Symptomatic Anomalous Coronary Artery Origin Diagnosis and Interventions
4
0
0
전체 글
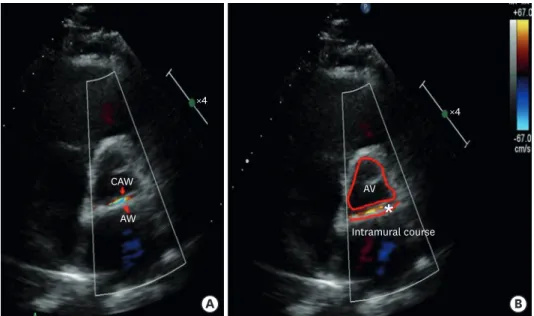
(2) Right ACAOS. *. *. B. A Figure 2. A CT angiographic scan demonstrate an anomalous origin (asterisk) of RCA (A) without a clear demonstration of the intramural course of the vessel (B). CT = computed tomography; RCA = right coronary artery.. clearly visible in the parasternal short axis view (Figure 3). A new coronary angiography with intravascular ultrasound examination of the intramural course demonstrated a phasic compression of the intramural decourse not apparent on the previous coronary angiography (Figure 4). A III generation DES has been successfully implanted (Figure 5) with ST changes and symptomatology resolution (Figure 6). Emotional or environmental stress and hypertensive status may have a potential role in phasic lumen reduction of the proximal vessel. ×4. CAW. ×4. AV. AW. *. Intramural course. A. B. Figure 3. Transthoracic echocardiogram in parasternal short axis view shows an intramural decourse (asterisk) of the of the proximal portion of RCA (A, B: the red conturns highlight the borders of the aortic annulus and the intramural wall of the vessel). AW = atrioventricular valve; AV = aortic valve; CAW = common atrioventricular valve; RCA = right coronary artery.. https://e-kcj.org. https://doi.org/10.4070/kcj.2018.0025. 443.
(3) Right ACAOS. B. A. C. Figure 4. Urgent coronary angiography in right anterior oblique projection (A) and IVUS examination: a compression of the intramural course is apparent being the proximal part of the vessel squeezed into an elliptical shape with clearly reduced luminal area and no real plaque burden (B). The rest of the vessel is free from significant atherosclerosis (C). IVUS = intravascular ultrasound.. Stent strut. B. Stent strut. A. C. Figure 5. IVUS control after successful stenting (A): the first 20 mm of the proximal portion of the vessel, that is the length of the intramural course were covered by the stent with a normal luminal area (B, C). IVUS = intravascular ultrasound.. https://e-kcj.org. https://doi.org/10.4070/kcj.2018.0025. 444.
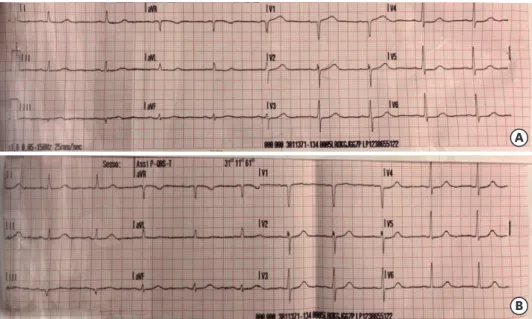
(4) Right ACAOS. A. B Figure 6. Electrocardiogram (A) pre- and (B) post-successful stenting of the intramural course demonstrating resolution of the ST changes in inferior leads, in particular D3.. lumen in case of ACAOS when an intramural de-course is present. A careful use of both noninvasive and ancillary invasive imaging tools are fundamental for the proper management of such rare anatomo-pathological entity.2). REFERENCES 1. Angelini P, Uribe C, Monge J, Tobis JM, Elayda MA, Willerson JT. Origin of the right coronary artery from the opposite sinus of Valsalva in adults: characterization by intravascular ultrasonography at baseline and after stent angioplasty. Catheter Cardiovasc Interv 2015;86:199-208. PUBMED | CROSSREF. 2. Rigatelli G, Cardaioli P. Endovascular therapy for congenital coronary artery anomalies in adults. J Cardiovasc Med (Hagerstown) 2008;9:113-21. PUBMED | CROSSREF. https://e-kcj.org. https://doi.org/10.4070/kcj.2018.0025. 445.
(5)
수치


관련 문서
Coronary anomalies considered hemodynamically significant included a single coro- nary artery, coronary artery origin from the opposite coronary sinus with an interarterial
Abstract : The left main descending artery (LMDA) of left coronary artery (LCA) in rats runs around the left side of conus arteriosus after arising from the aortic sinus and
Cardiac computed tomography revealed anomalous origin of the RCA from the left coronary cusp coursing between the pulmonary artery and the aorta (white arrows). Ao: aorta, RCA:
Anomalous origin of coronary arteries is a rare congenital anom- aly that was first described in 1948 by White and Edward. 2-6) In particular, in- cidence of a left coronary
We reported the surgical correction of the anomalous origin of right coronary artery from left sinus of valsalva between the aorta and pulmonary trunk using the unroofing
Conclusion: Anatomic re- pair of anomalous left coronary artery from the pulmonary artery offered an excellent surgical results, especially in terms of the recovery of left
Background: For the surgical management of anomalous origin of the left coronary artery from the pulmonary ar- tery (ALCAPA), there have been various techniques that reduce the
Objective: To examine the fractional flow reserve derived from computed tomographic angiography (CT-FFR) in patients with anomalous origin of the right coronary artery from the
