접수일: 2008년 6월 12일, 게재승인일: 2008년 8월 20일 책임저자: 박기영, 대구시 남구 대명 4동 3056-6
705-718, 대구가톨릭대학교 의과대학 재활의학교실
Tel: 053-650-4492, Fax: 053-654-3881 E-mail: [email protected]
Gi-Young Park, M.D., Ph.D.
Department of Rehabilitation Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea
This paper describes the use of ultrasound in the evaluation of the elbow. Ultrasound has emerged as a useful imaging method for the diagnosis of joint and soft tissue pathology.
The elbow is easily amenable to ultrasound examination due to its superficial position. Ultrasound is able to assess various abnormalities of the elbow affecting tendons, mus- cles, ligaments and bursa around the elbow as well as to define the nature of soft-tissue swelling, such as a space- occupying lesion or synovial enlargement. Intra-articular loose bodies and occult fracture can be delineated with this method as well. At the cubital tunnel, ultrasound allows ac- curate imaging of the ulnar nerve and proves changes that occur in compressive syndromes. It is likely that the use of ultrasound will increase further concerning evaluation of the wide range of disorders of the elbow. (J Korean Assoc Pain Med 2008;7:90-96)
Key Words: Elbow, Ultrasound, Soft tissue
서 론
초음파 검사는 관절의 활막 공간, 관절 표면, 힘줄, 인대, 신경 및 주위 연조직 등을 침범하는 다양한 병적 상태를 평가하는 데 있어 임상적으로 유용한 정보를 제공한다.1) 근 골격계 초음파 검사는 검사자 의존, 긴 학습 기간 및 고 해 상도 초음파 장비의 필요성 등의 제한점을 가지고 있다. 그 러나 초음파 검사는 자기공명영상, 컴퓨터 단층촬영 및 컴 퓨터 단층촬영 조영술을 포함한 다른 영상 검사들에 비해 쉽게 사용할 수 있고, 비용이 저렴하며, 표면 구조에 대한 자세한 정보를 제공하고, 움직이는 동안 검사가 가능한 실
다. 팔꿈치의 초음파 검사는 다주파수 10∼12 MHz 선형 탐침자를 사용한다. 정확한 초음파 검사를 위해 팔꿈치 주 위 연조직과 뼈 구조의 해부와 기능에 관한 검사자의 적합 한 지식과 이해가 필요하다. 팔꿈치는 삼차원적으로 복잡 한 구조이므로 앞쪽, 뒤쪽, 외측 및 내측 사분면으로 나누어 표준화된 접근방식에 따라 초음파 검사를 시행할 때 올바 르게 평가될 수 있다.2-4)
본 론 1. 앞쪽 팔꿈치
앞쪽 팔꿈치를 검사하기 위해 환자는 앉거나 혹은 바로 누운 상태에서 편안하게 편 팔을 탁자나 침대 위에 둔다.
주요 검사 구조는 위팔근(brachialis muscle), 먼쪽 두갈래 근 힘줄(distal biceps tendon), 위팔동맥(brachial artery), 정 중신경, 요골신경, 갈고리 활액 오목(coronoid synovial re- cess), 앞쪽 지방 덩이(anterior fat pad) 및 요골-작은머리(ra- dio-capitular)와 도르래-척골(trochlea-ulnar) 관절 등이 있다.
먼쪽 두갈래근 힘줄은 두갈래근의 긴, 짧은 두갈래근 힘 줄들이 팔꿈치 관절 근위 7 cm 지점에서 합쳐져서 편평한 힘줄을 형성한 후 요골 거친면(radial tuberosity)에 부착한 다. 먼쪽 힘줄은 활액막으로 싸여있지 않고, 부착 근위부에 서 위팔두갈래근 노윤활낭(bicipitoradial bursa)과 접촉된 다. 위팔두갈래근 노윤활낭은 아래팔 회내 동안 마찰을 줄 이기 위해 먼쪽 두갈래근 힘줄과 요골거친면 사이에 위치 한다.5) 먼쪽 두갈래근 힘줄 완전 파열은 외상 후 앞 쪽 팔꿈 치 통증의 가장 흔한 원인 중 하나이며, 보통 무거운 물건을 들 때 발생한다. 완전 파열의 초음파 소견은 팔꿈치 관절 부위의 먼 쪽에서 힘줄을 발견할 수 없거나, 혈종의 저에코 수집(effusion)에 의해 둘러싸인 힘줄 조각이 몸쪽 뒤당김 (distraction)이 있거나, 혈종과 다양한 양의 액체로 채워진 무에코 틈이 힘줄과 요골 거친면 사이에 존재한다.6,7) 부분 파열은 뒤당김없이 저에코의 힘줄이 두꺼워지거나 혹은 얇 아지고, 힘줄 섬유의 불연속성이 없이 비정상적 물결(undu- lation) 혹은 불규칙성을 나타낸다(Fig. 1).6) 팔꿈치 회외, 회
Fig. 2. Bicipitoradial bursitis. Longi- tudinal (A) and transverse (B) ul- trasound images at the anterior as- pect of the elbow distal to the joint space showing an enlarged bicipi- toradial bursa (arrows) that locates superior and lateral to the distal bi- ceps tendon (open arrow). RT radi- al tuberosity.
Fig. 1. Distal biceps tendon partial thickness tear. Longitudinal (A) and transverse (B) ultrasound images of right distal biceps tendon showing hypoechogenicity and swelling when compared with left side. However, the continuity of tendon is maintained. RT radial tuberosity.
내, 굽힘 및 폄 동작 동안의 동적 영상은 부분 파열로부터 완전 파열을 구별하는 데 유용하다.8) 그러나 먼쪽 두갈래근 힘줄은 비스듬하게 주행하기 때문에 비등방성(anisotro- phy) 인공음영으로 인하여 병변을 확인하기가 어려울 수 있다. 부분 파열은 보존적으로 치료할 수 있으나 완전 파열 은 즉각 수술적 치료가 필요하므로 완전과 부분 파열을 구 별하는 초음파 소견들이 임상적 치료에 중요하다.
두갈래근 노윤활낭염은 다양한 원인들에 의해 발생할 수 있으나 반복된 기계적 손상에 의해 가장 흔하게 발생한다.
윤활낭염은 초음파 검사에서 먼쪽 두갈래근 힘줄 몸쪽에 위치한 저에코의 덩어리로 나타난다(Fig. 2). 윤활낭염이 작은 경우 비등방성에 의해 저에코를 나타내는 먼쪽 두갈 래근 힘줄과 구별하기가 어려울 수 있고, 삼출이 많은 경우 힘줄을 완전히 둘러싸 힘줄윤활막염과 유사한 소견을 나타 낸다. 또한 두꺼운 벽, 내부 사이막형성(septation) 및 에코 의 모습을 나타낼 수 있다.9)
결절종(ganglion)은 앞쪽 관절막에서 주로 발생하고, 아 래팔의 연부조직을 절개하면서 관절로부터 다양한 거리까 지 팽창할 수 있다(Fig. 3). 결절종과 팔꿈치 관절 강을 연결
하는 가늘고 구불구불한 줄기(pedicle)를 확인할 수 있다.10) 정중신경과 요골신경의 포착은 팔꿈치에서 드물게 발생하 며, 관절융기위 돌기(epicondylar process) 혹은 원엎침근 (pronator teres) 비대에 의해 이차적으로 발생한다. 초음파 로 팔꿈치에서 이 신경들의 병적 변화를 평가할 수 있다.
2. 외측 팔꿈치
외측 팔꿈치는 환자의 팔꿈치를 펴고, 아래팔을 회내와 회외 중간에 두거나 혹은 회내 상태에서 검사한다. 주요 검 사 구조는 공통 폄근 힘줄(common extensor tendon)과 노 쪽 곁 인대(radial collateral ligament)이다. 공통 폄 힘줄은 외측 위관절융기에서 기원하며, 짧은 노측 손목 폄근(ex- tensor carpi radialis brevis), 손가락 폄근(extensor dig- itorium), 자쪽 손목 폄근(extensor carpi ulnaris) 및 새끼 폄 근(extensor digiti minimi)을 포함한 표면 폄 근육들의 힘줄 섬유로 구성되어 있다. 공통 폄 힘줄의 깊은 섬유는 주로 짧은 노측 손목 폄근으로 구성되어 있다. 외측 위관절융기 염은 흔히 테니스 팔꿉증으로 불리며, 외측 팔꿈치의 가장 흔한 질환으로 과다사용에 의한 반복적 미세외상에 의해
Fig. 3. Ganglion cyst. Transverse ultrasound image of a soft tis- sue mass over the proximal forearm showing a multilobed an- echoic cyst (asterisk).
Fig. 5. Chronic lateral epicondylitis. Transverse ultrasound im- age of the common extensor tendon at the lateral epicondyle (LE) showing hypoechoic area and hyperechoic tiny punctuated calcifications (arrows).
Fig. 4. Lateral epicondylitis. Longitudinal ultrasound image at the lateral epicondyle (LE) revealing retracted common extensor tendon (arrow) on the radial head (RH) with a full-thickness an- echoic cleft compatible with full-thickness tendon tear.
발생하는 퇴행성 힘줄병증이다. 외측 위관절융기염은 임상 적으로 쉽게 진단할 수 있으나 초음파 검사는 힘줄 손상의 심각도를 평가할 수 있는 유용한 영상 검사이다. 주요 초음 파 소견은 부착부병증(enthesopathy)과 연관된 저에코의 힘 줄 부기, 힘줄병증에 의한 국소적 혹은 광범위한 불규칙적 원섬유성(fibrillar) 양상 및 부분 혹은 완전 파열이다(Fig.
4).11) 깊은 힘줄섬유 손상은 중간 혹은 표면 섬유 손상보다 자주 발생한다. 만성질환에서 외측 위관절융기의 겉질 불 규칙(cortical irregularity)과 힘줄내 석회화가 관찰될 수 있 다(Fig. 5).12,13) 노쪽 곁 인대는 외측 위관절융기에서 노 머
리로 뻗치며, 공통 폄근 힘줄 아래에서 가는 원섬유성 구조 로 나타나고, 손상 때 더욱 잘 구별된다.14)
3. 내측 팔꿈치
내측 팔꿈치는 환자의 팔꿈치를 펴고, 아래팔을 완전히 회외 한 자세에서 검사한다. 안쪽 팔꿈치의 주요 검사 구조 는 공통 굽힘근 힘줄(common flexor tendon)과 내측 곁 인 대(ulnar collateral ligament)이다. 공통 굽힘근 힘줄은 원엎 침근과 표면 굽힘근으로 구성되며, 안쪽 위관절상과에서 기원한다. 공통 굽힘근 힘줄은 공통 폄근 힘줄보다 짧으며, 두껍고, 관절막과 더욱 명확하게 분리되어 있다. 굽힘근 힘 줄은 초음팔 검사에서 특징적으로 고에코의 부리 혹은 삼 각형을 나타내고, 힘줄의 미묘한 변화를 발견하기 위하여 양 측 힘줄을 비교해야 한다. 안쪽 위관절융기염은 공통 굽 힘근 힘줄병증으로 외측 위관절융기염과 유사한 초음파 소 견을 보인다(Fig. 6).13,15)
내측 곁 인대는 앞쪽, 뒤쪽 및 빗 인대로 구성되어 있다.
앞쪽 인대는 앞쪽 아래쪽 안쪽 위관절상과와 갈고리돌기 (coronoid process) 사이에 위치한다. 앞쪽 인대는 내측 팔 꿈치를 펼 때 팽팽하게 되므로 팔꿈치를 편 상태에서 외반 압박 때 팔꿈치 안정성에 중요한 역할을 한다.16) 그러므로 내측 켵 인대의 변성과 파열은 던지기의 가속 단계 동안 발생하는 반복적 외반 스트레스에 의한 미세손상에 의해 발생한다. 초음파 검사는 주로 앞쪽 인대를 검사하며, 인대 는 세로 초음파 영상에서 공통 굽힘근 힘줄 아래에 고에코 원섬유성 띠 구조를 나타낸다(Fig. 6A). 초음파 검사에서 앞쪽 인대 파열 때 액에 의해 둘러싸여진 저에코의 불연속
Fig. 6. Medial epicondylitis. Longitudinal (A) ultrasound image of the common flexor tendon revealing a focal hypoechoic area (arrow) that is consistent with tendinosis. The anterior band of the ulnar collateral ligament (arrowheads) is seen attached to the flattened contour of the medial epicondyle (ME) as hyperechoic and fibrillar. Longitudinal (B) ultrasound image of the common flexor tendon showing thickened and a focal linear anehoic cleft (arrow) that is consistent with intrasubstance tear. T trochea; U ulna.
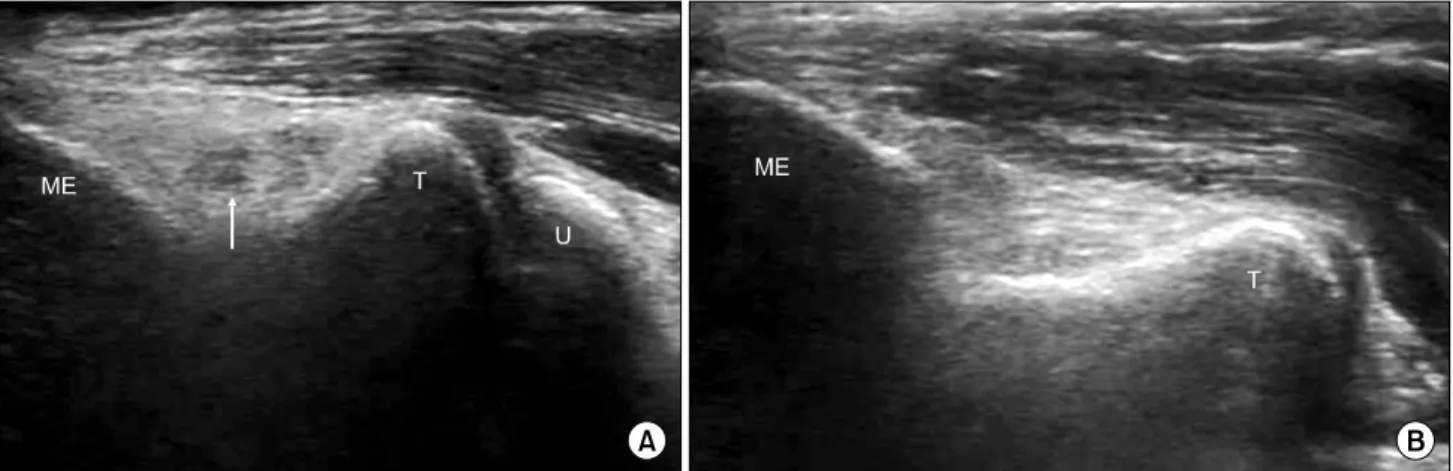
Fig. 7. Torn anterior band of the ulnar collateral ligament. Longitudinal (A) ultrasound image demonstrating disruption of normal fibers, indicating a partial-thickness tear. Compare this with the normal appearance of the anterior band of the ulnar collateral ligament (B). ME medial epicondyle; T trochea; U ulna.
적 인대를 나타낸다(Fig. 7).17) 초음파 동적 검사를 휴식 때 와 외반 스트레스를 가한 상태에서 함께 시행하여 인대의 통합성과 느슨함을 평가할 수 있다.18) 도르래 위(epitroch- lear) 림프절의 반응성 비대가 팔의 염증 혹은 패혈 상태에 서 나타날 수 있다.19)
4. 뒤쪽 팔꿈치
뒤쪽 팔꿈치는 환자의 팔꿈치 관절을 90도로 굽힌 상태 에서 검사한다. 이 자세는 관절액을 이동시켜 작은 유리 소 체(loose body)를 잘 발견할 수 있게 한다. 주요 검사 구조 는 팔꿉 굴(cubital tunnel)과 척골신경, 위팔세갈래근과 힘 줄, 팔꿈치 윤활낭(olecranon bursa) 및 뒤쪽 활액 오목이다.
팔꿉 굴은 팔꿈치, 안쪽 위관절융기, 먼쪽 활꼴 인대(ar-
cuate ligament)로 연속되는 지지띠(retinaculum)로 경계를 이룬다. 척골신경은 팔꿉 굴 안에서 난원형의 저에코 구조 로 나타난다. 팔꿈치 관절을 점차적으로 굽히는 동안 동적 초음파 검사를 시행하여 안쪽 위관절융기에 대해 척골신경 의 앞쪽 부분탈구 혹은 간헐적 탈구를 검사할 수 있다(Fig.
8).14) 척골신경의 불안정은 지지띠가 불완전하거나 없을 때 발생할 수 있으나 무증상의 일반인에서도 자주 발견된다.20) 그러나 안쪽 위관절융기에 대한 척골신경의 마찰은 신경염 을 유발하여 기능적 결핍을 야기한다. 척골신경 포착은 팔 꿉 굴 안에서 뼈곁돌기(osteophyte), 관절내 유리소체, 연조 직 석회화, 결절종 낭 및 부가 팔꿈치근(accessory anconeus muscle) 등에 의해 이차적으로 발생할 수 있다. 초음파 검 사는 팔꿈치 주위에서 척골신경의 크기와 에코 변화, 압박
dial epicondyle, until it snaps com- pletely out of the tunnel.
Fig. 9. Cubital tunnel syndrome. Longitudinal ultrasound image at the medial epicondyle (ME) demonstrating the ulnar nerve (arrow), which shows focal swelling at the elbow joint (EJ) level.
Fig. 10. Retrocondylar compression syndrome. Longitudinal ul- trasound image at the medial epicondyle (ME) demonstrating the ulnar nerve (arrow), which shows diffuse swelling from prox- imal end of medial epicondyle (PME) to elbow joint (EJ) level.
원인과 위치를 확인할 수 있다(Fig. 9, 10).21) 척골신경은 팔꿉굴 증후군에서 특징적으로 굴 안에서 납작해져 있고, 몸쪽에서 부어있으면서 저에코를 나타내고, 척골신경의 단 면적은 증상이 없는 반대쪽과 건강한 일반인에 비해 의미 있게 증가된다.22) 초음파 검사는 팔꿈치에서 척골신경의 형태학적 변화와 손상 범위를 평가할 수 있어 팔꿈치 부위 척골신경 손상을 가진 환자의 선별과 추적 관찰 검사로 사 용될 수 있다.21)
위팔세갈래근 힘줄은 낙상과 같이 수축된 위팔세갈래근 에 대해 팔꿈치를 구부릴 때 파열된다. 초음파 검사에서 액 에 의해 둘러싸여 있으면서 뒤당겨진 힘줄을 발견할 수 있 다.23) 완전 파열은 임상적 소견만으로 쉽게 확인될 수 있으 나 초음파 검사는 외상 후 부종과 통증으로 인하여 병태 확인이 어려울 때 부분 파열을 진단하는 데 도움이 될 수
있다.
팔꿈치 윤활낭염은 주로 반복적 국소 외상에 의해 이차 적으로 발생한다. 윤활낭염은 초음파 검사에서 팔꿈치와 피부사이에 위치한 저에코의 윤활낭 액 수집 소견을 나타 낸다(Fig. 11A). 윤활낭내 액은 출혈 혹은 패혈 윤활낭염에 서 에코발생을 보일 수 있고, 윤활낭 벽의 비후와 색상과 운동 도풀러 영상에서 증가된 혈관분포정도가 동반되어 나 타날 수 있다(Fig. 11B).24) 그러나 패혈 윤활낭염은 윤활낭 액과 균 배양 검사에 의해 확진할 수 있으므로 초음파 검사 는 윤활낭 액을 바늘 흡인하는 데 도움을 줄 수 있다. 팔꿈 치 오목은 고에코의 뒤쪽 지방 덩이에 의해 채워지므로 방 사선적으로 지방 덩이의 뒤쪽 전위는 팔꿈치 관절 삼출의 간접적 징후로 잘 알려져 있다. 초음파 검사는 팔꿈치 오목 에서 지방 덩이의 전위와 삼출 혹은 활액 누스(pannus)에
Fig. 11. Olecranon bursitis. Longitudinal (A) ultrasound image of a soft tissue mass over the olecranon process (OP) shows marked distension of the olecranon bursa, which exhibits anechoic fluid collection. Transverse (B) color Doppler image shows hyperemic flow signals, typically rim-like fashion.
Fig. 12. Arthritis of the elbow. Longitudinal (A) and transverse (B) ultrasound images of the olecranon fossa demonstrating anechoic fluid filling the posterior recess (open arrows). The joint effusion displace the posterior fat pad (arrows).
의한 관절 공간의 팽창을 확인할 수 있다(Fig. 12).25) 팔꿈 치 관절은 관절내 유리 소체가 흔한 관절로 대부분 앞쪽과 뒤쪽 활액 오목에 위치한다. 초음파 검사에서 조각들은 뒤 쪽 소리그림자(acoustic shadowing)를 가진 고에코 영상으 로 나타난다. 활액 삼출이 있는 경우 활액이 조각을 완전히 둘러싸며, 관절을 구부리거나 탐침자의 압력에 의해 조각 이 전이될 때 관절내 유리 소체를 진단할 수 있다. 삼출이 없는 경우 위팔뼈 겉질과 지방 덩이 사이에서 조각이 보이 면 유리 소체의 관절내 존재를 확인할 수 있다.26)
결 론
팔꿈치는 상지의 중요한 활액 경첩(hinge) 관절로 모든 연령에서 흔하게 근골격계 증상을 나타낸다. 초음파 영상 소견은 환자의 증상과 최고 누름통증의 위치와 직접적으로 연관할 수 있고, 증상이 없는 반대편과 비교하여 쉽게 비교 할 수 있다. 초음파 검사는 팔꿈치에서 주위 힘줄과 인대와 같은 관절 주위 구조와 더불어 관절 삼출, 유리 소체 및 윤 활낭 등도 평가할 수 있어 검사자의 풍부한 경험과 뛰어난
Derchi LE. Ultrasound of the elbow. Eur J Ultrasound 2001;14:21-7.
4. Martinoli C, Bianchi S, Giovagnorio F, Pugliese F. Ultra- sound of the elbow. Skeletal Radiol 2001;30:605-14.
5. Skaf AY, Boutin RD, Dantas RW, Hooper AW, Muhle C, Chou DS, et al. Bicipitoradial bursitis: MR imaging find- ings in eight patients and anatomic data from contrast mate- rial opacification of bursae followed by routine radiography and MR imaging in cadavers. Radiology 1999;212:111-6.
6. Miller T, Adler RS. Sonography of tears of the distal biceps tendon. Am J Roentgenol 2000;175:1081-6.
7. Lozano V, Alonso P. Sonographic detection of the distal bi- ceps tendon rupture. J Ultrasound Med 1995;14:389-91.
8. Chew ML, Giuffrè BM. Disorders of the distal biceps bra- chii tendon. Radiographics 2005;25:1227-37.
9. Liessi G, Cesari S, Spaliviero B, Dell'Antonio C, Avventi P. The US, CT and MR findings of cubital bursitis: a report of five cases. Skeletal Radiol 1996;25:471-5.
10. Steiner E, Steinbach LS, Schnarkowski P, Tirman PFJ, Genant HK. Ganglia and cysts around joints. Radiol Clin North Am 1996;34:395-425.
11. Connell D, Burke F, Coombs P, McNealy S, Freeman D, Pryde D, et al. Sonographic examination of lateral epi- condylitis. AJR 2001;176:777-82.
12. Lin J, Jacobson JA, Fessell DP, Weadock WJ, Hayes CW.
An illustrated tutorial of musculoskeletal sonography. 2.
Upper extremity. AJR 2000;175:1071-9.
13. Park GY, Lee SM, Lee MY. Diagnostic value of ultra-
mic sonography with valgus stress to assess elbow ulnar collateral ligament injury in baseball players. Skeletal Radiol 2002;31:671-6.
19. Barr LL, Kirks DR. Ultrasonography of acute epitrochlear lymphadenitis. Pediatr Radiol 1993;23:72-3.
20. Kim BJ, Date ES, Lee SH, Yoon JS, Hur SY, Kim SJ.
Distance measure error induced by displacement of the ul- nar nerve when the elbow is flexed. Arch Phys Med Rehabil 2005;86:809-12.
21. Park GY, Kim JM, Lee SM. The ultrasonographic and elec- trodiagnostic findings of ulnar neuropathy at the elbow.
Arch Phys Med Rehabil 2004;85:1000-5.
22. Chiou HJ, Chou YH, Cheng SP. Cubital tunnel syndrome:
diagnosis by high-resolution ultrasonography. J Ultrasound Med 1998;17:643-8.
23. Kaempffe FA, Lerner RM. Ultrasound diagnosis of triceps tendon rupture. A report of 2 cases. Clin Orthop 1996;332:
138-42.
24. Newman JS, Adler RS, Bude RO, Rubin JM. Detection of soft-tissue hyperemia: value of power Doppler sonography.
AJR Am J Roentgenol 1994;163:385-9.
25. DeMaeseneer M, Jacobson JA, Jaovisidha S, Lenchik L, Ryu KN, Trudell DR, et al. Elbow effusions: distribution of joint fluid with flexion and extension and imaging implications. Invest Radiol 1998;33:117-25.
26. Bianchi S, Martinoli C. Detection of loose bodies in joints.
Radiol Clin North Am 2000;37:679-90.