627 CASE REPORT
DOI 10.4070 / kcj.2008.38.11.627
Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright ⓒ 2008 The Korean Society of Cardiology
Anomalous Origin of the Right Coronary Artery From the Main Pulmonary Artery Presenting as Angina Pectoris in an Adult
Chung Su Park, MD1, Weon Kim, MD1, Sung Bum Hong, MD1, Sun Ho Hwang, MD1, Wan Kim, MD1 and Byung Hee An, MD2
1The CardioVascular Center of Gwangju Veterans Hospital, Gwangju, 2Cardiac Surgery of Chonnam National University Hospital, Gwangju, Korea
ABSTRACT
The anomalous origin of the right coronary artery from the main pulmonary artery has been rarely reported. We report a 63-year-old male with angina pectoris who was shown to have an anomalous origin of the right cor- onary artery from the main pulmonary artery. The abnormal origin was identified by conventional coronary angiography, but the abnormal course of the artery was precisely delineated by high resolution multi-slice com- puterized tomography. The patient underwent successful surgical correction of the anomalous vessel with com- plete resolution of symptoms. (Korean Circ J 2008;38:627-629)
KEY WORDS: Coronary vessel anomalies; Coronary artery disease.
Introduction
High resolution multi-detector computerized tomo- graphy (MDCT) is a non-invasive diagnostic modality which has been shown to be useful for patients with a suspected anomaly of a coronary artery. Cases involving anomalous origins of coronary arteries from the pulmo- nary artery have rarely been reported.1) We report herein a patient with an anomalous origin of the right coronary artery (RCA) from the main pulmonary artery (MPA) who underwent successful corrective surgery.
Case
The patient was a 63-year-old male with exertional dyspnea and effort-induced angina for 6 months. The pain was relieved with rest. The risk factors for coronary artery disease included hypertension and a 50-pack-year smoking history. He did not show specific abnormalities on physical examination. Biochemical test results, in- cluding cardiac enzymes, were within normal ranges. A chest X-ray showed mild cardiomegaly. An electrocar- diogram showed a normal sinus rhythm. Two-dimen-
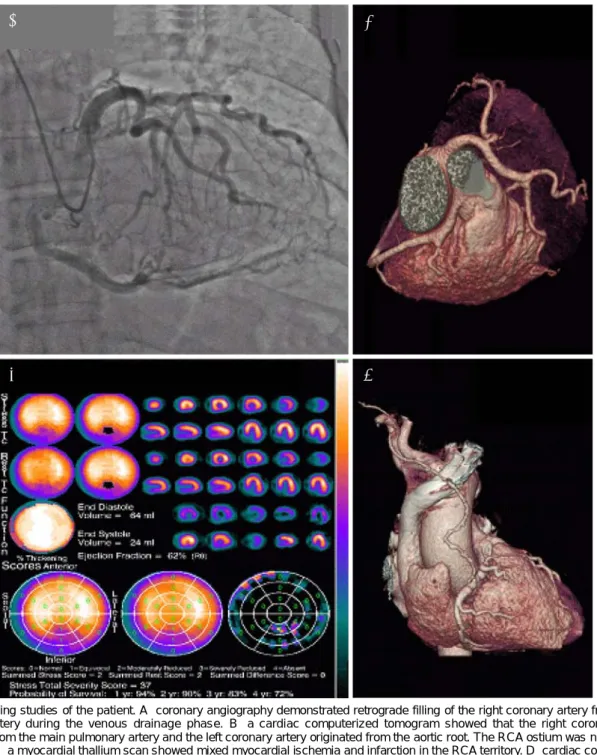
sional echocardiography showed normal left ventricular size and preserved systolic function. A treadmill test showed marked ischemic ST-segment depression in II, III, aVF, and V3-6. Coronary angiography demonstrated retrograde filling of the RCA from the left coronary artery during the venous drainage phase, and did not show significant stenosis in the coronary arteries (Fig.
1A). An aortogram showed flow into the left coronary artery, but did not show a RCA ostium. The MDCT showed that the RCA originated from the MPA and the left coronary artery originated from the aortic root (Fig.
1B). The RCA ostium was not detected by MDCT. We performed a myocardial thallium scan (M-SPECT) to ascertain the relationship between the symptoms and the coronary anomaly. The M-SPECT showed myo- cardial ischemia and infarction in the RCA territory (Fig. 1C). The patient underwent bypass surgery from the right internal mammary artery to the RCA after closure of the RCA originated in the main pulmonary artery. A cardiac computerized tomography obtained postoperatively showed a successful result (Fig. 1D). The patient was discharged and did not complain of any cardiac symptoms for 3 months of follow-up.
Discussion
In a large series of 126,595 coronary angiograms, anomalous right coronary arteries were reported in 0.26%.2) An anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) syndrome
Received: July 19, 2008
Revision Received: August 19, 2008 Accepted: August 21, 2008
Correspondence: Weon Kim, MD,The CardioVascular Center of Gwangju Veterans Hospital, 887-1 Sanwol-dong, Gwangsan-gu, Gwangju 506- 705, Korea
Tel: 82-62-602-6288, Fax: 82-62-602-7174 E-mail: [email protected]
628·Anomalous Origin of RCA From Pulmonary Artery
is a more common anomaly than an anomalous origine from the right coronary artery.3) Most patients with ALCAPA syndrome die from severe congestive heart failure due to chronic mitral regurgitation and global ischemic cardiomyopathy. An anomalous right coronary artery usually originates from the left sinus valsalva, the left main coronary artery, the thoracic aorta, and the pulmonary artery.4) An anomalous origin of the right coronary artery from the pulmonary artery in the adult has been rarely reported1) because most of the patients remain asymptomatic and are found incidentally in
adulthood.5)6) Symptoms of myocardial ischemia seldom develop in patients with this anomaly in the absence of additional atherosclerotic or other disease processes.
These symptoms have included acute myocardial infarc- tion, angina pectoris, syncope, non-fatal ventricular fi- brillation, and sudden death.7) We have demonstrated an anomalous origin of the right coronary artery from the pulmonary artery to be the cause of myocardial is- chemic symptoms through several tests, including MDCT and M-SPECT. Although coronary artery anomalies are usually diagnosed during coronary angiograms, MDCT
Fig. 1. Imaging studies of the patient. A: coronary angiography demonstrated retrograde filling of the right coronary artery from the left coronary artery during the venous drainage phase. B: a cardiac computerized tomogram showed that the right coronary artery originated from the main pulmonary artery and the left coronary artery originated from the aortic root. The RCA ostium was not detected by MDCT. C: a myocardial thallium scan showed mixed myocardial ischemia and infarction in the RCA territory. D: cardiac computerized tomogram checked after the operation showed a patent bypass graft vessel and closure of the RCA originated in the main pulmonary artery. RCA: right coronary artery, MDCT: multi-detector computed tomography.
A B
C D
Chung Su Park, et al.·629
may be beneficial in many clinical situations. MDCT coronary angiography currently appears to fulfill the re- quirements of a non-invasive morphologic assessment of the coronary arteries, as a result of its combination of rapid acquisition speed, spatial resolution, and robust- ness of use.3) It is an effective and non-invasive method to identify coronary artery anomalies in clinical practice when the patient has chest pain. Operative correction is the proper treatment for the anomalous coronary artery arising from the pulmonary artery.1) In our case, surgical correction was achieved by bypass surgery from the right internal mammary artery to RCA.
REFERENCES
1) Fernandez ED, Kadivar H, Hallman GJ, Reul GJ, Ott DA, Cooley DA. Congenital malformations of the coronary arteries. Ann Thorac Surg 1992;54:732-40.
2) Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595
paints undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990;21:28-40.
3) Rha SW, Park CG, Yong HS, et al. Anomalous origin of the left coronary artery from the pulmonary artery in an elderly patient visualized by three-dimensional multidetector computed tomo- graphy coronary angiography. Korean Circ J 2005;35:84-7.
4) Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary con- genital anomalies of the coronary arteries: a coronary arterio- graphic study. Int J Cardiol 2000;74:39-46.
5) Wald S, Stonecipher K, Baldwin BJ, Nutter DO. Anomalous origin of the right coronary from the pulmonary artery. Am J Cardiol 1971;27:677-81.
6) Tingelstad JB, Lower RR, Eldredge WJ. Anomalous origin of the right coronary artery from the main pulmory artery. Am J Cardiol 1972;30:670-3.
7) Mintz GS, Iskandrian AS, Bemis CE, Mundth ED, Owens JS.
Myocardial ischemia in anomalous origin of the right coronary artery from the pulmonary trunk: proof of a coronary steal. Am J Cardiol 1983;51:610-2.