164
• 교신저자:민승기, 국립경찰병원 비뇨기과 서울 송파구 가락본동 58번지 우 138-708
Tel: 02-3400-1263, Fax: 02-431-3192, E-mail: [email protected] Received: August 31, 2012
Revised: September 16, 2012 Accepted: October 5, 2012
대한민국 40-50대 남성에서 만성전립선염 증상점수 (NIH-CPSI)와 국제 발기능 지수 (IIEF-5)의 관계 분석
국립경찰병원 비뇨기과
조인창∙김성빈∙김유석∙최재영∙민승기
[Abstract]
Analysis of Correlation between The National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) and International Index of Erectile
Function (IIEF-5) among Korean Males Aged 40-50s
In Chang Cho, Sung Bin Kim, Yoo Seok Kim, Jae Young Choi, Seung Ki Min
From the Department of Urology, National Police Hospital, Seoul, Korea
Purpose: Analyzed the correlation between the National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) and International Index of Erectile Function (IIEF-5) from questionnaires among Korean 40-50s male.
Materials and Methods: From September 1, 2011 to December 31 2012, we conducted a survey tar- geting 1032 Korean males who were had medical examinations in National Police Hospital, Using NIH-CPSI and IIEF-5. After explaining the content of the NIH-CPSI and IIEF-5, the paper was checked by volunteers in person, and the results were then collected. The subjects were limited to Korean males in their 40-50s. We analyzed the collected questionnaires.
Results: The average age of 1032 volunteers was 50 years old (42-59), and the average of NIH-CPSI total
scores was 7.1±5.5. The average of IIEF-5 total scores was 17.4±6.5. IIEF-5 category was divided into
Normal 385 (37.3%), Mild 296 (38.7%), Mild-Moderate 215 (20.8%), Moderate 98 (9.5%), and Severe 38
persons (3.7%). Among total volunteers, 72 persons were Chronic prostatitis like symptom patients (6.9%),
and whose NIH-CPSI average of pain score (total 21), voiding score (total 10), quality of life score (total 12)
and total scores were 7.6±3.1, 4.3±2.5, 5.8±2.3, and 17.8±6.7, respectively. There were moderate correlations
of pain score, voiding score, quality of life score, but not significant (Pearson's coefficient of correlations
<0.501). An average of total IIEF-5 scores in chronic prostatitis - like symptoms in the present group was 14.0±6.8. It was significantly lower than in the in the absent group. Prostatitis-like symptoms in the present group had more severe degrees of erectile dysfunction than absent group (p=0.002). Assessing each NIH-CPSI category score and total score affected to total IIEF-5 score, we analyzed the correlation between NIH-CPSI and IIEF-5 using regression analysis. There were all negative correlations between IIEF-5 and Pain score (t=-6.199, r
2=0.036, p=0.000), voiding score (t=-0.157, r
2=0.025, p=0.000), QOL score (t=-7.845, r
2=0.056, p=0.000), and total score (t=-9.366, r
2=0.078, p=0.000). Having analyzed correlations between each score of NIH-CPSI groups and IIEF-5 score by using multiple regression analysis, there were statistically significant difference negative correlations between pain score and IIEF-5 (t=-2.646, p=0.008), QOLscore (t=-4.219, p=0.000), and age (t=-3.135, p=0.002), but not to voiding score (t=0.628, p=0.530).
Conclusions: The higher the NIH-CPSI score, especially for pain and QOL scores play a larger role, and adversely affects erectile function of chronic prostatitis like symptom patients in Korean males aged 40-50s. (Korean J UTII 2012;7:164-171)
Key Words: Prostatitis, Erectile dysfunction, Questionnaires
서 론
만성전립선염은 성인 남성의 약 50%가 일생에 한 번 정도는 그 증상을 경험할 정도로 흔한 질환이며
1그 특징적 증상인 비뇨생식기의 통증 및 사정시 통 증은 성욕감소, 발기부전을 유발하여 삶의 질 저하 를 초래하는 것으로 알려져 있다.
2현재까지의 보고 에 의하면 만성전립선염은 세균성에 비해 비세균성 원인이 월등히 많으며
3이로 인해 아직까지 병리학 적 기전은 거의 알려지지 않은 상태로 이전의 감염 병력, 골반저 고혈압, 국소적 화학변화, 관류장애 등 이 가설로 등장하였지만 여전히 논의 중이다.
4그래 서 만성전립선염은 만성 골반통 증후군 (Chronic Pelvic Pain Syndrome; CPPS)과 거의 동등한 의미로 통용되며 증후군의 개념에서 치료의 목적은 증상의 개선에 초점이 맞추어져 있다. 성기능 장애는 남성 들의 삶의 질을 저하시키는 주요한 질병 중 하나이 며
5흡연, 음주, 운동 등의 생활 양식적 원인, 신경학 적, 호르몬적, 정신적 원인 등 다양한 원인에 의해 발생 한다.
6,7현재는 경구용 phosphodiesterase 5형 (PDE5) 억제제가 성기능 장애의 일차 치료제로 널
리 쓰이지만 만성전립선염 증상으로부터 유발되는 성기능 장애의 경우 그 증상의 조절은 원인 교정을 통한 치료가 가능하다는 점에서 의의가 있다. 이러 한 점에 착안, 저자들은 만성전립선염 증상을 가진 환자들에서 성기능 장애의 유병률을 알고자 하였고 현재 전 세계적으로 널리 쓰이며 타당도를 인정받은 미 국립보건원 만성전립선염 증상지수 (National Institute of Health Chronic Prostatitis Symptom Index;
NIH-CPSI)와 국제 발기능 지수 (International Index of Erectile Fucntion; IIEF)를 이용한 설문조사를 시 행, 두 지표간의 상관관계를 분석하였다.
대상 및 방법
1. 대상
2011년 9월 1일부터 2012년 12월 31일까지 건강검
진 목적으로 본원을 방문한 1,032명의 40-50대 대한
민국 남성을 대상으로 설문조사를 시행하였다. 설문
전 과거력 및 가족력 조사하여 이전에 만성전립선염
및 발기부전으로 진단, 치료를 받은 경우는 대상에
서 제외하였다. 대상의 지역별 분포는 각 시도별 인
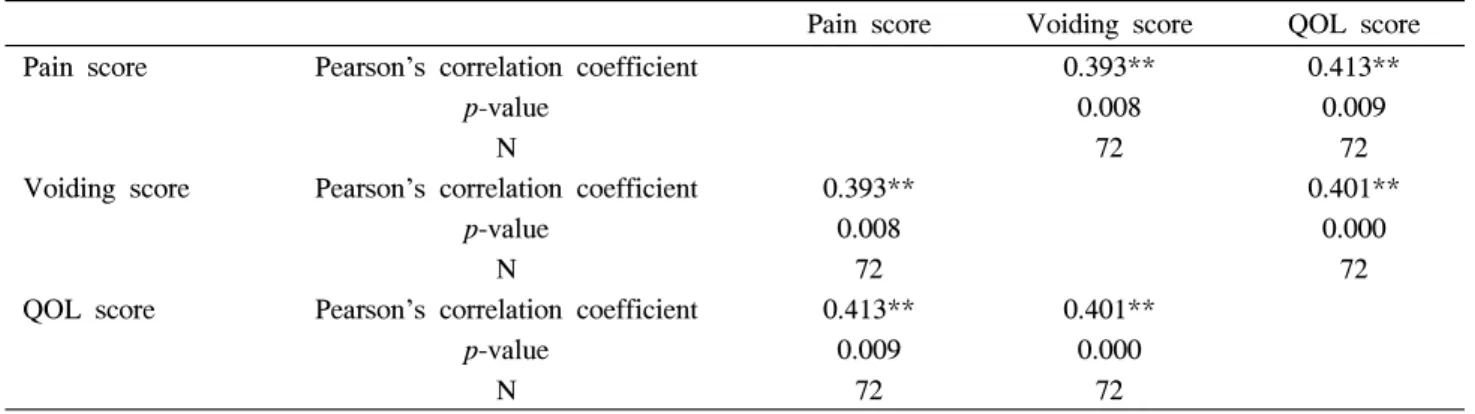
Table 2. Correlation of NIH-CPSI pain score, voiding score and QOL score in chronic prostatitis-like symptom patients with Pearson's correlation
Pain score Voiding score QOL score
Pain score Pearson's correlation coefficient 0.393** 0.413**
p-value 0.008 0.009
N 72 72
Voiding score Pearson's correlation coefficient 0.393** 0.401**
p-value 0.008 0.000
N 72 72
QOL score Pearson's correlation coefficient 0.413** 0.401**
p-value 0.009 0.000
N 72 72
Table 1. NIH-CPSI scores according to the presence or absence of chronic prostatitis-like symptoms
Pain score Voiding score QOL score Total score Prostatitis-like Symptom absence (n=956) 0.8±1.5 2.4±2.1 3.1±2.2 6.3±4.5 Prostatitis-like Symptom presence (n=72) 7.6±3.1 4.3±2.5 5.8±2.3 17.8±6.7
p-value <0.0001 <0.0001 <0.0001 <0.0001
구에 비례하여 전국적으로 고른 분포를 보였다.
2. 방법
국문판 NIH-CPSI와 IIEF-5를 이용하여 설문조사를 시행하였고 해당 대상자들에게 각 항목에 대하여 충 분한 설명을 한 후, 대상자들이 직접 기록하게 하여 기록된 설문지를 수집하였다. NIH-CPSI는 통증영역 6개 문항 (통증의 위치와 형태 4개, 통증의 빈도와 정도 2개), 배뇨영역 2개 문항 (잔뇨감, 빈뇨), 삶의 질 영역 3개 문항 (통증 및 배뇨에 의한 영향 2개, 삶의 질 1개)로 구성되어 있고 IIEF-5는 발기능, 절 정감, 성적욕구, 성교만족도 및 전반적 성생활 만족 도의 5개 영역에 각각 1문항씩으로 구성되어 있다.
저자들은 수집된 설문지를 분석하여 회음부 통증이 나 불편감과 사정시 통증이나 불편감을 호소하며 NIH-CPSI 총 통증점수의 합이 4점 이상일 경우 만 성 전립선염 증상이 있다고 정의하였으며 IIEF-5는 경증 (17-21), 경중등증 (12-16), 중등증 (8-11), 중증 (5-7)으로 분류하였다. 그리고 만성전립선염 유증상 군 내에서 NIH-CPSI의 통증, 배뇨, 삶의 질 점수와 IIEF-5 점수와의 상관관계를 분석하였다.
3. 통계 분석
수집된 설문지 내에서 상기된 만성전립선염 증 상의 정의에 맞는 대상자를 추출해 유병률을 계산 하였고 전체 설문대상자와 만성전립선염 유증상군 간의 NIH-CPSI 및 IIEF-5 평균 점수 차이를 in- dependent samples T-test를 이용해 비교하였다. 또한 만성전립선염 유증상군의 NIH-CPSI 각 영역 점수 간 상관관계를 Pearson's correlation analysis를 이용 하여 검증하였고 NIH-CPSI 각 영역 점수 및 총점 과 IIEF-5 총점과의 관계를 regression analysis를 이 용해 분석하였다. 통계 분석은 SPSS version 18.0을 이용하여 수행하였으며 p-value가 0.05 미만일 경우 를 통계학적으로 유의성이 있다고 하였다.
결 과
1. 만성전립선염 증상과 발기부전 유병률의 산출
전체 설문대상자 1,032명의 평균 연령은 50세
(42-59)였으며 이들의 NIH-CPSI 각 영역 점수와 총점
Prostatitis-like symptom presence (Mean IIEF-5 score=14.2±6.8)
Prostatitis-like symptom absence (Mean IIEF-5 score=17.7±6.4)
Severe Moderate Mild to moderate Mild
Normal
p=0.0020 10 20 30 40 (%)
Fig. 1. IIEF-5 scores according to the presence or absence of chronic prostatitis-like symptoms 평균은 1.3±2.4점 (통증), 2.6±2.2점 (배뇨), 3.3±2.3점
(삶의 질), 7.1±5.5점 (총점)이고 IIEF-5 총점 평균은 17.4±6.5점 이었다. IIEF-5상 정상 385명 (37.3%), 경 증 396명 (28.7%), 경중등증 215명 (20.8%), 중등증 98명 (9.5%), 중증 38명 (3.7%)이었다. 전체 설문대상 자 중 회음부 통증이나 불편감과 사정시 통증이나 불편감을 호소하며 NIH-CPSI 총 통증점수의 합이 4 점 이상인 경우는 72명 (6.9%)이었다.
2. NIH-CPSI와 IIEF-5 점수 분석
만성전립선염 유증상군을 대상으로 하여 NIH- CPSI를 분석하였을 때 통증, 배뇨, 삶의 질 점수 및 총점의 평균은 각각 7.6±3.1점, 4.3±2.5점, 5.8±2.3점, 17.8±6.7점이었고 이는 각 영역과 총점이 무증상군 에 비해 유의하게 높았다 (p=0.000) (Table 1). 통증, 배뇨, 삶의 질 각 영역간의 상관관계는 관찰되었으 나 정도는 미약하였다 (Table 2). 또한 만성전립선염 유증상군에서 IIEF-5 총점 (25점) 평균은 14.0±6.8점 으로 무증상군에 비해 유의하게 낮았으며 정상 16 명 (21.1%), 경증 23명 (30.3%), 경중등증 17명 (22.4%), 중등증 13명 (17.1%), 중증 7명 (9.2%)으로 무증상군에 비해 중증의 비율이 더 높았다 (Fig. 1).
3. NIH-CPSI와 IIEF-5의 상관관계 분석
NIH-CPSI 각 영역의 점수 및 총점이 IIEF-5 총점
에 영향을 끼친다는 가정 하에 NIH-CPSI와 IIEF-5 의 관계를 회귀분석을 이용하여 분석하였다. 통증, 배뇨, 삶의 질, 총점 모두 IIEF-5 점수와 음의 상관 관계가 있었고 (Table 3), NIH-CPSI의 각 영역 점수 와 IIEF-5 점수와의 관계를 연령을 보정하여 다중 회귀분석을 하였을 때 통증점수, 삶의 질 점수와 나이가 증가할수록 IIEF-5 점수는 감소하는 경향을 보였으나 (각각 t=-2.646, p=0.008; t=-4.219, p=0.000;
t=-3.135, p=0.002), 배뇨점수 (t=0.628, p=0.530)는 IIEF-5 점수와 유의한 상관관계가 없었다 (Table 4).
고 찰
만성전립선염은 다양한 임상경과를 나타내는 비
뇨기계 질환으로 최근 증가 추세이며 연구마다 차이
는 있지만 성인 남성에서의 유병률은 5-9%로 알려
져 있다. 특히 우리나라의 경우 개원비뇨기과 방문
환자의 15-25%가 만성전립선염 환자로 추정된다는
보고도 있을 만큼 매우 흔한 질환이다.
8만성전립선
염의 가장 특징적인 증상은 통증과 관련된 증상으로
NIH-CPSI final validation study에서는 회음부 통증이
나 불쾌감, 그리고 사정시 통증이나 불쾌감이 만성
전립선염 환자에서 가장 특징적인 증상이라고 하였
으며 위의 두 증상이 한 가지 이상 있으면서
NIH-CPSI 통증 점수 합이 4점 이상일 경우 만성전
립선염 증상이 있다고 정의하였다.
9본 연구에서 조
사된 만성전립선염 증상 유병률도 6.9%로 기존에
Table 4. Correlation between NIH-CPSI pain score, voiding score, QOL score, total score, age and IIEF-5 total score in all patients with multiple regression analysis
Pain score Voiding score QOL score Age
IIEF-5 score (r2=0.072)
t=-2.646 B=-0.246 p=0.008
t=0.628 B=0.076 p=0.530
t=-4.219 B=-0.533 p=0.000
t=-3.135 B=-0.130 p=0.002
Table 3. Correlation between NIH-CPSI pain score, voiding score, QOL score, total score, age and IIEF-5 total score in all patients with single regression analysis
Pain score Voiding score QOL score Total score Age
IIEF-5 score
t=-6.199 r2=0.036 B=-0.507 p=0.000
t=-0.157 r2=0.025 B=-0.462
p=0.000
t=-7.845 r2=0.056 B=-0.673 p=0.000
t=-9.366 r2=0.078 B=-0.328 p=0.000
t=-4.686 r2=0.021 B=-0.193 p=0.000