac- tures of the calcaneus. J Bone Joint Surg Am, 75: 331- 341, 1993.
14) Richards PJ, Bridgman S: Review of the radiology in randomised controlled trials in open reduction and internal fixation (ORIF) of displaced intraarticular calcaneal frac- tures. Injury, 32: 633-636, 2001.
15) Sanders R, Vaupel ZM, Erdogan M, Downes K: Opera- tive treatment of displaced intraarticular calcaneal frac- tures: long-term (10-20 Years) results in 108 fractures us- ing a prognostic CT classification. J Orthop Trauma, 28:
551-563, 2014.
16) Hammesfahr JF: Surgical treatment of calcaneal fractures.
Orthop Clin North Am, 20: 679-689, 1989.
17) Leung KS, Yuen KM, Chan WS: Operative treatment of displaced intra-articular fractures of the calcaneum. Medium- term results. J Bone Joint Surg Br, 75: 196-201, 1993.
18) Sanders R, Fortin P, DiPasquale T, Walling A: Opera- tive treatment in 120 displaced intraarticular calcaneal frac- tures. Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res, (290): 87-95, 1993.
19) Sanders R: Current concepts review. Displaced intra-artic- ular fractures of the calcaneus. J Bone Jt Surg, 82: 225- 250, 2000.
20) Miric A, Patterson BM: Pathoanatomy of intra-articular fractures of the calcaneus. J Bone Joint Surg Am, 80:
207-212, 1998.
21) Carr JB: Surgical treatment of the intra-articular calca- neus fracture. Orthop Clin North Am, 25: 665-675, 1994.
22) Ogut T, Ayhan E, Kantarci F, Unlu MC, Salih M:
Medial fracture line significance in calcaneus fracture. J Foot Ankle Surg, 50: 517-521, 2001.
23) Rammelt S, Zwipp H: Calcaneus fractures: facts, con- troversies and recent developments. Injury, 35: 443-461, 2004.
24) Eastwood DM, Gregg PJ, Atkins RM: Intra-articular fractures of the calcaneum. Part I: pathological anatomy and classification. J Bone Joint Surg Br, 75: 183-188, 1993.
25) Tennent TD, Calder PR, Salisbury RD, Allen PW, Eastwood DM: The operative management of displaced intra-articular fractures of the calcaneum: a two-centre study using a defined protocol. Injury, 32: 491-496, 2001.
26) Benirschke SK, Sangeorzan BJ: Extensive intraarticular fractures of the foot. Surgical management of calcaneal fractures. Clin Orthop Relat Res, (292): 128-134, 1993.
Copyright ⓒ 2016 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
https://doi.org/10.12671/jkfs.2016.29.4.233
전위성 관절내 종골 골절의 관혈적 정복 시 종골 후방 조면 골편 정복의 중요성
박홍기 ⋅백종륜⋅최장석⋅이상진⋅백제원
가천대 길병원 정형외과
목 적: 전위성 관절내 종골 골절의 치료 시 성공적인 관혈적 정복을 위한 요소로, 일차 골절 선에 의한 종골 후방 조면 골편 정복의 중요성을 확인하고자 하였다.
대상 및 방법: 2010년 1월부터 2015년 12월까지 전위성 관절내 골절로 관혈적 정복을 시행한 90예의 환자를 대상으로, 술 후 3개월 후방 조면 골편의 외측 전위 정도와 건측과의 종골 길이 및 높이 차이를 측정하여 종골 후방 조면 골편의 정복 상태를 평가하였다. 골절부 간격 및 층 형성 정도, Böhler 각과 Gissane 각의 건측과의 차이를 측정하여 각각 후방 관절 소면 정복 상태와 종골 각도 회복을 평가하였다.
결 과: 후방 조면 골편의 정복 상태를 평가한 3가지 항목과 골절부 간격 및 층 형성의 상관계수는 각각 r=0.538, 0.467, r=0.505, 0.456, r=0.518, 0.493이었으며, 건측과의 두 가지 종골 각 차이와의 상관계수는 각각 r=0.647, 0.579, r=0.684, 0.630, r=0.670, 0.628이었다. 모든 항목 간의 p-value는 <0.01로 통계적으로 유의미한 상관관계를 보였다.
결 론: 종골 후방 조면 골편의 정확한 정복은 후방 관절 소면 정복 및 종골 각도 회복을 포함한 종골 체부의 해부학적 정복을 위한 중요한 요소로 생각된다.
색인 단어: 종골, 관절내 골절, 후방 조면, 해부학적 정복
접수일 2016. 5. 10 수정일 2016. 6. 8 게재확정 2016. 7. 1 교신저자 박홍기
21565, 인천시 남동구 남동대로 774번길 21, 가천대 길병원 정형외과 Tel 032-460-3384, Fax 032-423-3384, E-mail [email protected]
241