Underlying Hemato-oncologic, Gastrointestinal-nutritional Diseases, or Prematurity May Be Risk Factors for Hypovitaminosi D in Children
9
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
수치


+2
관련 문서
Vitamin D status affects serum parathyroid hormone concentrations during winter in female adolescents: associations with forearm bone mineral density.. Budak N, Cicek B,
Conclusion: Although serum vitamin D levels were severely low in terminally ill cancer patients, we found no association between severe vitamin D deficiency
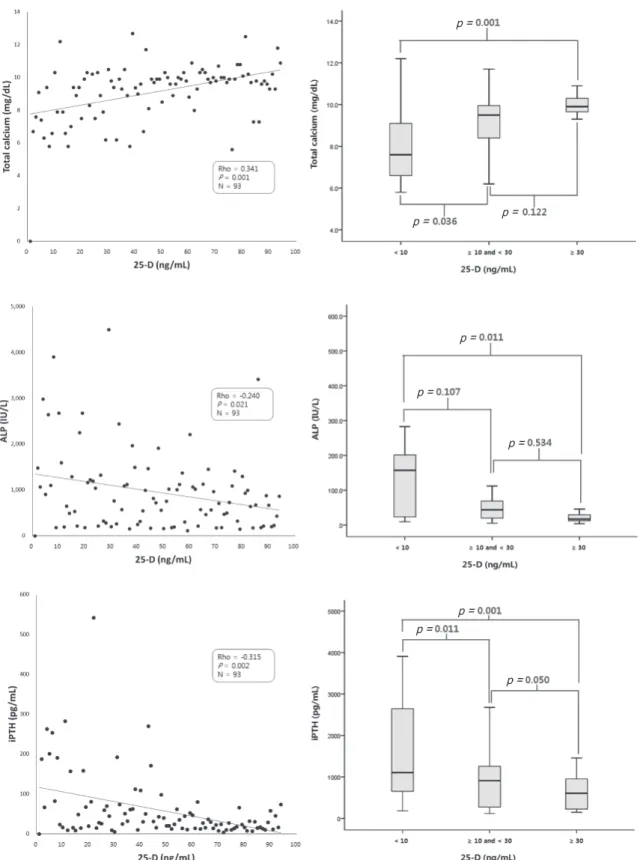
Most of the Ca in the body is stored in the bone, and serum Ca levels are regulated mainly by parathyroid hormone (PTH), vitamin D, and calcitonin via bony uptake of Ca
Serum vitamin D concentrations and associated severity of acute lower respiratory tract infections in Japanese hospitalized children.. Vitamin D deficiency and acute lower respiratory
Sahota et al.[4] previously reported that among patients with vitamin D deficiency, those with low serum PTH levels had significantly higher BMD than those with high serum
Odds ratios (95% confidence intervals) for the non-linear relationship between serum 25-hydroxy vitamin D (25(OH)D) concentration and prevalence of (A) anemia and (B) iron
Adult population-based studies have noted that low vitamin D levels were independently related to NAFLD [8-11] and a study of Korean adults showed that vitamin D deficiency
[19] classified serum 25(OH)D levels of ≤20 ng/mL as vitamin D deficiency based on data obtained from 6011 participants of the Korean National Health and Nutrition Examination
