심방
6
0
0
전체 글
(2) 히, 우심증 환자에서 병발한 상심실성 빈맥을 전극도자 2)4)6-8). 절제술로 치료한 경우는 전세계적으로도 드물고, 국내에서는 아직 보고된 바가 없다.. 인 심계항진을 주소로 내원하였다. 10년전 신체검진시 우 심증을 진단받았으나 추가적인 검사는 받지 않았다. 가족력:특이 사항 없었다.. 이에 저자 등은 심계항진을 주소로 내원한 심방 중격. 신체 진찰소견:내원 당시 의식은 명료하였으며, 혈압. 결손이 동반된 내장 정상위 우심증(단독 우심증, isol-. 은 160/100 mmHg, 맥박은 분당 170회, 호흡수는 분. ated dextrocardia) 환자에서 심전도와 전기생리 검사. 당 20회, 체온은 36.5℃였고, 노작성 호흡곤란이나 전신. 로 방실결절 회귀성 빈맥을 진단하고, 전극도자절제술. 부종 등은 호소하지 않았으며, 청색증이나 곤봉상 수지. 을 성공적으로 시술하여 치료한 예를 경험하였기에 문헌. 는 관찰되지 않았다. 심장 청진상 우측 흉골연에서 4도. 고찰과 함께 보고하는 바이다.. 의 수축기 잡음이 청진되었다. 양측 폐야에서 이상 호흡 음은 청진되지 않았으며, 복부촉진상 간・비장종대는 없. 증. 례. 었다. 심전도 소견:내원 당시 빈맥이 지속되는 동안에 사. 환 자:한○규, 남자, 34세.. 지유도와 흉부유도를 정위치에 위치시키고 찍은 12유도. 주 소:3일간의 간헐적인 발작적 심계항진.. 심전도에서 분당 약 170회의 넓은 QRS파형의 빈맥이. 현병력:환자는 15세경 약 30분간의 심계항진을 처. 관찰되었으며, 전체 유도에서 뚜렷한 P파는 관찰되지 않. 음 경험하였고 최근 1년전부터는 심계항진의 빈도가 잦. 았다(Fig. 1). 심전도 모니터로 관찰하면서 Adenosine. 아지고 지속시간이 길어졌으며, 내원 당일에는 약 2시간. 6 mg을 정주하였고 약 10초 후 빈맥은 소실되었다. 동. 가량 흉부 불쾌감과 경도의 어지러움을 동반한 지속적. 율동으로 전환된 후에 찍은 12유도 심전도소견은 분당. Fig. 1. Electrocardiogram on admission showed wide QRS tachycardia (170BPM). No P wave was identifiable in any lead.. Fig. 2. 12-lead electrocardiogram during sinus rhythm showed right axis deviation, low voltage QRS in leads I, aVL, V5, V6 and wide QRS complex. The QRS deflections in precordial leads were negative throughout. The amplitude of QRS complex was progressively decreased from V1 to V6.. 1210. Korean Circulation J 2001; 31(11):1209-1214.
(3) Fig. 4. Transthoracic echocardiogram (TTE) showed that markedly enlarged RA, RV and secundum type atrial septal defect (size measured as 1.07 cm;double arrow) with left to right shunt flow by color doppler. LA:left atrium, LV:left ventricle, RA:right atrium, RV:right ventricle.. 를 통해 6F 4극도자 2개와 6F 3극도자 1개를 방사선 투시하에 우심방 상부(high right atrium, HRA), 우심 실 첨부(right ventricular apex, RVA) 및 His poteFig. 3. Chest X-ray showed cardiac apex in right side and gastric air shadow in left side.. ntial 기록 부위(His bundle, HIS)에 각각 위치시켰으. 72회의 넓은 QRS파형의 동율동으로 우측편위 및 I, aVL,. 근위부에 위치시키고자 하였으나 접근이 어려워 우전사. V5, V6유도에서 low voltage QRS를 보였으며, 전 흉부. 미향경사 방향(RAO caudal view)과 좌전사 두향경사. 유도에서 QRS방향은 모두 음성이었고 QRS amplitude. 방향(LAO cranial view)의 방사선 투시하에 좌관동맥. 는 V1에서 V6으로 갈수록 감소되었다(Fig. 2).. 조영술을 시행한 후 조영제가 관정맥동으로 배액되는 것. 흉부 X-선 소견:심첨부는 우측, 위장은 좌측에서 관찰되었다(Fig. 3). 경흉부 심초음파 소견:심첨부는 우측 흉부에서 관 찰되었고, 형태학적 좌심실이 형태학적 우심실의 좌측에. 며, 좌측 쇄골하정맥을 통해 6F 10극도자를 관정맥동. 을 관찰하여 관정맥동 입구의 위치를 정확히 파악한 뒤 우측 대퇴정맥을 통하여 halo 전극도자(10-bipole, DAIG, DUO-DEC)를 성공적으로 관정맥동내에 위치시킬 수 있었다(Fig. 5).. 위치하고 있었다. 우심방, 우심실 확장 소견이 관찰되었. 동맥 혈압을 지속적으로 감시하기 위해서 대퇴동맥에. 고, 좌심실 구출율은 45%로 측정되었다. 중증의 삼첨판. 도관을 삽입하였고, 체표 심전도와 심장내 전기도는 EP-. 역류 소견을 보였으며, 양측 심방간에 약 1.07 cm 크. Lab computer(CardioLabTM, Prucka Engineering Inc.,. 기의 이차공 심방 중격결손과 이를 통한 좌 → 우 단락. USA)에 기록하였다.. 이 관찰되었다(Fig. 4). 삼첨판 도플러를 이용하여 측 정한 추정 우심실 수축기압은 40 mmHg였다. 심도자술:대정맥과 우심방 사이에 19%의 산소포화 도 증가를 관찰할수 있었으며, Qp/Qs는 3.9였다.. 심장의 조율 및 자극은 EP-3 Clinical Stimulator (EPMedical, Inc., USA)를 이용하였다. 자극전기는 2 m/sec, 자극강도는 이완기 역치의 2배로 하였고, filter setting은 30~500 Hz로 하였다. 동율동 상태에서 주. 전기생리검사 및 전극도자절제술:전기생리검사는 검. 기간격은 684 ms, AH간격은 104 ms, HV간격은 14. 사전 6시간 이상 금식한 상태에서 환자와 보호자로부터. ms, QRS duration은 133 ms이었으며(Fig. 6), 심방. 서면동의를 구한 후 시행하였다.. 자극시 방실차단주기(atrioventricular block cycle le-. 먼저 14F 도관을 Seldinger법을 이용하여 2% lid-. ngth, AVBCL)은 350 ms이었다. S1을 600 ms로 조. ocaine으로 국소마취하에 좌측 대퇴정맥에 삽입하고 이. 율하고 8번째 S1후 S2를 가하는 심방조기자극 방법 1211.
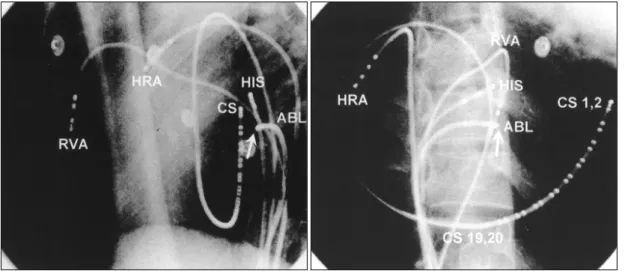
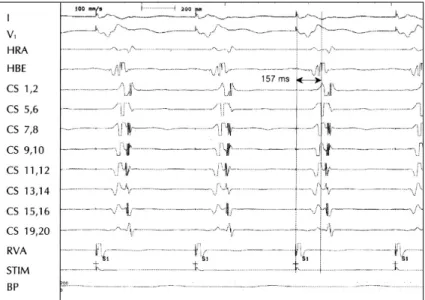
(4) Fig. 5. Successful catheter ablation site of slow pathway (arrow). The left pannel was in LAO view and the right pannel was RAO view. The ablation catheter (ABL) was positioned at right atrial septum near the His potential recording site (HIS). HRA:high right atrium, HIS:the catheter recording maximal His potential, RVA:right ventricular apex, CS: coronary sinus.. Fig. 6. Surface electrocardiogram (I, V1) and intracardiac recordings during sinus rhythm. HRA:high right atrium, HBE:his bunble electrogram, CS:coronary sinus, RVA:right ventricular apex.. (S1-S2 protocol)을 시행했을 때 600/310 ms에서 AH. 였다. 빈맥은 신속심방조율(over drive pacing)에 의해. 간격은 176 ms이다가 600/300 ms일 때는 AH간격이. 쉽게 종료되었다. 이어 계속되는 심방조기자극에서 방실. 426 ms로 갑자기 늘어나는 AH jump 소견을 보이면서. 결절의 이중회로를 통한 상심실성 빈맥이 저속 통로의 유. 저속 통로(slow pathway)를 전향적 전도로 하고 고속. 효불응기(effective refractory period, ERP) 600/230. 통로(fast pathway)를 후향적 전도로 하는 전형적인 방. ms에 이르기 전까지 계속 유발되었다. 심방유효불응기. 실결절 회귀성 빈맥이 유도되었다(Fig. 7). 빈맥의 주기. (AERP)는 600/210 ms였다. 우심실 조율시 역행전도. 간격은 310 ms였고 이때 혈압은 110/70 mmHg로 비. 의 VA간격은 HIS에서 157 ms로 가장 빨랐고(Fig. 8),. 교적 안정적이었으며, 환자는 심계항진을 심하게 호소하. 실방차단주기(VABCL)는 380 ms, 심실유효불응기(VE-. 1212. Korean Circulation J 2001; 31(11):1209-1214.
(5) RP)는 600/230 ms이었다.. 맥이 나타나는 부위에서(Fig. 5) 40초간 에너지를 가하. 방실결절 회귀성 빈맥 진단하에 저속 통로에 대해 전. 고 같은 부위에서 Booster로 2차례에 걸쳐 33 W의 에. 극도자절제술을 시행하기로 하였으며, 좌전사 30도, 우. 너지를 30초씩 가하였으며, 방실차단의 발생여부를 주. 전사 30도의 방향으로 방사선 투시하에 7F 전극절제. 의 깊게 관찰하였다. 이후 심방자극으로 상심실성 빈맥. 도자를 His 기록부위와 관정맥동 입구사이에 위치시켰. 은 유발되지 않았으며, AH jump 소견도 보이지 않았. 다. 관정맥동 입구 근처에서부터 HIS부위로 이동하면서. 다. Isoproterenol 정주 후에도 같은 결과였다.. 28 W의 고주파 에너지를 가하는 도중 방실접합부 빈. 시술 다음날까지 심혈관계 합병증과 상심실성 빈맥의. Fig. 7. Surface electrocardiogram (I, V1) and intracardiac recordings during AVNRT induced by single extra-atrial stimuli. Typical AVNRT (slow-fast) was initiated in association with jump of AH conduction time. HRA:high right atrium, HBE:his bunble electrogram, CS:coronary sinus, RVA:right ventricular apex.. Fig. 8. Intracardiac electrogram during ventricular pacing. The earliest VA conduction was seen at His potential recording area. HRA:high right atrium, HBE:his bunble electrogram, CS:coronary sinus, RVA:right ventricular apex.. 1213.
(6) 재발은 없었으며, 심방 중격결손에 대해서는 향후 수술. 로에 접근하기가 어려워 전극절제도자를 최대한 관정맥. 적 치료를 고려하기로 하고 퇴원하였다.. 동 입구에서 가까운 부위부터 HIS로 차츰 옮겨가면서 고주파 에너지를 가하였으며, 도중에 방실차단의 발생여. 고. 찰. 부를 주의 깊게 관찰하였다.. 우심증은 내장역위를 동반한 우심증(situs inversus with dextrocardia), 내장 정상위에서 심장만 우측에 위. 중심 단어:단독 우심증・방실결절 회귀성 빈맥・전극 도자절제술.. 치한 단독 우심증(situs solitus with dextrocardia, is-. REFERENCES. olated dextrocardia) 그리고 무비증(asplenia synd-. 1) Hebe J, Antz M, Siebels J, Volkmer M, Ouyang F, Kuck. rome)이 동반된 우심증 등 세 가지로 보통 분류된다.9) 이중 단독 우심증에는 흔히 다른 선천성 심장, 혈관 기형 이 동반되는 것으로 알려져 있으며, 심방 및 심실 중격. 2). 10). 결손, 대혈관기형 등이 이에 해당된다.. 이러한 선천성 심장기형 환자에서 상심실성 빈맥등 부 정맥이 병발할 수 있으며 이에 대해 전극도자절제술을. 3). 성공적으로 시술하여 치료한 보고가 최근 잇따르고 있 는데,1-8) Levine 등2)은 엡슈타인 기형, 우심증, 활로 사 징등의 선천성 심장기형 환자에서 발생한 Wolf-Par-. 4). kinson-White(WPW)증후군과 방실회귀성 빈맥을 전 극도자절제술로 치료하여 80%의 성공률을 보고한 바 있고, Abe 등7)은 우심증에 동반된 WPW증후군 1례를,. 5). 4). Wu 등 은 우심증 환자에서 발생한 심방내 회귀성 빈맥 을 전극도자절제술을 이용하여 각각 효과적으로 치료하 여 보고하였다. 심장기형이 있으면 심장의 해부학적 구조와 전도체계. 6). 의 변형으로 인해 전극도자를 심장내에 위치시키거나 목 표 병변(target lesion)을 지도화(mapping)할 때 어려 움이 따르고 전극도자절제술시 예기치 못한 합병증도 발. 7). 생할 수 있다. 본 예에서도 우심증으로 인해 좌우 방실 간 해부학적인 연관관계를 알기가 어려웠으며, 대퇴정맥 과 동맥을 통해 도자를 좌, 우심실에 위치시키고 각각 조. 8). 영술을 시행한 후에야 대략적인 구조를 파악할 수 있었 다. 또한, 전극도자를 위치시킬 때 특히, 관정맥동 입구 를 찾을 때 많은 어려움이 있었으며, 좌관동맥 조영술 후 관정맥동으로 조영제가 배액되는 것을 관찰한 후에 이 를 따라서 관정맥동내에 전극도자를 위치시킬 수 있었다. 전극도자절제술시에도 HIS와 관정맥동 입구 사이의 해 부학적 변형이 매우 심하여 통상적인 방법으로는 저속 통. 1214. 9) 10). KH. High frequency current ablation of supraventricular tachyarrhythmias in congenital heart disease. Herz 1998; 23:231-50. Levine JC, Walsh EP, Saul JP. Radiofrequency ablation of accessory pathways associated with congenital heart disease including heterotaxy syndrome. Am J Cardiol 1993;72:689-93. van Hare GF, Lesh MD, Stanger P. Radiofrequency catheter ablation of paroxysmal supraventricular arrhythmias in patients with congenital heart disease: results and technical considerations. J Am Coll Cardiol 1993;22:883-90. Wu TJ, Chen SA, Chiang CE, Yang CJ, Cheng CC, Wang SP, Chiang BN, Chang MS. Radiofrequency catheter ablation of sustained intraatrial reentrant tachycardia in a patient with mirror-image dextrocardia. J Cardiovasc Electrophysiol 1994;5:790-4. Chiou CW, Chen SA, Chiang CE, Wu TJ, Tai CT, Lee SH, Cheng CC, Ueng KC, Chen CY, Wang SP. Radiofrequency catheter ablation of paroxysmal supraventricular tachycardia in patients with congenital heart disease. Int J Cardiol 1995;50:143-51. Hatala R, Weiss C, Koschyk DH, Siebels J, Cappato R, Kuck KH. Radiofrequency catheter ablation of left atrial tachycardia originating within the pulmonary vein in a patient with dextrocardia. Pacing Clin Electrophysiol 1996; 19:999-1002. Abe H, Araki M, Nagatomo T, Miura Y, Nakashima Y. Radiofrequency catheter ablation of an accessory pathway in dextrocardia. Pacing Clin Electrophysiol 1997; 20:2284-5. Singh B, Talwar KK, Kaul U, Kothari SS, Saxena A, Wasir HS. Radiofrequency catheter ablation of accessory pathways in association with congenital heart disease. Indian Heart J 1997;49:198-200. van PR, Van PS, Vlad P. Anatomic types of congenital dextrocardia: diagnostic and embryologic implications. Am J cardiol 1964;13:510-31. Richard VP, Paul MW, Stella VP. Malpositions of the heart. In: arthur JM, Forrest HA, George CE, editors. Heart disease in infants, children and adolescents. 2nd ed. Baltimore: waverly press, Inc.; 1977. p.438-43.. Korean Circulation J 2001; 31(11):1209-1214.
(7)
수치


관련 문서
The arrow indicates bulging enhancing mass in right orbit apex, extending to cavernous sinus with fatty marrow signal loss and enhancement of right lesser
Electrocardiogram revealed normal sinus rhythm without any ischemic signs but chest radiograph showed pleural effusion at right lobe and pneumopericardium at left heart
척 -스트라우스증후군은 전신적인 질환이기 때문에, 심장 침범 으로 인한 심부전이 발생한 척-스트라우스증후군 환자에서 심장 Fig. Initial electrocardiogram shows
Electrical activation time for normal sinus rhythm and artificial pacing in apex, left ventricular free wall, and right ventricular free wall were obtained
After a right atrium angiography, we crossed PFO with coronary sinus catheter to assess the reference en- try point, and then another 7 Fr catheter was inserted to the left fe-
draining into the left atrium without arterial oxygen unsatu- ration. Persistierende linke ober hohlvene und mitralstenose. Sinus node dysfunction associated with absence of
In the second case, the right atrial ostium of the coronary sinus was again atresi and an abnormal tubular communication between the coronary sinus and the left atrium coexisted
We describe here a case of migration of the tip of a port catheter from the right atrium to the right axillary vein in a patient with severe cough.. Coughing was suggested for this
