Continuous High-Pressure Negative Suction
Drain: New Powerful Tool for Closed Wound
Management: Clinical Experience
by
Seung Jun Shin
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
Continuous High-Pressure Negative Suction
Drain: New Powerful Tool for Closed Wound
Management: Clinical Experience
by
Seung Jun Shin
A Dissertation Submitted to The Graduate School of
Ajou University in Partial Fulfillment of the Requirements for
The Degree of Ph.D. in Medicine
Supervised by
Myong Chul Park, M.D., Ph.D.
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
This certifies that the dissertation
of Seung Jun Shin is approved.
SUPERVISORY COMMITTEE
The Graduate School, Ajou University
December, 19th, 2014
i
ABSTRACT
-Cont
i
nuousHi
gh-Pr
essur
eNegat
i
veSuct
i
on Dr
ai
n:
New Power
f
ulToolf
orCl
osedWoundManagement
:
Cl
i
ni
calExper
i
ence
Background & Aims:Although various reconstructive flap surgeries have beensuccessfullyperformed,therestillaredifficultwoundcomplications,such
as seroma formation,wound margin necrosis,delayed wound healing,and
even flap failures.The negative-pressure wound therapy hasbeen described in detailin the literature to assistopen chronic/complex wound closure in reconstructive surgery.However,the negative-pressure wound therapy was difficulttobeappliedundertheincisionalclosedwounds.
Methods:A totalof23 patients underwentthe various reconstructive flap surgeries with continuous high-pressure negative suction drain.Instead of
using regular suction units,BarovacⓇ (50 - 90 mmHg,Sewoon Medical,
Seoul,RepublicofKorea)drainagetubeswereconnectedtothe wallsuction
unit, providing continuous high-powered negative pressure. In addition,
continuoussubatmosphericsuction pressure(100-300 mmHg)wasapplied.
Outcome of the measures was obtained from the incidence of seroma,
volume of postoperative drainage,hospitalization period,and incidence of
other typical wound complications. Dead space was evaluated
postoperativelywithultrasonography.
Results:Using continuous high-pressure negative suction drain, successful
managementofseroma was obtained withoutany major complication such
aswoundinfection,flaploss,andwoundmargin necrosis,exceptforonly 1
drain in the latissimus dorsi donor site was significantly reduced in
comparison with the authors’previous data (P = 0.047).The volume of
drainage and hospitalization period were also reduced;however,these were notstatistically significant. The dead space with continuous high-pressure negative suction drain was more reduced than in the controlgroup in the immediatepostoperativeperiodandconfirmedwithultrasonography.
Conclusions:Continuous high-pressure negative suction drain mightbe the
simple and powerful solution in the management of challenging closed
wounds.
Key Words:Seroma,Wallsuction,Continuoushigh-pressurenegativesuction
iii
TABLE OF CONTENTS
ABSTRACT ···ⅰ TABLE OF CONTENTS ···ⅲ LIST OF FIGURES ···ⅳ LIST OF TABLES ···vⅠ.INTRODUCTION···1
Ⅱ.PATIENTS AND METHODS···3
Ⅲ.RESULTS ···8
IV.CASE REVIEWS ···12
V.DISCUSSION ···15
REFERENCES ···20
LI
ST OF FI
GURES
Fig.1.Barovac® (Sewoonmedical,Seoul,Korea)draintubesareperforated
polyvinylchloridesuctiondrainsproviding50-90mm Hgofnegative
pressure···5
Fig.2.Wallsuctionunitprovideshighpressurenegativepowerranging
from 0-300mmHg···6
Fig.3.Volumeofdrainoutputuntildrainsincontrolandwallsuction
groupswereremoved ···10
Fig.4.Ultrasonographywasexaminedimmediatepostoperatively.Compared withregularsuctionunit(leftpanel),bothdeadspaceandthegap betweenlayersweredefinitelyreduced(rightpanel).Redarrows indicatedeadspace,andbluearrowsindicatedrainagetube ···11
Fig.5.Onapplyinghighpressurenegativesuctiontherapyundertheskin
flapat150–160mmHg,theflapsweremorestabilizedtofixthe
underlyingtissues(bluearrows)thanothermethodssuchas
v
LI
ST OF TABLES
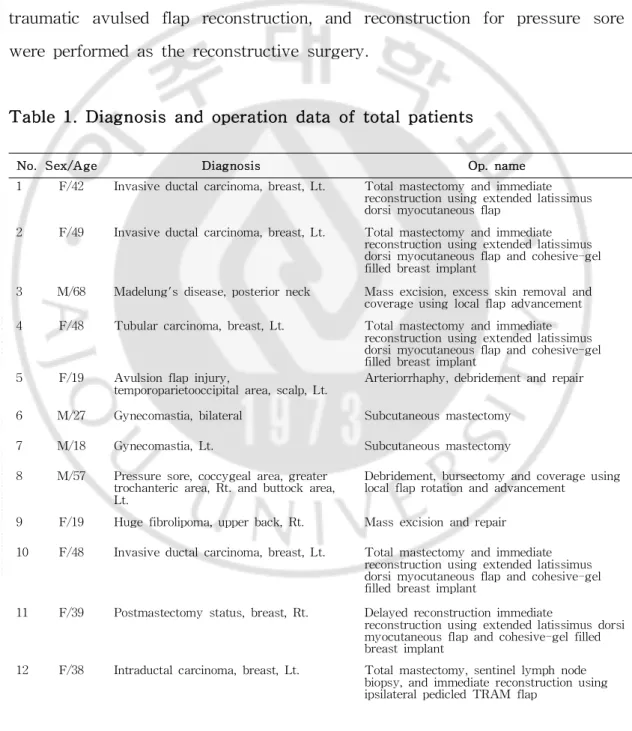
Table1.Diagnosisandoperationdataoftotalpatients···3
Table2.Comparisonofoutcomemeasurementsinextendedlatissimus
I
.I
NTRODUCTI
ON
Nowadays, various reconstructive flap surgeries have been
successfully performed to cover the challenging wounds thatrequire extra care.There are some complications - donor site seroma in the latissimus
dorsiflap,seroma in the abdominoplasty area,hematoma under the flaps,
wound margin necrosis,partialflap loss,repetitive seroma,and even flap necrosis.Among severaldifferenttechniques,whichhavebeendocumentedin the managementofthese complications,some preventive maneuvers are not uniformlysuccessful.
Negative-pressure wound therapy (NPWT) is an adjunct therapy
using negativepressureto removefluid from open woundsthrough asealed
dressing(reticulatedopen-cellpolyurethaneetherfoam)andaspecializedtube thatis connected to a suction unit.The technique is designed to remove chronicedema fluid,thereby decreasing theafterload to blood flow,resulting in increased localized tissue perfusion (Timmeretal.,2005;Scherer etal., 2008;Schintler,2012;Argenta etal.,2006).With applied negative-pressure forces,theformation ofgranulation tissueisenhanced (Timmeretal.,2005; Schintler,2012;Leeetal.,2011;Saxenaetal.,2004). Thenegative-pressure technique has been demonstrated to be an extremely efficacious method to stimulatehealingbysecondaryintention(Argentaetal.,2006;.Leeetal.,2011; Mendonca etal.,2006).Thiseffectivetechniquehas been mostly applied on
challengingwoundssuchasexposedcomplex andchronicwounds,oronskin
graftarea,orclosed surgicalincision sites(Leeetal.,2011;Mendoncaetal.,
2006;Kilpadiand Cunningham,2011;Schmedes etal,2012;Ubbink etal,
2008;ArgentaandMorykwas,1997).
2
-wounds oroverthe closed surgicalincision sites.This reportreviews such articles that state that using negative-pressure technique successfully preventedthecomplicationsinvariousflapsurgeries.
No.Sex/Age Diagnosis Op.name 1 F/42 Invasiveductalcarcinoma,breast,Lt. Totalmastectomyandimmediate
reconstructionusingextendedlatissimus dorsimyocutaneousflap
2 F/49 Invasiveductalcarcinoma,breast,Lt. Totalmastectomyandimmediate reconstructionusingextendedlatissimus dorsimyocutaneousflapandcohesive-gel filledbreastimplant
3 M/68 Madelung'sdisease,posteriorneck Massexcision,excessskinremovaland coverageusinglocalflapadvancement 4 F/48 Tubularcarcinoma,breast,Lt. Totalmastectomyandimmediate
reconstructionusingextendedlatissimus dorsimyocutaneousflapandcohesive-gel filledbreastimplant
5 F/19 Avulsionflapinjury,
temporoparietooccipitalarea,scalp,Lt.
Arteriorrhaphy,debridementandrepair 6 M/27 Gynecomastia,bilateral Subcutaneousmastectomy
7 M/18 Gynecomastia,Lt. Subcutaneousmastectomy 8 M/57 Pressuresore,coccygealarea,greater
trochantericarea,Rt.andbuttockarea, Lt.
Debridement,bursectomyandcoverageusing localflaprotationandadvancement
9 F/19 Hugefibrolipoma,upperback,Rt. Massexcisionandrepair 10 F/48 Invasiveductalcarcinoma,breast,Lt. Totalmastectomyandimmediate
reconstructionusingextendedlatissimus dorsimyocutaneousflapandcohesive-gel filledbreastimplant
11 F/39 Postmastectomystatus,breast,Rt. Delayedreconstructionimmediate
reconstructionusingextendedlatissimusdorsi myocutaneousflapandcohesive-gelfilled breastimplant
12 F/38 Intraductalcarcinoma,breast,Lt. Totalmastectomy,sentinellymphnode biopsy,andimmediatereconstructionusing ipsilateralpedicledTRAM flap
I
I
.PATI
ENTS AND METHODS
Thisstudyincluded23patientswhounderwentthereconstructive
surgery from September 2011 to January 2013 (Table 1). Breast
reconstruction,abdominoplasty,giantmass excision,gynecomastia correction, traumatic avulsed flap reconstruction,and reconstruction for pressure sore wereperformedasthereconstructivesurgery.
4
-13 F/54 Pendulousabdomen Fullabdominoplastyandliposuction 14 F/51 Recurredductalcarcinomainsitu,
breast,Lt. rSkieconstnsparructingmasionusingetectomyandixtendedlatmmeissidimusate dorsimyocutaneousflapandcohesive-gel filledbreastimplant
15 F/51 Infiltratingductalcarcinoma,breast,
Rt. iNimmepplesdiatpareriengtconsottralmasuctionustectiomyandngextended latissimusdorsimyocutaneousflapand cohesive-gelfilledbreastimplant 16 F/44 Pendulousabdomen Fullabdominoplasty
17 F/44 Recurredseroma,back
S/P Nipplesparingmastectomyand immediatereconstructionwithextended latissimusdorsiflaptranspositionwith cohesivegelbreastimplant
d/tDuctalcarcinomainsitu,breast,Lt.
Drain tube insertion and connect with wall suction
18 F/57 Giantlipoma,anteriorneck Massexcision,excessskinremovaland coverageusinglocalflapadvancement 19 F/46 Ductalcarcinomainsitu,breast,Lt. Nipplesparingmastectomyandimmediate
reconstructionusingextendedlatissimusdorsi flaptranspositionwithcohesivegelbreast implant
20 F/44 Avulsionflapinjury,lowerlegand
dorsum offoot,Lt. Defatting,debridementandrepair 21 F/37 Pressuresore,greatertrochanteric
area,Lt. Delocbralfidelaprmentot,burationandadvancsectomyandcemeoventrageusing 23 M/54 Recurredpressuresore,coccygealarea Debridement,bursectomyandcoverage
usinggluteusmaximusmusculocutaneousflap rotation
F,female;M,male;S/P,statuspost;d/t,dueto.
When the operative fields were closed after the main operative procedures,BarovacⓇ (SewoonMedical,Seoul,RepublicofKorea)draintubes, which areperforated polyvinylchloridesuction drains(Fig.1),wereinserted into the cavity.In place ofthe regularsuction unitproviding 50 to 90 of
mmHg negative pressure, the drains were connected to the continuous
high-pressure suction wallsuction unit(Fig.2).Negative pressure ranged
from 120 to 300 mmHg,minimalpressure,to maintain the stable flap base
and to reduce dead space.In the largeroperative area,the higherpressure
quilting sutures orfibrin glue injection.To evaluate the dead space in the operative sites,ultrasonography was performed.Patients were treated with the standard conventionalpostoperative care (Stebbins etal.,2011).Amount
of the volumes and duration of wound drainage were recorded
postoperatively.When drainage was less than 20 mL fora 24-hourperiod,
thedrainagetubeswereremoved(Chaetal.,2012;Shinetal.,2012).
Fig. 1. Barovac® (Sewoon medical, Seoul, Korea) drain tubes are
perforated polyvinylchloridesuction drainsproviding 50- 90mmHg of
6
-Fig. 2. Wall suction unit provides high pressure negative power
Outcome ofthe measures was the volume ofdrainage output,the length oftimethatthedrain remained in thesite,hospitalization period,and evaluationofdeadspaceusingultrasonography.Inaddition,anycomplications, including recurred seroma,wound dehiscence,infections,and delayed wound healing, were studied. In the group of the breast reconstruction with latissimus dorsiflap,each patientwas compared with thepatients who had undergone the same surgical procedures without high-pressure negative suctiondrain.
Statisticalanalysis was performed using the StatisticalPackage for theSocialSciencesversion13.0(Windowsversion,StatisticalPackageforthe
SocialSciences Inc,Chicago,IL).The Mann-Whitney test was used to
8
-I
I
I
.RESULTS
Continuous high-pressure negative suction drain was applied to 23 patientswhounderwentreconstructiveflapsurgery.Among them,therewere 8 breast reconstructions with extended latissimus dorsiflap and cohesive gel-filled implant,1 breast reconstruction with pedicled transverse rectus
abdominus myocutaneous flap, 2 abdominoplasties, 3 giant benign mass
removals,2 traumatic avulsed flap reconstructions,and 8 other cases.The authors used the continuous high-pressure negative suction drain as an
adjuvantmethod.There was no typicalwound complication,such as wound
infection,flaploss,andwoundmargin necrosis,exceptfor1recurredseroma case,which waseasily solved with theone-timeaspiration and compressive
dressing.However,inthecontrolgroup,8in 10caseshadseromaformation,
and serialaspiration with compression dressing was performed to treatthe seroma.In extended latissimus dorsiflap donor site,drainage volume was significantly reduced in comparison with recentdataof10patientsfrom the authors’previous study.These patients underwenta conventionaldonorsite closurewithoutquiltingsuturesorfibringlueinjection.
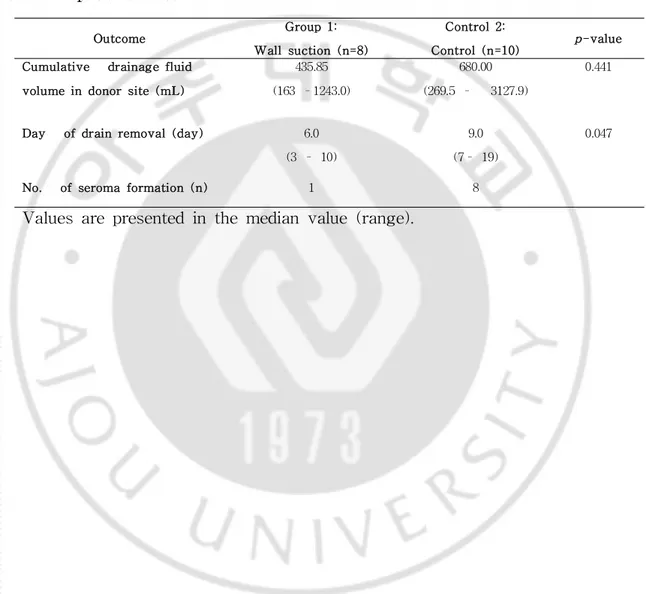
Thetotaldrainagevolumesweredecreasedwiththismethod,from
a median of680.00 (269.5 - 3127.9)mL to 438.85 (163.0 - 1243.0)mL in
extendedlatissimusdorsiflapdonorsite.Themedianindwelling periodofthe
drainswas6.0 (3 - 10)dayswith thewallsuction group and 9.0 (8 - 19)
dayswith thecontrolgroup(Table2andFig.3).Themedian hospitalization
periodofthewallsuctiongroup(8days)wasshorterthanthatofthecontrol
group (12 days);however,this was notstatistically different(P = 0.183). Ultrasonography was examined immediately after the operation.Compared with the regular suction unit,dead space was definitely reduced (Fig.4).
Outcome Group1: W allsuction (n=8)
Control2:
Control(n=10) p-value Cumulative drainagefluid
volumein donorsite(mL)
435.85 (163–1243.0)
680.00 (269.5– 3127.9)
0.441
Day ofdrain removal(day) 6.0 (3– 10)
9.0 (7– 19)
0.047
No. ofseromaformation (n) 1 8
Valuesarepresentedinthemedianvalue(range).
Finally,woundslastedfor6monthsto18months.
Table 2.Comparison ofoutcome measurements in extended latissimus
10
-Fig.3.Volumeofdrain outputuntildrains in controland wallsuction
Fig. 4. Ultrasonography was examined immediate postoperatively.
Comparedwith regularsuctionunit(leftpanel),bothdeadspaceandthegap
between layers were definitely reduced (right panel).Red arrows indicate
12
-I
V.CASE REVI
EWS
Patient1
A 43-year-oldwomanwasexaminedintheclinicforreconstruction
of her right breast.She had undergone modified radical mastectomy for
intraductal carcinoma 5 years ago. Breast reconstruction using extended latissimus dorsifasciocutaneous flap and cohesive gel-type breast implant
(Mentor,Santa Barbara,CA;175mL)was performed.When the donor site
was closed,simple suture method withoutquilting suture was applied,and
thedrainagetubewasplaced into thedonorsitewith theconnection tothe
high-pressurenegativesuction unitat300mmHg.Thedrainagevolumewas
134mL onthefirstpostoperativeday anddecreasedrapidly sincethesecond
postoperativeday.Onthefifthpostoperativeday,thedrainagewas22mL
duringa24-hourperiod,sothedrainwasremovedonthesixthpostoperative
day.Therewerenowound-relatedproblemsandnoseromaformation.
Patient2
A 19-year-oldwoman had atrafficaccidentand washospitalized for
multiple rib fractures,livercontusion,and leftparietotemporalfasciocutaneous avulsion flap injury. The superficial temporal artery was transected. In emergentoperation,arteriorrhaphy wasdonesuccessfully.Afterdirty margin debridement,theavulsedflapwasrepairedwithsimplesilasticdrains.Despite a successfuloperation,a largeamountofserous drain was noted along the silasticdrains.
On thefourth postoperativeday,thedrainagetubewasplaced under
suction unit at 120 mmHg.On the fifth postoperative day,the drainage
volumewas25mL.Drainagevolumewasdecreaseddaily andwas5mL on
the ninth postoperative day, so the drain was removed on the 10th
postoperativeday.
Patient3
A 42-year-old woman had undergone breast reconstruction using
extended latissimusdorsifasciocutaneousflap andcohesivegel-filled implant. Shehadbeenvisiting theoutpatientclinicforrepetitiveaspirationtherapyfor
chronic seroma on the donor site for 2 weeks after discharge.The mean
aspiration volumewas26.5mL.Shewasadmitted,and 1drainagetubewas
inserted and connected tothecontinuoushigh-pressurenegativesuction unit
at 200 mmHg.On the third day after application,drainage volume was
decreased to nearly 0 mL. After 2 more days,the drainage tube was
removed, and compressive dressing was applied. Chronic seroma was
successfullyresolved,andtherewasnorecurrence.
Patient4
A 54-year-old man had a chronic recurred pressure sore on the
coccygealarea.Hehad paraplegiafor20years.GradeIV pressuresorewas
noted.DebridementandconventionalNPWT withintravenousantibioticswere applied for 2 weeks.Despite repetitive adjuvant therapy,there was not enoughfreshgranulation tissue.Afterdirty margindebridement,V-Y gluteus
maximus musculocutaneous flap rotation was performed using 2 drainage
tubesinserted and connected toahigh-pressurenegativesuction unitat300
mmHg.Flapsizewasapproximately20x10cm2.Theflapseemedstableand
14
-by day and was 15 mL on the 10th postoperative day;therefore,the drain
was removed on the 14th postoperative day. There were no wound
V.DI
SCUSSI
ON
Treatmentsofwounds,especially hard-to-healwounds,havebeenthe
working basisofplasticsurgerysincethestartofthisspecializeddiscipline( Schintler,2012).However,reconstructive flap surgery is one of the main methods for these complicated wounds and many related complications –
seroma/ hematoma,wound margin dehiscence,delayed wound healing,and
evenflapfailures.
Among these complications, seroma is one of the common
postoperative complications in reconstructive surgeries.The etiology behind seromaformation remainsunclear.Severaltheorieshavebeen suggested that include disruption of vascular and lymphatic channels, shearing effects between subcutaneous surfaces and underlying musculates, creation of a surgical dead space, and an effect of inflammatory mediators generated
subsequent to tissue damage (Shin et al, 2012; Arrawal et al., 2006;,
Taghizadeh etal.2008).Themain conceptsoftheprevention and controlof
theseromaarethereduction ofmechanicalshearing effectsandpromotion of
woundhealing(Chaetal.2012;Taghizadehetal.2008;Alietal,2010;Nahas
etal.,2007).
In the various methods of preventing seroma formation, quilting suture and fibrin sealanthave been tried in many groups (Cha etal.2012;
Shin etal,2012;Alietal,2010;Nahas etal.,2007;Andrades etal.,2007).
Quiltingsuturebetweenskinflapsandunderlyinglayersiscommonlyusedto
reduceseromaformation,andstudieshaveshownthismethodtobeeffective
in a clinicalsetting (Nahas etal.,2007;Andrades et al.,2007).It might eliminate the mechanical shearing force and dead space. However, this
16
-especially when large skin paddles are harvested (Cha etal.2012).Fibrin sealant,a componentadhesive tissue composed offibrinogen and thrombin,
has been used in a number of surgical settings primarily to achieve
hemostasisand sealtissues.Themodeofaction ofthefibrin sealantistwo
pronged:itreduces the dead space between 2 planes by means oftissue
adhesion,whichcoaptstheelevatedskinflaptotheunderlyingtissues,andit
reduces hematoma and serous oozing from the involved surfaces by
enhancing hemostasis and blocking the lymph channels responsible for
drainageinto theoperativesite(Cha etal.2012;Shin etal,2012;Alietal,
2010). Some studies have reported that fibrin sealant was found to be
effective in reducing wound drainageorseroma formation (Shin etal,2012; Alietal,2010).Incontrast,itwasnotfoundtobeeffectiveinotherstudies. In conclusion,fibrin sealantdoesnotproduceuniform resultsyet(Chaetal.
2012).
Authorspaidattentiontothemethodthatreducesmechanicalshearing effectsand promoteswound healing.Theuseofnegativepressuretherapies
inwoundhealingwasfirstdescribedintheearly1990sandhassubsequently
beenadoptedinthetreatmentofcomplexsurgicalandtraumaticwounds(Lee
etal.2011).During the pastdecade,NPWT has gained favor in a wide
variety of fields. Negative-pressure wound therapy is thought to yield wound-healing benefits by increasing blood flow,promoting angiogenesis, modulating inhibitory contents in wound fluid,and inducing cellproliferation
(Timmersetal.,2005;Schitler,2012;Argentaetal.,2006;Saxenaetal.,2004;
ArgentaandMorykwas,1997).OtherreportedeffectsofNPWT includetissue
deformation with stretching of individualcells,thereby promoting cellular proliferationinthewoundmicroenvironment(Saxenaetal.,2004).
hematomaand promotion ofwound healing wasrefined toapply through the
drainage tubes withoutthe polyurethane foam.The usualnegative drainage
system providesonly 50to 90ofmmHg negativepressure.Authorstried to apply highernegative pressure continuously using wallsuction units,which
provideamaximum of300mmHg.Thelargertheareaoftheflap was,the
higherthe pressure was applied.Largerareas such as abdominoplasty area, latissimus dorsiflap donor site,and giantlipoma excision site were very effective.In contrast,the effectiveness in relatively smallareas was not different between low pressure and high pressure. In our experiences, effectivenegativepressureperareamightbethekeystoneofthistrial.
On applying high-pressurenegativesuction drain undertheflaps,the flaps seemed to be more stabilized to fix the underlying tissues than were othermethodssuchasquilting sutures(Fig.5).Ultrasonography showedthat dead space and the gap between tissues of each layer were decreased
dramatically (Fig.4).Pressurelevelwaschangedcaseby case.Thedaysof
indwelling ofthewallsuction group weresignificantly shorterthan thoseof
thecontrolgroup (P = 0.047).However,themedian oftotaldrainagevolume
and hospitalization period seemed to decrease,which was not statistically significant(P =0.441and0.183,respectively).Thismightbetheresultofthe
smallnumbers ofpatients in both groups.No serious wound complications
such as wound dehiscence,flap margin necrosis,orflap losswerefound.It means thatour refined technique mightreduce mechanicalshearing effects
and promote wound healing effectively. The advantages of continuous
negative suction over conventionalsuction drains are (1) keeping vacuum state ofclosed space;(2) keeping zero dead space;(3) rapid decrease of serum products;(4)helpfulto theflap successfordifficultwounds;(5)and, consequently,rapidreductionofthehospitalizationtime.
18
-In the resultofour study,a large flap wound or donor site that
needscontinuouscompression toreducedead spacecan beagood indication
ofhigh-pressurenegativesuction drain.Latissimusdorsiflap and transverse abdominis flap donor site,flap area after the pressure sore reconstruction,
abdominoplasty area, and defect after huge mass excision were good
examples. As the disadvantage of this method, it is presumed that
high-pressure negative suction can induce ischemia of fat tissue and fat
necrosis.However,wethink thatoursuction drain istoo smallto inducea
large area offatnecrosis,so dead space willnotbe formed by a small
amountoffatnecrosis.
Fig.5.On applying high pressurenegativesuction therapy underthe
skin flapat150~160mmHg,theflapsweremorestabilizedtofix the
underlying tissues(bluearrows)than othermethodssuchasquilting
Before using high-pressure negative suction drain,there are a few
things to be aware of. If there is a bleeding vessel in the wound,
high-pressure negative suction can cause massive bleeding.Thus,before applying high-pressure negative suction drain,meticulous hemostasis ofthe flap and recipientwound is mandatory.In addition,negative suction drain with the highestpressure (300 mmHg)can induce painfulsensation forthe patient.Therefore,ifthe patientcomplains ofpain,gradually increasing the negativepressurewillbehelpful.Becauselocalhigh pressure(>200 mmHg) can inducedrain tubecollapsenearthewallsuction bottle,regularchecking
ofthetubeisneeded,andithastobechangedtoathickertubewhenthere
isrepetitivecollapse.Inaddition,forthefreeflaporthepedicledflapwound, negativesuctiondrainneartheanastomosissiteortheflappediclecancause vascularcollapsebecauseofhighpressure.Therefore,suctiondrainshouldbe keptawayfrom theanastomosissiteortheflappedicle.
In ourexperience,the application ofnegative-pressure therapy under the clean closed wound is a new powerfultechnique in the postoperative
management of various flap surgeries, which may decrease wound
complications.Thisisthefirststudy toreportsuch anoveluseofnegative suction drain therapy.A largergroup ofpatientsand prospectiverandomized studiesforappropriatepressurelevelareneededforourrefinedtechnique.
20
-REFERENCES
1.AliSN,GillP,OikonomouD,etal.Thecombinationoffibringlueand
quiltingreducesdrainageintheextendedlatissimusdorsiflapdonorsite.
PlastReconstrSurg125:1615-1619,2010
2.AgrawalA,AyantundeAA,CheungKL.Conceptsofseromaformation
andpreventioninbreastcancersurgery.ANZ JSurg76:1088-1095,2006
3.AndradesP,PradoA,DanillaS,etal.Progressivetensionsuturesinthe
preventionofpostabdominoplastyseroma:aprospective,randomized, double-blindclinicaltrial.PlastReconstrSurg120:935-946;discussion: 947-951,2006
4.ArgentaLC,MorykwasMJ.Vacuum-assistedclosure:anew methodfor
woundcontrolandtreatment:clinicalexperience.AnnPlastSurg38:
563-576;discussion577,1997
5.ArgentaLC,MorykwasMJ,MarksMW,etal.Vacuum-assistedclosure:
stateofclinicart.PlastReconstrSurg117:127S-142S,2006
6.ChaHG,KangSG,ShinHS,etal.Doesfibrinsealantreduceseroma
afterimmediatebreastreconstructionutilizingalatissimusdorsi
myocutaneousflap?ArchPlastSurg39:504-508,2012
7.KilpadiDV,Cunningham MR.Evaluationofclosedincision
managementwithnegativepressurewoundtherapy(CIM):hematoma/
seromaandinvolvementofthelymphaticsystem.WoundRepairRegen
19:588-596,2011
8.LeeDL,RyuAY,RheeSC.Negativepressurewoundtherapy:an
tissuedefects.IntWoundJ8:406-411,2011
9.MendoncaDA,PapiniR,PricePE.Negative-pressurewoundtherapy:a
snapshotoftheevidence.IntWoundJ3:261-271,2006
10.NahasFX,FerreiraLM,GhelfondC.Doesquiltingsutureprevent
seroma in abdominoplasty? PlastReconstrSurg 119:1060-1064;discussion 1065-1066,2007
11.SaxenaV,HwangCW,HuangS,etal.Vacuum-assistedclosure:
microdeformationsofwoundsandcellproliferation.PlastReconstrSurg
114:1086-1096;discussion1097-1088,2004
12.SchererSS,PietramaggioriG,MathewsJC,etal.Themechanism of
actionofthevacuum-assistedclosuredevice.PlastReconstrSurg122: 786-797,2008
13.SchintlerMV.Negativepressuretherapy:theoryandpractice.Diabetes
MetabResRev28(suppl1):72-77,2012
14.SchmedesGW,BanksCA,MalinBT,etal.Massiveflapdonorsitesand
theroleofnegativepressurewound therapy.OtolaryngolHead Neck Surg
147:1049-1053,2012
15.ShinIS,LeeDW,Lew DH.Efficacyofquiltingsuturesandfibrinsealant
togetherforpreventionofseromainextendedlatissimusdorsiflapdonor
sites.ArchPlastSurg39:509-513,2012
16.StebbinsWG,HankeCW,PetersenJ.Ultrasound-guideddrainageof
aseromafollowingtumescentliposuction.DermatolTher24:121-124,2011
17.TaghizadehR,ShoaibT,HartAM,etal.Triamcinolonereducesseroma
re-accumulationintheextendedlatissimusdorsidonorsite.JPlast
22
-18.TimmersMS,LeCessieS,BanwellP,etal.Theeffectsofvarying
degreesofpressuredelivered by negative-pressurewound therapy on skin
perfusion.AnnPlastSurg55:665-671,2005
19.UbbinkDT,WesterbosSJ,NelsonEA,etal.A systematicreview of
topicalnegativepressuretherapy foracuteandchronicwounds.BrJSurg
국문요약
-고압력 연속 음압 흡입기를 이용한,
패쇄 창상의 치료의 새로운 해결방법
아주대학교 대학원의학과 신 승 준 (지도교수 :박 명 철) 배경 및 목적:현재까지 다양한 재건 피판 수술이 소개되고 그 성공례가 보 고되고 있지만 장액종의 형성,창상의 변연부의 괴사,지연성 회복,또는 피판의 괴사와 같은 어려운 합병증들이 꾸준히 있어오고 있다.음압치료는 이제까지 재 건수술에 있어서 개방성 창상의 회복을 도와주는 것은 여러 문헌에 소개되어왔 다.하지만,음압치료가 패쇄적인 창상에 직접적인 적용을 하는 것은 어려움이 있어왔다.이에 본 연구에서는 이러한 창상의 회복에 대한 새로운 방법을 고안하 여 성공적인 결과를 보고하고자 한다. 방법:다양한 재건수술을 받은 환자 중 고압력 연속 음압 흡입술을 받은 23 명의 환자를 대상으로 하였다.일반적은 흡입기 대신 고압력 음압을 지속적으로 재공해 줄 수 있는 음압기를 사용하였다.또한 음압은 100– 300mmHg의 범 위로 적용하였다.결과의 측정은 장액종의 빈도,수술 후 배액량,병원 재원 기 간,그 외의 다른 창상과 연관된 합병증을 수집하여 평가하였다.또한 수술 후 발생하는 사강은 초음파를 통하여 평가하였다. 결과:고압력 연속 음압 흡입술을 통하여 치료한 환자들은 창상 감염,피판 괴사와 같은 주요 합병증은 발생하지 않았지만,단 1례의 경우 퇴원 후 지연성으 로 장액종이 발생하였다.광배근의 공여부에서 삽입한 배액관의 유지기간의 경우24 -저자들의 과거 자료와 비교 시 의미 있게 감소함을 알 수 있었다 (P = 0.047). 배액량과 재원기간 역시 감소함을 나타내었으나 통계적인 유의함은 없었다.초음 파를 통해 평가한 술후 발생한 사강의 경우 대조군과 비교 시 크게 감소하였다. 결론:고압력 연속 음압 흡입치료는 간단하지만 패쇄적 창상의 치료에 있어 서 강력한 치료 방법이다.