48
• 교신저자:이동현, 이화여자대학교 의학전문대학원 비뇨기과학교실 서울시 양천구 목동 911-1 우 158-710
Tel: 02-2650-5157, Fax: 02-2654-3682, E-mail: [email protected] Received: February 23, 2011, Accepted: March 20, 2011
만성 비세균성 전립선염 환자의 전립선액에서 interleukin-1β의 변화
이화여자대학교 의학전문대학원 비뇨기과학교실 윤하나∙이동현
[Abstract]
Changes of Interleukin-1β in the Prostate Secretions of Chronic Nonbacterial Prostatitis Patients
Hana Yoon, Dong Hyeon Lee
From the Department of Urology, Ewha Womans University School of Medicine, Seoul, Korea
Purpose: To measure changes in prostate cytokine secretion in chronic non-bacterial prostatitis (NBP) patients and examine the clinical usefulness of these changes in differentiating the pathophysiologic mech- anism of NBP and subsequent selection of treatment modalities.
Materials and Methods: Sixty male patients were diagnosed with chronic NBP, and a control group comprised of 30 male patients without clinical evidence of NBP were enrolled in this study. Prostate secre- tion (centrifuged VB3) was analyzed at the initialdiagnosis and 8 weeks after treatment initiation. Patients who showed more than 10 white blood cells (WBCs)/high power field (HPF) 8 weeks after treatment ini- tiation were categorized into group A. Group B patients had less than 3 WBCs/HPF. Group B was further subclassified into two groups according to presence of symptoms after treatment: Bp (symptom-persisted) and Br (symptom-resolved). IL-1β, C3, C4, IgG were measured and the results were analyzed.
Results: There were significant differences in the IL-1β level in the control group compared to group A, Bp and Br (p<0.05). C3, C4, IgG showed higher levels in groups A and B than in the control group, albeit without statistical significance (p>0.05).
Conclusions: Elevated IL-1β in group Bp suggests that chronic NBP patients who did not respond to treatment could exhibitclinical manifestations of autoimmune reactions rather than infection of external origin. We suggest that a more advanced diagnostic technique using cytokine at the initial stage of disease manifestation tohelp clinicians avoid unnecessary antibiotic treatment and manage the condition more effectively. (Korean J UTII 2011;6:48-53)
Key Words: Autoimmunity, Cytokines, Prostatitis
INTRODUCTION
Chronic NBP and chronic pelvic pain syndrome are common and important problems in adult men. Most patients are offered no explanation as to the cause of their disease and are empirically treated with pro- longed and repeated courses of antimicrobial agents without substantial relief.
The definitive pathophysiology of chronic NBP has not been clearly identified. The chronic, relapsing, and episodic nature of the patient’s symptoms, along with the frequent concurrence of irritating symptoms suggested to us that the chronic prostatitis and chron- ic pelvic pain syndrome may have an autoimmune component.
Cytokines are important factors which act locally to initiate and modulate immune reactions. We hypothe- sized that certain proinflammatory cytokines might be acting as the crucial factors for the progression of the chronic NBP and chronic pelvic pain syndrome as a consequence of certain autoimmune reactions. We thus measured cytokine changes in the prostate secre- tion of chronic NBP patients and examined the clin- ical usefulness of these changes in differentiating the pathophysiologic mechanism of NBP and selecting ap- propriate treatment modalities.
MATERIALS AND METHODS
Sixty men diagnosed with chronic NBP included in the study as subjects, and 30 healthy men who did not have any clinical evidence of NBP with no WBC in EPS were included in the study as a control group.
Patient evaluation included a complete medical his- tory, a physical examination, and a urinalysis with cultures and microscopic examination of the EPS. All of the subject patients were included only if i) there are no medical history of active autoimmune disease;
ii) no history of anti-inflammatory medications within
2 months; iii) there is no active urethritis or acute prostatitis. Diagnosis of chronic NBP was based on the guideline from Chronic Prostatitis Collaborative Research Network (CPCRN).1 Urinalysis and micro- scopic examination of prostatic secretion in the con- trol group were all clear.
Prostate fluid was obtained by massage of the pros- tate gland and divided into two parts. Half of the fluid was stored at -80C until used for cytokine analysis.
The remaining fluid was placed under a coverslip and examined for whithe blood cells (WBCs) in five high power fields (HPF). Standard microbiologic Methods were used to quantify and identify all microorganisms.
EPS examination was performed twice; baseline and 8 weeks after the course of treatment. Treatments were conventional medical treatments consisted of antibiotics (fluoroquinolone 750mg P.O. per day) with anti-in- flammatory agents. Adjuctive management such as hot sitz bath or regular ejaculation were informed to the patients as needed. In patients group, according to the result of post-8 week treatment EPS, they were divided into two groups; patients with more than 10 WBCs/HPF were classified as group A. Group B was defined as those subjects having less than 3 WBCs/HPF. Group B subjects were further classified as persistent symptom group (Group Bp) and symptom resolution group (Group Br). IL-1β, C3, C4, and IgG levels in the prostate fluid were measured 8 weeks af- ter the treatment in all of the patients. Cytokine levels were measured by using commercial enzyme-linked im- munosorbent assay (ELISA) kits (R&D systems, Inc.
MN, USA.). The methodology was to add 150ul of as- say diluent HD1C to the microtiter well and then add 150ul of urine sample. The combined assay and sam- ple were then [sealed and] incubated for 14hours at room temperature. After incubation the mictotiter wells were washed 4 times with the wash buffer. 200ul of conjugated polyclonal antibody directed against IL-1β is then added to the cleaned microtiter and incubated for 3 hours at room temperature. The wells are then wash-
ed 4 times with wash buffer solution. The color devel- oping process was performed with the substrate sol- ution and the amplifier solution (provided from the kit) and an incubation period 45 minutes at room temper- ature for each process. A stop solution was then added and the plates were read within 30 minutes at 490nm., which corrects OD450 reading by subtracting OD650. IL-1β values are obtained from the optical density val- ues using a standard curve in the ELISA. All measure- ments were performed in duplicate. The lower limit of detection was 0.1 pg/ml. Other cytokines, C3, C4, IgG were also measured by Methods similar to those de- scribed above.
Data was analyzed and compared using a Student’s t-test and ANOVA. P-values <0.05 were considered to be significant.
RESULTS
Among 90 subjects, all of the patients except healthy control showed more than 10 WBCs/HPF in EPS ex- amination before starting medications. After 8 weeks of medications with antibiotics and anti-inflammatory agents, 27showed more than 10 WBCs/HPF in their follow up EPS after 8 weeks of treatment (group A), 33 subjects showed less than 3 WBCs/HPF in the EPS study after 8 weeks of treatment (group B). Among group B subjects, 18 (group Bp) showed persistent symptoms of chronic prostatitis/chronic pelvic pain syn- drome; frequency, residual urine sensation, perineal pain, penile pain, scrotal pain. 15 out of the 33 group B subjects showed resolution of their distressing symp- toms after the treatment (group Br).
The mean age of the subjects in group A (n=27) was 42.110.5 years old. In group Bp (n=18), the mean age was 41.111.7 years old; in the group Br (n=15), the mean age was 40.2 12.5 years old. The mean age of the healthy control group (n=30) was 39.7 10.8 years old. There were no significant differ- ences of mean age of patients among group A, group
Bp, group Br, and the control group (p>0.05).
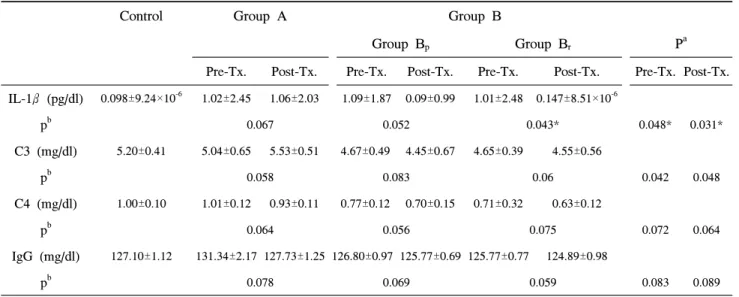
Baseline cytokine analysis of the four groups (group A, group Bp, group Br, and control group) are shown in Table 1. There were significant differences in IL-1β level of the control group compared with group A and B (Bp and Br) (pre-Tx. p=0.048, post-Tx. p=0.031) IL-1β expression was increased af- ter 8 weeks of treatment in group A but there was no statistical significance (p=0.067). In group Br, IL-1 β level is significantly decreased after treatment (p=0.043). In group Bp, expression of IL-1β was de- creased with borderline significance (p=0.052).
Pre-treatment C3 level demonstrated lower in all four groups with statistical significance (p=0.042).
Post-treatment C3 level also demonstrated significantly lower in groups Bp and Br, meanwhile, the level was higher than control group in group A (p=0.048).
Although elelvation of expression with borderline sig- nificance in post-treatment group A, there were stat- istically no significance between pre- and post-trea- ment within each group.
Pre-treatment C4 level was not significantly differ- ent in group A, Bp, and Br when compared with con- trol group (p=0.072). Althoughpost-treatment C4 level showed decreasing tendency in each group, there were no significant differences between pre- and post-treat- ment within each group (Table 1). When compared with controlgroup, there also were no significant dif- ferences in group A, Bp, and Br (p=0.064).
Ig G level showed no significant differences among four groups (control, group A, group Bp and group Br) (Tabe 1). Although level of Ig G was lower after 8 week-treatment in group A, Bp and Br, there were no statistical significance between pre- and post-treat- ment within groups (Table 1).
DISCUSSION
The cause of chronic prostatitis/chronic pelvic pain syndrome is unknown. Infection has been regarded as
Table 1. Cytokine levels baseline and among different groups 8 weeks after treatment
Control Group A Group B
Group Bp Group Br Pa
Pre-Tx. Post-Tx. Pre-Tx. Post-Tx. Pre-Tx. Post-Tx. Pre-Tx. Post-Tx.
IL-1β (pg/dl) 0.098±9.24×10-6 1.02±2.45 1.06±2.03 1.09±1.87 0.09±0.99 1.01±2.48 0.147±8.51×10-6
pb 0.067 0.052 0.043* 0.048* 0.031*
C3 (mg/dl) 5.20±0.41 5.04±0.65 5.53±0.51 4.67±0.49 4.45±0.67 4.65±0.39 4.55±0.56
pb 0.058 0.083 0.06 0.042 0.048
C4 (mg/dl) 1.00±0.10 1.01±0.12 0.93±0.11 0.77±0.12 0.70±0.15 0.71±0.32 0.63±0.12
pb 0.064 0.056 0.075 0.072 0.064
IgG (mg/dl) 127.10±1.12 131.34±2.17 127.73±1.25 126.80±0.97 125.77±0.69 125.77±0.77 124.89±0.98
pb 0.078 0.069 0.059 0.083 0.089
Group A: patients with more than 10 WBCs/HPF in EPS Group, B: patients having less than 3 WBCs/HPF in EPS after 8 weeks of treatment. Group Bp: patients with persistent symptom group in Group B, Group Br: patients without symptoms after treatment in Group B, Tx.:treatment, p: p-value, a: significant difference compared with control group in group A, Bp, Br, b: compared values between baseline and post-treatment, *: p<0.05
the main etiology for this disease. However, most pa- tients with chronic prostatitis/chronic pelvic pain syn- drome fail to achieve a durable and lasting remission of symptoms with antimicrobial therapy. Some inves- tigators have thus suggested participation of the auto- immune process in the pathophysiology of the chronic prostatitis/chronic pelvic pain syndrome.2-4
This hypothesis, that chronic prostatitis/chronic pel- vic pain syndrome represents an autoimmune disease in some patients, is supported by observations such as the chronic, relapsing, and episodic nature of the symptoms. Furthermore, the prostate is commonly found to contain inflammatory infiltrates when pros- tate tissue is removed for any reason (typically for prostate cancer or benign prostate hypertrophy).5,6 Interleukin-1, first identified as a pyrogen is a key mediator in the inflammatory response through mono- cyte activation. Interleukin-1 (IL-1) appears early in the immune response cascade and is the preferred in- dicator over interleukin-1because the latter is predom- inate in membrane and cell-associated process.7,8
In this study we have shown that persistent chronic prostatitis/chronic pelvic pain syndrome patients, in spite of the prolonged treatment, have elevated levels of the proinflammatory cytokines, IL-1in their prostate secretion. IL-1 levels in patients’ EPS were all sig- nificantly elevated than control group before treatment. Although the significance was not proved, their IL-1 levels were more elevated after treatment in group A (who still shows more than 10 WBCs/HPF in EPS) than pre- treatment or than control group.
Group B patients had less WBCs (<3/HPF) in EPS after treatment. However, patients with cleared clinical symptoms (group Br) had significantly lowered EPS IL-1 level. These results prove that immune reactions are responsible for the disease manifestation.
Treatment with antibiotics improves symptoms in 30% of men with chronic prostatitis/chronic pelvic pain syndrome, but the improvement occurswhether or not the men have bacterial organisms in EPSs.9,10 Even though the finding of leukocytes in EPSs has been interpreted as demonstrating that inflammation is
present in the prostate, there is significant overlap in the numbers of leukocytes when compared with asymptomatic men.11-13
There have been some evidences supporting chronic prostatitis/chronic pelvic pain syndrome is one clinical manifestation of autoimmune-associated inflammatory response.14-17
IL-1is the cytokine principally secreted by cells of the monocyte/macrophage lineage. The elevated cyto- kine levels we found in the persistently symptomatic subjects without bacterial growth suggest that there may be another pathophysiologic mechanism which results in the clinical manifestations.
The proinflammatory cytokines are also found in elevated levels in the joint fluid of rheumatoid arthritis patients and inhibition of the cytokine in rheumatoid arthritis patients has improved symptoms.18 Ponniash et al demonstrated that PSA was the self antigen for the autoimmune response in their study.19Several inves- tigators have provided evidence that prostate antigens can be recognized by T cells.20,21 T cell activation and participation of subsequent immune responses result in clinical symptoms. Therefore, in some patients, mem- brane stabilizing agents or anti-inflammatory agents give good clinical effects.20,21 Interleukin, complement and immunoglobulin in serum and ejaculates of chron- ic prostatitis/chronic pelvic pain syndrome revealed that there are some association of inflammatory proc- ess,4 They are also key factors associated with auto- immune reactions and
In this study, we found that the levels of IL-1in the prostate secretion of all subject patients were in- creased before treatment. Although overall IL-1level was significantly higher in each group when com- pared with control group at before and after treat- ment, group Br only showed significant pre- and post- treatment difference. IL-1β was elevated in subjects with significant WBCs in EPS with symptoms (group A) and subjects who still showed symptoms of chron- ic prostatitis/chronic pelvic pain syndrome even after
treatment (group Bp).
C3, C4, and IgG are also known to be related to immune reaction. Although data of our study was not evenly showing significant correlations in C4 and Ig G, C3 level showed significant correlation compared with control group. Group A is treatment non-res- ponder in EPS and its C3 level was higher at pre- and post-treatment period than control group. Group Bs are treatment responder in EPS and both sub- groups (Bp and Br) showed lower level of C3 than control group at pre- and post-treatment period.
These results suggest that clinical symptoms may be related with proinflammatory reactions which result from possible autoimmune reaction. This study has some limitations. Patient number is small and we on- ly measured only some part of various kinds of cytokines. Therefore, we cannot overly interpret our limited results. However, based on the result of this study, we can suggest that autoimmune reaction may be involved in developing chronic prostatitis/chronic pelvic pain syndrome.
Many reports are supporting that pathogenesis of chronic prostatitis/chornic pelvic pain syndrome is as- sociated with autoimmune reaction. The blocking of the effects of proinflammatory cytokines such as IL-1 β will diminish the symptoms, and this should be studied further with respect to proper treatment of the chronic prostatitis/chornic pelvic pain syndrome.
CONCLUSIONS
We evaluated the IL-1β, complements, and im- munoglobulin in prostate secretion in chronic prostati- tis/chronic pelvic pain syndrome. Our data reveals an inflammatory process even in subjects where no white cells were present in prostate secretion (category IIIB) with associated symptoms. Although more data and further studies should be followed, this suggests that chronic pelvic pain syndrome may be caused by an au- toimmune component and further treatment modalities
should be focused on the blocking of this reaction.
REFERENCES
1. Krieger JN, Nyberg LJ, Nickel JC. NIH consensus definition and classification of prostatitis. JAMA 1999;282:236-7
2. Hochreiter WW, Nadler RB, Koch AE, Campbell PL, Ludwig M, Weidner W, et al.Evaluation of the cytokines interleukin 8 and epithelial neutrophil acti- vating peptide 78 as indicators of inflammation in prostatic secretions. Urology 2000;56:1025-9
3. Tomaskovic I, Ruzic B, Trnski D, Kraus O. Chronic prostatitis/chronic pelvic pain syndrome in males may be an autoimmune disease, potentially re- sponsive to corticosteroid therapy. Med Hypotheses 2009;72:261-2
4. John H, Barghorn A, Funke G, Sulser T, Hailemariam S, Hauri D, et al. Noninflammatory chronic pelvic pain syndrome: immunological study in blood, ejacu- late and prostate tissue. Eur Urol 2001;39:72-8 5. Kohnen PW, Drach GW. Patterns of inflammation in
prostatic hyperplasia: a histologic and bacteriologic study. J Urol 1979121:755-60
6. Kramer G, Mitteregger D, Marberger M. Is benign prostatic hyperplasia (BPH) an immune inflammatory disease? Eur Urol 200751:1202-16
7. Hopp TP, Dower SK, March CJ. The molecular form of interleukin-1. Immunol Res 1986;5:271-80 8. Grassi J, Roberge CJ, Frobert Y, Pradelles P,
Poubelle PE. Determination of IL 1 alpha, IL 1 beta and IL2 in biological media using specific enzyme immunometric assays. Immunol Rev 1991;119:125-45 9. Murphy AB, Nadler RB. Pharmacotherapy strategies
in chronic prostatitis/chronic pelvic pain syndrome management. Expert Opin Pharmacother 2010;11:
1255-61
10. Nickel JC, Corcos J, Afridi S, Anderson P, Chetner M, Fradet Y, et al. Antibiotic therapy for chronic in- flammatory (NIH category II/IIIA) prostatitis (abstract). J Urol 1998;159 (suppl 5):272
11. Wiygul RD. Prostatitis: epidemiology of inflammation.
Curr Urol Rep 2005;6:282-9
12. Pontari MA, Ruggieri MR. Mechanisms in prostati- tis/chronic pelvic pain syndrome. J Urol 2004;172:
839-45
13. A Pontari M. Inflammation and anti-inflammatory therapy in chronic prostatitis. Urology 2002;60 (6 Suppl):29-33
14. Rivero VE, Motrich RD, Maccioni M, Riera CM.
Autoimmune etiology in chronic prostatitis syndrome:
an advance in the understanding of this pathology.
Crit Rev Immunol. 2007;27:33-46
15. Motrich RD, Maccioni M, Ponce AA, Gatti GA, Oberti JP, Rivero VE. Pathogenic consequences in semen quality of an autoimmune response against the prostate gland: from animal models to human disease. J Immunol 2006;177:957-67
16. Karlovsky ME, Pontari MA. Theories of prostatitis etiology. Curr Urol Rep. 2002;3:307-12
17. Shoskes DA, Albakri Q, Thomas K, Cook D.
Cytokine polymorphisms in men with chronic prosta- titis/chronic pelvic pain syndrome: association with diagnosis and treatment response. J Urol 2002;168:
331-5
18. Halloran MM, Woods JM, Strieter RM, Szekanecz Z, Volin MV, Hosaka S, et al. The role of an epithelial neutrophil-activating peptide-78-like protein in rat ad- juvant-induced arthritis. J Immunol 1999;162:7492-500 19. Ponniah S, Arah I, Alexander RB: PSA is a candi- date self-antigen in autoimmune chronic prostati- tis/chronic pelvic pain syndrome. Prostate 2000;44:
49-54
20. Bai J, Wang S, Liu J, Ye Z, Yu X, Xi Q, et al.
Characterization of circulating CD4+CD25high regu- latory T cells in men with chronic prostatitis/chronic pelvic pain syndrome. Urology 201075:938-42 21. Tomaskovic I, Ruzic B, Trnski D, Kraus O. Chronic
prostatitis/chronic pelvic pain syndrome in males may be an autoimmune disease, potentially re- sponsive to corticosteroid therapy. Med Hypotheses 2009;72:261-2