J Korean Ophthalmol Soc 2013;54(12):1939-1944 pISSN: 0378-6471 eISSN: 2092-9374 http://dx.doi.org/10.3341/jkos.2013.54.12.1939
= 증례보고 =
유리체강내 덱사메타존 임플란트 삽입 후 발생한 급성 안내염 1예
한현철⋅방종욱⋅염정훈⋅김진형⋅이도형⋅이종현 인제대학교 의과대학 일산백병원 안과학교실
목적: 망막분지정맥폐쇄에 합병된 황반부종으로 유리체강내 덱사메타존 임플란트(Ozurdex®) 삽입 후 발생한 급성 안내염을 보인 1예를 보고하고자 한다.
증례요약: 우안 망막분지정맥폐쇄에 합병된 황반부종으로 인한 시력저하를 주소로 63세 남자 환자가 내원하였다. 유리체강내 베바시주 맙 주입술을 시행하였으나 황반부종은 호전을 보이지 않았고, 2개월 후 유리체강내 덱사메타존 임플란트 삽입술을 시행하였다. 삽입 4일째 심한 시력저하로 내원하였고 세극등현미경 검사에서 경한 충혈, 전방축농, 전방내의 염증, 유리체 혼탁 소견을 보여 급성 안내염 진단 하에 유리체절제술 및 유리체강내 항생제 주입술, 덱사메타존 임플란트 제거술, 수정체유화술을 시행하였으며 치료 후 안저소견 및 염증반응은 잘 조절되었다. 유리체액 배양검사에서는 coagulase negative staphylococcus가 검출되었다.
결론: 유리체강내 덱사메타존 임플란트를 삽입한 후 발생한 급성 안내염은 스테로이드의 항염증 작용으로 인하여 심한 충혈이나 통증 없이 비특이적인 양상을 보일 수 있으므로 시술 후 안내염의 발생을 관찰하는데 있어 주의를 요한다.
<대한안과학회지 2013;54(12):1939-1944>
■Received: 2013. 5. 25. ■ Revised: 2013. 7. 31.
■Accepted: 2013. 10. 18.
■Address reprint requests to Jong Hyun Lee, MD
Department of Ophthalmology, Inje University Ilsan Paik Hospital, #170 Juhwa-ro, Ilsanseo-gu, Goyang 411-706, Korea Tel: 82-31-910-7240, Fax: 82-31-911-7241
E-mail: [email protected]
유리체강내 주입술은 전신 독성을 최소화 하면서 안구 내에서 약물이 치료 농도에 도달하게 하는 효과적인 방법 으로 다른 여러 약물주입 경로에 비해 많은 장점이 있어 후안부의 여러 질환에 대한 약물치료로서 널리 사용되는 술기이다.1,2 특히 당뇨망막병증, 망막정맥폐쇄, 포도막염, Irvine-Gass 증후군 등의 다양한 안과질환으로부터 발생 한 황반부종의 경우 유리체강내 트리암시놀론 주입술이 우 수한 치료성적과 비교적 안전한 시술로 알려져 있어 최근 까지 널리 시행되고 있다.3-7 그러나 망막박리, 유리체 출 혈, 트리암시놀론 결정의 황반부 침착, 가성전방축농, 비감 염성 안내염과 감염성 안내염, 중심망막동맥폐쇄, 일시적 안 압상승, 백내장의 발생, 스테로이드 녹내장 등이 유리체강내 트리암시놀론 주입술의 합병증으로 보고되어 있다.8-13최근 개발된 덱사메타존 임플란트(Ozurdex®, Allergan, Irvine, CA)는 유리체강내 삽입 후 수용성의 강력한 부신피질호르 몬인 덱사메타존을 저용량으로 수개월 동안 서서히 방출하 는 생분해성 삽입물로 기존 유리체강내 트리암시놀론 주입
술에 비해 적은 빈도의 안압상승과 백내장 발생을 보이며, 망막정맥폐쇄에 있어 시력의 호전과 유의한 황반부종의 감 소를 보이고 있어 시술의 증가가 기대되는 바이다.14,15
저자들은 망막분지정맥폐쇄에 합병된 황반부종으로 유 리체강내 덱사메타존 임플란트(Ozurdex®)를 삽입한 후 급 성 안내염을 보인 1예를 경험하였기에 문헌고찰과 함께 임 상결과를 보고하는 바이다.
증례보고
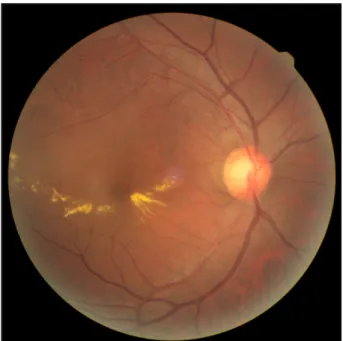
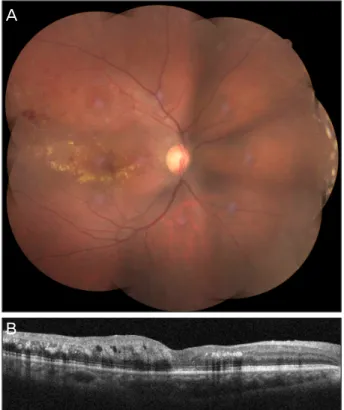
63세 남자가 1년 전부터 발생한 우안 시력저하로 타 병 원에서 망막분지정맥폐쇄에 합병된 황반부종을 진단 받은 후 유리체강내 베바시주맙(Avastin®, Genentech Inc., San Francisco, CA) 주입술을 권유 받고 본원에 내원하였다. 기 저질환이나 안과수술의 병력은 없었고, 최대교정 시력은 우 안 0.6, 좌안 1.0 안압은 우안 10 mmHg, 좌안 13 mmHg이 었으며, 세극등현미경 검사에서는 특이소견을 보이지 않았 다. 우안의 안저소견에서 황반부 주변의 경성 삼출물과 위 쪽 혈관궁과 황반부 사이의 점상출혈을 보이는 망막분지정 맥폐쇄의 소견을 보였고(Fig. 1) 빛간섭단층촬영에서 황반 부종이 합병된 소견을 보였다(Fig. 2A). 유리체강내 베바 시주맙 주입술을 시행하였으나 황반부종은 호전을 보이지 않아(Fig. 2B), 2개월 뒤 시술에 대한 설명과 동의 후 유 리체강내 덱사메타존 임플란트 삽입술을 시행하였다. 모
Figure 1. Initial fundus photograph. The right eye shows
branch retinal vein occlusion (BRVO) with macular edema.A B
Figure 3. Slit lamp photograph of the right eye shows hypopyon in the anterior chamber (A). Ultrasonogram of the right eye shows
vitreous opacity (B).A
B
Figure 2. The baseline optical coherence tomography (OCT)
of the right eye shows macular edema (A). Despite intravitreal bevacizumab injection, macular edema did not improve at one month after injection (B).든 유리체강내 시술은 외래 수술실에서 0.5% 프로파라카 인(Alcaine®, Alcon lab., Fort Worth, TX) 점안마취 하에 멸균포와 멸균개검기를 이용한 무균상태에서 멸균장갑과 마스크를 착용하고 5% 포비돈 소독 후 시행하였다. 시술 직 후 0.3% 가티플록사신(Gatiflo®, Handok, Chungbuk, Korea) 을 바로 점안해 주었고, 하루 4회씩 3일간 유지하도록 하였 다. 유리체강내 삽입술 시행 4일 뒤 환자는 우안의 심한 시 력저하와 경한 통증을 호소하며 내원하였다. 시력은 광각유 상태로 저하되어 교정되지 않았고 세극등현미경 검사에서 경한 결막충혈과 전방내 염증세포(++++), 방수흐림과 섬 유소, 전방축농이 관찰되었다(Fig. 3A). 안구 초음파검사에
서유리체강내를 채우는 중등도의 음파반향이 나타나 유리 체 혼탁을 짐작할 수 있었고 안저는 관찰되지 않았다(Fig.
3B). 감염성 안내염 의심 하에 당일 유리체절제술 및 유리 체강내 항생제 주입술(vancomycin 1.0 mg/0.1 ml, cefta- zidime 2.0 mg/0.1 ml), 전방세척을 시행하였다. 유리체절 제술 시 얻어진 검채로 유리체액 배양검사를 시행하였고 coagulase negative staphylococcus가 검출되었다. 수술 후 0.5% 목시플록사신(Vigamox®, Alcon lab., Fort Worth, TX)과 1% 프레드니솔론(Predforte®, Allergan, Irvine, CA) 점안액을 2시간마다 점안하게 하였고 24시간 간격으 로 유리체강내 항생제 주입술을 3회 추가로 시행하였으며, 목시플록사신(Avelox®, Chongkundang, Cheonan, Korea) 400 mg을 하루 한 번 정맥내로 전신투여하였다. 수술 3일 후 전방 및 유리체의 염증반응이 호전되어 안저관찰이 가
A B
Figure 4. Fundus appearance during vitrectomy. Vitreous fibrosis and opacity was removed through previous vitrectomy (A). The
implant was easily removed by the vitreotome tip (B).A
B
Figure 5. Fundus photograph (A) and optical coherence to-
mography (B) of the right eye, one month after treatment shows the macular edema much improved.능하였으나 안내염 발생 전에는 관찰되지 않았던 심한 후 낭하백내장 소견을 보여 2차 유리체절제술 및 유리체강내 항생제 주입술, 덱사메타존 임플란트 제거술, 수정체유화술 및 인공수정체 삽입술을 시행하였다(Fig. 4A, B). 수술 1개 월 뒤 우안 교정 시력은 0.1로 호전되었고 전방 및 유리체 의 염증반응은 보이지 않았다. 안저소견에서 황반부 주변의 경성 삼출물과 위쪽 혈관궁과 황반부 사이의 점상출혈은 여전히 관찰되었으나 빛간섭단층촬영에서 황반부종은 상당
히 호전된 소견을 보였다(Fig. 5A, B).
고 찰
덱사메타존 임플란트는 22게이지 전용 분사기를 사용하 여 평면부를 통해 유리체강내로 삽입되는 장치로 생분해성 폴리머 매트릭스(D, L-lactide-co-glycolide)에 0.7 mg 의 덱사메타존을 중합시켜 유리체강내로 삽입 후 수개월 동안 유지되면서 저용량의 덱사메타존을 서서히 분출하게 된다. 2009년 망막정맥폐쇄로 인한 황반부종 환자에서 그 효과가 입증되어 미국 식약청의 허가를 받았고16무작위 대 조군 다기관 제3상 임상시험(GENEVA study14) 연구 결과 에서는 허위주사 군과 비교 시 덱사메타존 임플란트 군에 서 시력호전에 걸리는 기간이 유의하게 짧았으며 3줄 이상 의 시력호전을 보일 확률이 유의하게 크고 심각한 시력상 실은 유의하게 적게 나타나는 것으로 보고하였다. 본 증례 에서는 안내염으로 인해 덱사메타존 임플란트를 삽입 후 4일만에 제거하였으나 기존 유리체강내 베바시주맙 주입 술에도 호전을 보이지 않았던 황반부종이 상당한 호전을 보였다. 비록 안내염으로 인해 시행한 유리체 절제술이 황 반부종을 어느 정도 낮추는데 기여했다 하더라도 망막정 맥폐쇄에 있어 덱사메타존 임플란트의 효과가 기대되는 바 이다.
Pilli et al17은 항혈관내피성장인자(Anti-VEGF) 주입 술 후 안내염의 발생빈도는 0.029%라고 보고하였고, 최 근 McCannel18은 0.02-0.05%로 항혈관내피성장인자 주 입술 후 안내염의 발생빈도는 낮다고 보고하였다. GENEVA study14에서 덱사메타존 임플란트 삽입 후 주요한 합병증으 로는 안구통, 안압상승, 전방내 염증, 백내장, 유리체 출혈, 망막박리 등을 보고하였으나 안내염의 발생은 보고하지 않
았으며 최근에서야 Marchino et al19이 덱사메타존 임플란 트 삽입 후 Alloiococcus otitidis가 동정된 급성 안내염을 최초로 보고하였다. 이러한 결과는 덱사메타존이 안내염 발 생 위험에 안전한 약물이라기 보다는 이전 연구에서 모집 단의 수가 크지 않았고 약제가 허가되어 시행된 지 얼마 되 지 않았기 때문이라 생각하며 앞으로 시술이 증가함에 따라 안내염의 발생 빈도도 비례하여 늘어날 것이라 예상된다.
감염성 안내염의 원인이 되는 균은 환자의 눈꺼풀과 결 막 등 눈 주위에 상재하는 정상 세균총이다.20-22그 중 co- agulase negative staphylococcus 가장 흔한 원인균으로 안 구표면에서 가장 흔하게 동정되며, 본 증례에서도 유리체액 배양검사에서 coagulase negative staphylococcus가 검출 되었다. 따라서 감염성 안내염의 발생을 최소화하기 위해 가장 중요한 사항은 주사부위 주위를 무균상태로 유지하는 것이며23,24 2004년 Aiello et al2은 유리체강내 주입술 시 지켜야 할 사항으로 첫째, 안검 및 주위 부속기에 기구가 닿지 않도록 주의하여 무균적 조작, 둘째, 포비돈으로 안구 주위 피부와 결막 소독, 셋째, 멸균소독된 개검기 이용, 넷 째, 전방천자를 하지말 것을 권고하였고, 본원에서도 권고 사항에 따라 멸균포와 멸균개검기, 멸균장갑, 마스크, 5%
포비돈을 사용하여 무균적 환경에서 유리체강내 주입술을 시행하고 있다. 일반적인 유리체강내 약물, 항혈관내피성장 인자, 트리암시놀론 주입술은 30게이지를 사용하는데 반해 덱사메타존 임플란트의 경우 22게이지의 전용분사기를 통 하여 삽입된다. 때문에 창상의 크기가 크고, 이로 인한 창상 부위 누출과 벌어짐이 발생할 가능성이 높다고 추정된다.
본 증례에서 발생한 안내염도 눈꺼풀과 결막 주변의 상재 균인 coagulase negative staphylococcus가 창상을 통해 유 입되어 감염을 일으켰을 것으로 생각하며, 안내염을 최소화 하기 위해 시술 전 포비돈으로 안구주위 피부와 결막을 철 저히 소독하고 외래보다는 수술실에서의 시술이 권유된다.
Bucher et al25은 동물실험모델을 통해 유리체강내 주입 된 트리암시놀론이 안구 내 국소적인 면역반응을 억제하여 감염성 안내염을 일으키는 세균의 문턱을 낮춤으로써 감염 에 대한 감수성을 증가시키고 초기 안내염의 증상 발현을 지연시키며, 치료하지 않을 경우 더 심한 유리체내 염증반 응을 유발시킨다고 보고하였다. 본 증례의 경우 상재균인 coagulase negative staphylococcus가 원인균으로 다른 종 류의 균에 비하여 지연되고 경한 안내염의 증상을 보였을 수 있지만, 덱사메타존 임플란트도 트리암시놀론과 같은 부 신피질호르몬이기 때문에 스테로이드의 항염증작용으로 인 하여 상재균에 의한 감염의 기회가 증가되고 초기 증상 발 현을 지연시키며 증상의 양상도 비특이적으로 나타날 수 있다.
유리체절제술의 경우는 유리체강내에서 배양을 위한 가 검물을 충분히 채취할 수 있고, 유리체강내 염증산물을 제거 함과 동시에 세균독소를 제거할 수 있으며, 유리체강내로 항 생제 주입을 용이하게 하여 항생제가 골고루 분포되게 함으 로써 그 효과를 극대화 시켜주는 등의 장점이 있다. Puliafito et al26과 Laatikainen and Tarkkanen et al27은 안내염 진 단 후 24시간 내에 유리체절제술을 시행한 군에서 시력예 후가 좋았다고 보고하였다. 최근 Marchino et al19의 보고 에 따르면 유리체강내에서 서서히 분출되는 삽입물과 관련 된 감염성 안내염의 경우 감염균이 이러한 삽입물 내에 존 재하면서 항생제에 대한 반응을 더디게 만들 수 있으므로 안내염의 효과적인 치료를 위해서는 유리체절제술을 통한 삽입물의 제거가 필요하다고 주장하였다. 본 증례에서도 진 단 후 경험적 광범위 항생제를 사용한 즉각적인 유리체강 내 항생제 주입술이 시행되었고 내원 당일 유리체절제술을 시행하여 수술 3일 후 전방 및 유리체의 염증반응이 호전되 어 안저관찰이 가능한 비교적 좋은 결과를 보였으며, 2차 수술 시 삽입하였던 덱사메타존 임플란트를 제거하여 안내 염을 효과적으로 조절할 수 있었다.
본 증례는 망막정맥폐쇄로 인한 황반부종에 우수한 치료 효과를 보여 앞으로 시술의 증가가 기대되는 유리체강내 덱사메타존 임플란트 삽입 후 발생한 안내염의 국내 최초 보고임에 의의가 있다.
결론적으로 유리체강내 덱사메타존 임플란트 삽입 후에 는 스테로이드의 항염증작용으로 인하여 감염의 기회가 늘 어날 수 있고 안내염 증상 발현까지의 기간이 연장되거나 증상의 양상이 비특이적으로 나타나 진단이 어려울 수 있 으므로 초기에 주의 깊은 추적관찰이 필요하며, 안내염이 의심이 된다면 즉각적인 진단을 위하여 가검물을 채취하여 미생물검사를 시행하고, 조기에 유리체강내 항생제 주입술 과 유리체절제술을 시행하는 것이 예후에 도움이 될 것이 라고 생각한다.
REFERENCES
1) Jager RD, Aiello LP, Patel SC, Cunningham ET Jr. Risk of intra- vitreous injection: A comprehensive review. Retina 2004;24:676-98.
2) Aiello LP, Brucker AJ, Chang S, et al. Evolving guidelines for in- travitreous injections. Retina 2004;24(5 Suppl):S3-19.
3) Sutter FK, Simpson JM, Gillies MC. Intravitreal triamcinolone for diabetic macular edema that persists after laser treatment: three- month efficacy and safety results of a prospective, randomized, double-masked, placebo-controlled clinical trial. Ophthalmology 2004;111:2044-9.
4) Ip MS, Gottlieb JL, Kahana A, et al. Intravitreal triamcinolone for the treatment of macular edema associated with central retinal vein occlusion. Arch Ophthalmol 2004;122:1131-6.
5) Antcliff RJ, Spalton DJ, Stanford MR, et al. Intravitreal tri- amcinolone for uveitic cystoid macular edema: An optical coher- ence tomography study. Ophthalmology 2001;108:765-72.
6) Sutter FK, Gillies MC. Intravitreal triamcinolone for radiation in- duced macular edema. Arch Ophthalmol 2003;121:1491-3.
7) Spaide RF, Sorenson J, Maranan L. Combined photodynamic ther- apy with verteporfin and intravitreal triamcinolone acetonide for choroidal neovascularization. Ophthalmology 2003;110:1517-25.
8) Vasconcelos-Santos DV, Nehemy PG, Schachat AP, Nehemy MB.
Secondary ocular hypertension after intravitreal injection of 4 mg of triamcinolone acetonide: incidence and risk factors. Retina 2008;28:573-80.
9) Jung JW, Nam DH, Shyn KH. The complications after intravitreal injection of triamcinolone acetonide. J Korean Ophthalmol Soc 2007;48:55-62.
10) Moshfeghi DM, Kaiser PK, Scott IU, et al. Acute endophthalmitis following intravitreal triamcinolone acetonide injection. Am J Ophthalmol 2003;136:791-6.
11) Gillies MC, Kuzniarz M, Craig J, et al. Intravitreal triamcinolone induced elevated intraocular pressure is associated with the devel- opment of posterior subcapsular cataract. Ophthalmology 2005;
112:139-43.
12) Rhee DJ, Peck RE, Belmont J, et al. Intraocular pressure alterations following intravitreal triamcinolone acetonide. Br J Ophthalmol 2006;90:999-1003.
13) Nelson ML, Tennant MT, Sivalingam A, et al. Infectious and pre- sumed noninfectious endophthalmitis after intravitreal triamcinolone acetonide injection. Retina 2003;23:686-91.
14) Kuppermann BD, Blumenkranz MS, Haller JA, et al. Dexamethasone DDS Phase II Study Group. Randomized controlled study of an in- travitreous dexamethasone drug delivery system in patients with persistent macular edema. Arch Ophthalmol 2007;125:309-17.
15) Haller JA, Bandello F, Belfort R Jr, et al. Randomized, sham-con- trolled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology 2010;117:1134-46.e3.
16) Chan A, Leung LS, Blumenkranz MS. Critical appraisal of the
clinical utility of the dexamethasone intravitreal implant (Ozurdex) for the treatment of macular edema related to branch retinal vein occlusion or central retinal vein occlusion. Clin Ophthalmol 2011;
5:1043-9.
17) Pilli S, Kotsolis A, Spaide RF, et al. Endophthalmitis associated with intravitreal anti-vascular endothelial growth factor therapy in- jections in an office setting. Am J Ophthalmol 2008;145:879-82.
18) McCannel CA. Meta-analysis of endophthalmitis after intravitreal injection of anti-vascular endothelial growth factor agents: causa- tive organisms and possible prevention strategies. Retina 2011;
31:654-61.
19) Marchino T, Vela JI, Bassaganyas F, et al. Acute-onset endoph- thalmitis caused by alloiococcus otitidis following a dexamethasone intravitreal implant. Case Rep Ophthalmol 2013;4:37-41.
20) Speaker MG, Milch FA, Shah MK, et al. Role of external bacterial flora in the pathogenesis of acute postoperative endophthalmitis.
Ophthalmology 1991;98:639-50.
21) Ta CN. Minimizing the risk of endophthalmitis following intra- vitreous injections. Retina 2004;24:699-705.
22) de Caro JJ, Ta CN, Ho HK, et al. Bacterial contamination of ocular surface and needles in patients undergoing intravitreal injections.
Retina 2008;28:877-83.
23) Kreissig I, Degenring RF, Jones JB. [Intravitreal triamcinolone acetonide: complication of infectious and sterile endophthalmitis].
Ophthalmology 2006;103:30-4.
24) Westfall AC, Osborn A, Kuhl D, et al. Acute endophthalmitis incidence. Arch Ophthalmol 2005;123:1075-7.
25) Bucher RS, Hall E, Reed DM, et al. Effect of intravitreal tri- amcinolone acetonide on susceptibility to experimental bacterial enodphthalmitis and subsequent response to treatment. Arch Ophthalmol 2005;123:649-53.
26) Puliafito CA, Baker AS, Haaf J, Foster CS. Infectious endophthalmitis.
Review of 36 cases. Ophthalmology 1982;89:921-9.
27) Laatikainen L, Tarkkanen A. Early vitrectomy in the treatment of post-operative purulent endophthalmitis. Acta Ophthalmol (Copenh) 1987;65:455-60.
=ABSTRACT=
A Case of Acute Endophthalmitis Following a Dexamethasone Intravitreal Implant
Hyun Cheol Han, MD, Jong Wook Bang, MD, Jung Hoon Yum, MD, Jin Hyoung Kim, MD, Do Hyung Lee, MD, PhD, Jong Hyun Lee, MD
Department of Ophthalmology, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
Purpose: To report a case of acute endophthalmitis after a dexamethasone (Ozurdex®) intravitreal implant for macular edema (ME) secondary to branch retinal vein occlusion (BRVO).
Case summary: A 63-year-old male patient presented with decreased vision in the right eye due to ME secondary to BRVO. The patient was treated with an intravitreal bevacizumab injection, but ME did not improve. Two months after the injection, dexamethasone (Ozurdex®) intravitreal implantation was performed. Four days after the implantation, the patient visited our clinic complaining of severe visual disturbance. Slight conjunctival injection was observed and inflammatory cells and hypopyon were found in the anterior chamber. Fundus was not visible due to vitreous opacity. The patient was presumed to have acute endophthalmitis. Vitrectomy, intravitreal antibiotics injection, dexamethasone implant removal and phacoemulsification were performed. After treatment, the patient’s fundus markedly improved, the inflammatory re- sponse was controlled and coagulase negative staphylococcus was detected from vitreous culture.
Conclusions: In cases of intravitreal dexamethasone implant associated with acute endophthalmitis, careful examination for diagnosis of endophthalmitis is recommended because the patient may not present with severe ocular pain and in- jection due to anti-inflammatory effect of corticosteroid.
J Korean Ophthalmol Soc 2013;54(12):1939-1944
Key Words: Branch retinal vein occlusion, Dexamethasone implant, Endophthalmitis, Intravitreal injection, Macular edema
Address reprint requests to Jong Hyun Lee, MD
Department of Ophthalmology, Inje University Ilsan Paik Hospital
#170 Juhwa-ro, Ilsanseo-gu, Goyang 411-706, Korea
Tel: 82-31-910-7240, Fax: 82-31-911-7241, E-mail: [email protected]