118
In 1937, Eagle [1] coined the term stylalgia to describe the pain associated with Eagle’s syndrome. Eagle’s syndrome is the term given for the symptomatic elongation of the styloid process or mineralization of the stylohyoid or stylomandibular ligament [2]. Eagle considered any styloid process longer than 25 mm to be elongated and usually responsible for Eagle’s syndrome [2].
He further described the condition as atypical facial neuralgia and reported various associated symptoms, such as the sensa- tion of a foreign body lodged in the throat; difficulty and pain during swallowing; throat pain; pain on turning the head; pain in the infraorbital, infratemporal, ear, and occipital areas; pain on wide opening of mouth; headache; tinnitus; and vertigo [2].
As diagnosis is not very easy, the number of total cases has been underestimated in the population [3]. Due to the variable and
non-specific nature of symptoms, patients seek treatment in several different clinics, for example, otolaryngology, neurology, neurosurgery, psychiatry and dentistry clinics [4]. Eagle’s synd- rome is considered a rare disease. The prevalence of styloid process elongation is reported to be 4%; however, only a small subgroup of these patients becomes symptomatic (between 4%
and 10.3%), with higher frequency in women older than 30 years [5]. The basic symptoms are recurrent neck, throat, and hemifacial pain; the sensation of a foreign body in the throat;
dysphagia; a change in voice; otalgia; and pain that radiates to the upper extremities [6]. The main treatment approach involves partial excision of the styloid process [7].
Case Report
A 58-year-old woman visited Chosun University Dental Hospital with foreign body sensation and pain in the oropha- ryn geal area during swallowing, coupled with a headache and radiating pain to the ear. Her symptoms had started 6 months prior. She was able to palpate the tubercle in the oropharynx.
Before she came to our department, she had received physical ORAL BIOLOGY RESEARCH 2014; 38(2): 118-121
Resection of calcified elongated styloid process (Eagle's syndrome) with Piezosurgery: A case report and review of literature
Seong-Yong Moon, Su-Gwan Kim*, Kyung-Seop Lim, Seung-Min Shin, Cheol-Man Kim
Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University, Gwangju, Korea
ABSTRACT
Eagle’s syndrome is the term given for the symptomatic elongation of the styloid process or mineralization of the stylohyoid or stylomandibular ligament. The basic symptoms are recurrent neck, throat, and hemifacial pain; sensation of a foreign body in the throat; dysphagia; change in voice; otalgia; and pain radiating to the upper extremities. Treatment usually involves a medical approach (e.g., administration of non-steroidal anti-inflammatory medications or even carbamazepine) or surgical intervention.
The main treatment approach involves partial excision of the styloid process. A 58-year-old woman visited Chosun University Dental Hospital with a foreign body sensation and pain in the oropharyngeal area during swallowing, as well as a headache and radiating pain to the ear. Operation was performed under general anesthesia via an intra-oral approach with resection via Piezosurgery. The patient had no postoperative complications and was free of symptoms for 9 months after the operation.
Key Words: Eagle syndrome, Elongated styloid process syndrome, Styloid-stylohoid syndrome Case Report
Received Mar 3, 2014; Revised version received Apr 28, 2014 Accepted May 21, 2014
Corresponding author: Su-Gwan Kim
Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University, 309 Pilmun-daero, Dong-gu, Gwangju 501- 759, Korea
Tel: 82-62-220-3819, Fax: 82-62-228-7316 E-mail: [email protected]
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Seong-Yong Moon et al.
119 treatment and was also prescribed medications, although she
did not feel that her symptoms had improved. On clinical examination, she had pain during palpation of the firm, round bony tubercle in the submandibular area. She did not have a previous history of tonsillectomy or head and/or neck trauma.
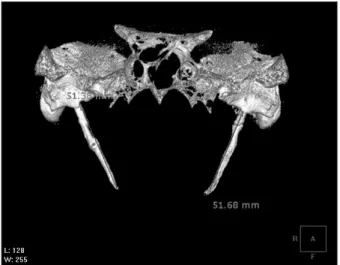
Panoramic examination revealed an elongated and calcified styloid process. She was given a preliminary diagnosis of Eagle’s syndrome and underwent a three-dimensional computed tomography. In the computed tomography (CT) view, the styloid process was elongated to the medial surface of the mandibular ramus and measured approximately 51 mm on both sides (Fig. 1).
The operation was performed under general anesthesia via an intra-oral approach using a Dingman retractor. Two incisions
were made at the pteryogomandibular raphe area. The tensor and elevator of the palatal veli muscles were retracted with the two retractors, for exposing the styloid process. And then, periosteal incision was made on the periosteum at the tip of the styloid process. Then, the periosteum was stripped from the tip to the base for resection of the styloid process, approximately 34 mm. The styloid process was resected using Piezosurgery (Fig. 2). The removed styloid process was approximately 33 mm in length, compared to 51 mm before surgery (Fig. 3). After resection of the elongated styloid process, the palatal mucosa was sutured with Vicryl 3-0. The patient did not have any postoperative complications and was free from her symptoms.
She had no discomfort and underwent another 3-dimensional (3D)-CT 9 months after the surgery (Fig. 4).
Discussion
Eagle documented that the average length of the styloid ranges from 2.5 to 3.0 cm [2]. Kaufman et al. [3] reported that 30 mm is the upper limit for a normal styloid process. Mansour and Young [8] concluded that a diagnosis of an elongated styloid process could be made when it is longer than 40 mm. In presented case, all of the styloid processes in Eagle’s syndrome were longer than 40 mm, with the maximum length measured at approximately 51 mm. After resection, the length was approximately 17 mm. The incidence of Eagle’s syndrome has been reported to be between 1.4% and 30%, with more frequent incidence in women than in men [3].
The exact cause of the elongation of the styloid process Fig. 1. In the 3-dimensional computed tomography view, the elon-
gated styloid process measured approximately 52 mm on both sides.
Fig. 2. Exposure of the elongated styloid process and resection with Piezosurgery. This picture is published with the patient’s consent.
Fig. 3. The resected styloid process. This picture is published with the patient’s consent.
120
Resection of calcified elongated styloid process (Eagle’s syndrome) with Piezosurgery
is not clear. Steinman [9] reported 3 pathogeneses of the calcification of the styloid process. The first is that mechanical stimulation to the pharynx promotes ossification of the tip of the styloid process. The second is that mechanical stimulation causes ossification starting from the inside of the ligament of the styloid process. The third explains the pathogenesis as a congenital ossification of the ligament of the styloid process from birth.
Eagle proposed two types of the syndrome. The first type is the classic type, which is characterized by pain secondary to stimulation of cranial nerves V (trigeminal), VII (facial), IX (glossopharyngeal), and X (vagus); this type is often observed subsequent to a tonsillectomy [2]. Eagle theorized that these patients develop scarring near the styloid apex that subsequently compresses or stretches nerve structures near the styloid process [2]. The second type is the carotid artery type, which occurs when the styloid process becomes involved with the carotid nerve plexus and causes a foreign body sensation in the pharynx as well as neck pain on rotation of the head.
This type is not dependent on previous pharyngeal surgery. It has been suggested that mechanical irritation and stimulation of the sympathetic plexus in the walls of the external and/or internal carotid arteries by the styloid tip or ossified ligament provide a diverse array of symptoms [2]. Langlais et al. [10]
classified this syndrome into the 3 following types, according to the form and characteristic of elongation: type I (elongated) indicates continuous elongation of more than 25 mm; type II
(pseudo-articulated) refers to a combined stylomandibular ligament and styloid process or stylohyoid ligament and styloid process by pseudoarticulation; and type III (segmented) refers to a discontinuous segment of the styloid process or calcified ligament.
Eagle’s syndrome is characterized by symptoms involving recurrent throat pain; pharyngeal foreign body sensation;
dysphagia; neck pain and reduction in neck mobility when turning to the affected side; and painful limitation of mandi- bular opening and lateral excursion [11]. Differential diagnoses for Eagle’s syndrome should include all conditions causing cervicofacial pain. These involve temporomandibular disorders; trigeminal, sphenopalatine, glossopharyngeal, and upper laryngeal nerve neuralgias; myofascial pain; mastoiditis;
otitis; temporal arteritis; dental pain (especially involving the third molars); chronic tonsillitis or pharyngitis; submandibular sialadenitis or sialolithiasis; esophageal diverticulosis; benign or malignant neoplastic disease; true pharyngeal foreign bodies; neoplasia; and migraine [11]. Clinical diagnosis is generally difficult and must be confirmed by radiologic imaging that commonly shows an enlarged and excessively long styloid process [12]. Only panoramic radiography is effective in making a preliminary diagnosis in patients suspected for Eagle’s syndrome. To confirm the diagnosis, a 3D-CT can be helpful in defining the length, angulation, and anatomic relationship of the styloid process. In addition to these radiographs, a posterior-anterior projection or anterior- posterior projection of skull view, lateral cephalogram, lateral oblique mandible view, Towne’s view, and open-mouth odontoid views are also useful [13].
Eagle’s syndrome can be treated pharmacologically, surgi- cally, or both. Nonsurgical treatments include the admini- stration of NSAIDs, steroids, or carbamazepine, as well as the injection of local anesthetic agents, which has poor results [14]. The surgical management of an elongated styloid process consists of the following two major procedures: a transoral approach and an extraoral cervical approach [11]. The choice of treatment usually depends on the experience of the surgeon.
Nevertheless, surgical resection has generally been accepted as the primary treatment modality for Eagle’s syndrome [14]. In surgical treatment, the external approach provides adequate anatomic exposure of both the styloid process and nearby structures. This exposure will be important in the presence of Fig. 4. In the 3-dimensional computed tomography view at 9 months
after resection of the elongated styloid process.
Seong-Yong Moon et al.
121 vascular injury with intensive bleeding. In addition, this sterile
surgical technique decreases the risk of bacterial contamination.
The major disadvantage of the external approach, however, is postoperative cosmetic deformity due to scar formation.
Other disadvantages are the necessity for general anesthesia and extensive fascial dissection, a longer surgery duration, and uncomfortable paresthesias of the great auricular nerve and cutaneous nerve [11]. Additionally, manual fracturing through transpharyngeal manipulation can be applied, although this usually does not relieve symptoms and may cause possible damage to nearby neurovascular structures [15]. Transoral/
intraoral resection of the styloid process is relatively easy to perform, is less time consuming, and avoids external scars as well as extensive fascial dissection [15]. This technique could also be performed under local anesthesia [15]. However, disad- vantages associated with the transoral approach are the risk of deep cervical infection, poor visualization of the surgical field, and the risk of neurovascular injury while attempting to leave the shortest residue of the styloid process [11,15]. It is generally accepted that the intraoral approach should be used only if the distal tip of the styloid process can be palpated in the tonsillar fossa. More importantly, however, the intraoral approach should be used only if the surgeon is familiar with the technique and how to handle possible detrimental complications [11]. In this case, Piezosurgery was used for resecting the calcified styloid process, Piezosurgery could prevent soft tissue injury and resect precisely.
Eagle’s syndrome can be diagnosed based on clinical symp- toms and radiologic examination with panoramic and 3D-CT radiographs. An elongated styloid process can be successfully resected using Piezosurgery via an intra-oral approach without postoperative complications.
Acknowledgments
This study was supported by research fund from Chosun University, 2013.
References
1. Eagle WW: Elongated styloid processes: report of two cases.
Arch Otolaryngol 25:584-587, 1937.
2. Eagle WW: Symptomatic elongated styloid process; report of two cases of styloid process-carotid artery syndrome with operation. Arch Otolaryngol 49:490-503, 1949.
3. Kaufman SM, Elzay RP, Irish EF: Styloid process variation.
Radiologic and clinical study. Arch Otolaryngol 91:460-463, 1970.
4. Cernea CR, Hojaij FC, De Carlucci D Jr, Plopper C, Vanderley F, Guerreiro CA, Viana MS: First-bite syndrome after resection of the styloid process. Laryngoscope 117:181-182, 2007.
5. Balbuena L Jr, Hayes D, Ramirez SG, Johnson R: Eagle's syndrome (elongated styloid process). South Med J 90:331-334, 1997.
6. Cantín LM, Suazo Galdames I: Eagle syndrome or stylohyoid syndrome? Neurologia 26:254, 2011.
7. Buono U, Mangone GM, Michelotti A, Longo F, Califano L: Surgical approach to the stylohyoid process in Eagle's syndrome. J Oral Maxillofac Surg 63:714-716, 2005.
8. Monsour PA, Young WG: Variability of the styloid process and stylohyoid ligament in panoramic radiographs. Oral Surg Oral Med Oral Pathol 61:522-526, 1986.
9. Steinmann EP: A new light on the pathogenesis of the styloid syndrome. Arch Otolaryngol 91:171-174, 1970.
10. Langlais RP, Miles DA, Van Dis ML: Elongated and mineralized stylohyoid ligament complex: a proposed classification and report of a case of Eagle's syndrome. Oral Surg Oral Med Oral Pathol 61:527-532, 1986.
11. Diamond LH, Cottrell DA, Hunter MJ, Papageorge M: Eagle's syndrome: a report of 4 patients treated using a modified extraoral approach. J Oral Maxillofac Surg 59:1420-1426, 2001.
12. Slavin KV: Eagle syndrome: entrapment of the glossopha- ryngeal nerve? Case report and review of the literature. J Neurosurg 97:216-218, 2002.
13. Goldstein GR, Scopp IW: Radiographic interpretation of calcified stylomandibular and stylohyoid ligaments. J Prosthet Dent 30:330-334, 1973.
14. Sela J, Abu el Naaj I, Peled M. The styloid process elongation syndrome (Eagle syndrome): a case report. Refuat Hapeh Vehashinayim 20:44-45, 80, 2003.
15. Chase DC, Zarmen A, Bigelow WC, McCoy JM: Eagle's syndrome: a comparison of intraoral versus extraoral surgical approaches. Oral Surg Oral Med Oral Pathol 62:625-629, 1986.