Case Report
원고 접수일 2012년 7월 26일, 원고 수정일 2012년 8월 17일, 게재 확정일 2012년 8월 27일
책임저자 권대근
(700-705) 대구시 중구 달구벌대로 2175, 경북대학교 치과병원 구강악안면외과 Tel: 053-600-7551, Fax: 053-426-5365, E-mail: [email protected]
RECEIVED July 26, 2012, REVISED August 17, 2012, ACCEPTED August 27, 2012
Correspondence to Tae-Geon Kwon
Department of Oral and Maxillofacial Surgery, School of Dentistry, Kyungpook National University
2175, Dalgubeol-daero, Jung-gu, Daegu 700-705, Korea
Tel: 82-53-600-7551, Fax: 82-53-426-5365, E-mail: [email protected]
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
측완 지방근막 피판과 악교정수술을 통한 반안면 위축증의 재건의 치험례: 증례보고
황희돈ㆍ최진욱ㆍ이성탁ㆍ이상한ㆍ권대근
경북대학교 치의학전문대학원 구강악안면외과학교실
Abstract
Reconstruction of Hemifacial Atrophy with Lateral Arm Adipofascial Flap and Orthognathic Surgery: A Case Report
Hee-Don Hwang, Jin-Wook Choi, Sung-Tak Lee, Sang-Han Lee, Tae-Geon Kwon Department of Oral and Maxillofacial Surgery, School of Dentistry, Kyungpook National University
Treatment of hemifacial atrophy is a challenge for oral & maxillofacial surgeons. The surgical approach basically focused on skeletal correction so that the overlying soft tissues can be improved by the osseous change of the skeleton. However, the treatment ends up with insufficient soft tissue mophology in most cases even after skeletal correction. Therefore comprehensive hard and soft tissue reconstruction is needed for treating the hemifacial atrophy. In this case report, we experienced a successful result after combined orthognathic and microvascular adipofascial flap reconstruction for hemifacial atrophy patient.
Key words: Facial hemiatrophy, Lateral arm free flap
서 론
반안면 위축증(hemifacial atrophy)은 1825년에 Parry[1], 1846년 Romberg[2]에 의해 처음 보고된 드문 질환이다. 안면의 편측으로 연조직뿐만 아니라 악골의 위축을 보이기 때문에 기능 적, 심미적으로뿐만 아니라 정신적으로도 환자에게 장애를 남기 는 질환이다. 일차적 원인으로 뇌의 지방대사 장애가 제시되고 있지만, 원인은 명확히 밝혀지지 않고 있다[3]. 이밖에 외상, 3차
신경 및 부교감신경의 손상, 목교감신경의 손상 및 압박, 두부 영양신경증, 내분비대사 장애, 감염에 따른 독혈증, 피부경화증 등이 관련이 있을 것으로 보고되고 있다[4]. 위축 과정은 악골의 성장이 완료된 후에 일어난다면 연조직에 국한되지만, 악골 성장 이 완료되지 않은 10대 이전에 일어난다면 대개 피부, 피하지방, 근육, 골 및 연골 등을 포함하는 얼굴 부위의 전체 구조물에 이환 하게 된다.
초기 증상으로 일부 연조직의 함몰을 보이는 작은 부위의 위축
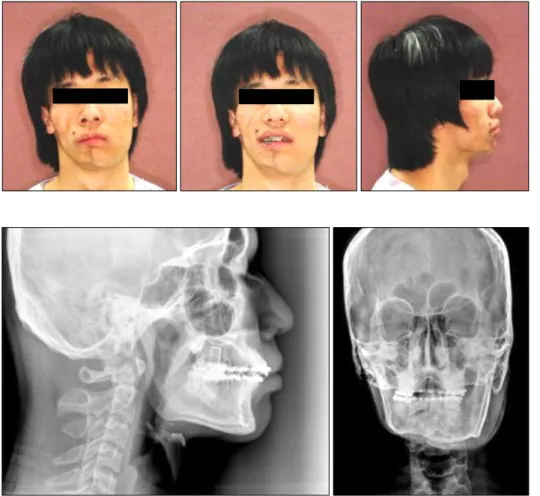
Fig. 1. Preoperative clinical photo-
graph. It shows right inferior border irregular appearance, rare hair, slight browny pigment and different skin texture.Fig. 2. Preoperative cephalometric
radiography.에서 시작하여 점차 다양한 비율, 다양한 거리로 안면 및 머리의 편측 전체로 퍼져나간다. 이는 종종 3차 신경의 주행경로를 따라 일어나기도 하여 신경학적 과정과 관련이 있을 것이라 추측한다.
얼굴 편측 피하조직의 명백한 위축은 진단의 가장 큰 특징이며 이러한 위축이 3차 신경의 3개의 주요 분지를 따라 일어나기도 함이 특징이다. 국소적 또는 점상 변색이 종종 뺨, 협골 융기, 입술 또는 이마에 나타나기도 하며, 'coup de sabre'가 특징적으 로 나타나기도 한다. 하지만 확진을 주는 명확한 혈액학적 소견은 없다.
반안면 위축증의 치료는 악안면재건외과의에게 당면한 과제 중 하나로, 일차적으로 외과적 접근을 기본적으로 하여 경조직교 정에 초점을 맞춘다. 이는 골격구조의 변화에 의해 연조직의 향상 을 기대하기 때문이다. 그러나, 결국 치료는 경조직교정 이후 대부분의 경우에 연조직 재건을 추가하게 된다. 재건 과정은 지방 이식, 진피 지방이식, 유경피판, 골이식, 유리피판, 지방근막이식 등이 주로 이용된다. 다음 단계로, posurs polyethylene im- plantation, liposuction debulking, fat injection, fat re- suspension과 같은 부가적인 술식이 필요할 수도 있다. 또한 좀 더 나은 결과를 위해 비이환된 부위에 부가적인 술식을 시행할 수도 있다.
본 증례에서는 골격적 교정 및 연조직 재건을 위해 악교정 수술과 측완 지방근막 피판술이 시행되었다. 이식된 피판의 지방 조직 흡수가 적었으며 측완 지방근막 피판술이 충분한 연조직을 제공함을 알 수 있었다. 본 증례에서 악교정 수술과 측완 지방근막 피판술을 사용하여 반안면 위축증의 치료를 시행 후 만족할 만한 결과를 얻었기에 보고하고자 한다.
증례보고
16세의 남자 환자가 반안면 위축증 치료를 위해 내원하였다.
환자는 우측 편측 얼굴의 위축과 더불어 2급 부정교합, 귀 주위와
측두부의 드문 머리 숱, 약한 갈색의 착색 및 좌우 피부 질감과
근육량의 차이를 보이며 하악 정중부에서 하악체까지 불규칙한
외형의 하악 하연을 보였다(Fig. 1). 코와 입술은 우측으로 변위되
었으며 하악정중부를 가로지르는 선상의 섬유성의 칼로 베낸 듯한
외형이 관찰되었다. 환자는 5세에 낙상에 의한 이부 부위의 외상
을 받은 적이 있으며 6세부터 우측 얼굴의 열성장이 나타남이
처음 인지되었다. 구강내 소견으로 상악 정중선이 우측으로 4.5
mm 변위되었으며 canting은 없었다. 하악 정중선은 우측으로
6 mm 변위를 보였다. 방사선 사진상으로 하악은 하악 정중부에
Fig. 3. Postoperative cephalometric
radiography after Lefort I osteotmy and sagittal split ramus osteotomy.Fig. 4. Operative photography: left
mandibular body osteotomy and fat dermal graft.Fig. 5. Postoperative photography
and x-ray after left mandibular body osteotomy and fat dermal graft.Positioned and fixed the cortical bone harvested by left mandibular body osteotomy on right man- dibular inferior border.
서 우측 하악체까지 불규칙한 외형의 하악 하연을 보였으며 우측 이 좌측에 비해 현저한 위축을 보였다(Fig. 2).
병력, 임상검사, 방사선 촬영을 통해 우측 반안면 위축증으로 진단하고, 술 전 계획으로 경조직 재건을 위해 상악은 Lefort I osteotomy를 통해 상악을 좌측으로 4.5 mm 이동, 하악은 부정교합 해결 및 하악골 저성장 재건을 위해 sagittal split ramus osteotomy 및 좌우 비대칭 개선을 위한 left mandibular body osteotomy를 계획하였고, 연조직 재건을 위해 fat dermal graft 를 계획하였다.
2008년 12월 8일 통상적인 방법으로 전신마취 후 저자 중의
한 명(Sang Han Lee)에 의하여 수술이 시행되었다. 상악은 통상 적인 Lefort I osteotmy를 통해 좌측으로 4.5 mm 이동을 통한 정중선 변위를 교정하였으며, 하악은 통상적인 sagittal split ra- mus osteotomy를 통해 하악을 3.5 mm 전방 이동 및 left로 6 mm 이동하여 부정교합을 해결하였다. 술 후 방사선 사진을 통해 술 후 골격적 교정 확인을 시행하여, 반안면 위축증의 골격적 교정을 완료하였다(Fig. 3).
2009년 12월 29일 연조직 재건을 위해 2차 수술을 시행하였다.
통상적인 방법으로 전신마취를 시행하였으며, 먼저 기존수술의
고정판 제거술을 시행 후 부가적 경조직교정을 위해 Left man-
Fig. 6. Operative photography on
reconstruction with lateral arm adi- pofascial flap.Fig. 7. Postoperative photography
after reconstruction with lateral arm adipofascial flap.dibular body osteotomy를 시행하였다. 이후 연조직 교정을 위해 fat dermal graft를 시행하였다(Fig. 4). 수술 직후 좌우 비대칭이 해소되어 만족할 만한 결과를 보여주었으나(Fig. 5) 추적 관찰 과정에서 fat dermal graft의 흡수가 관찰되었다. 이에 2010년 7월 13일 측완 지방근막 피판술을 이용한 연조직 재건을 시행하였다. 먼저 통상적인 방법으로 전신마취를 시행 후 본 증례 에서는 우측의 결손부위보다 약 120% 큰 부피로 측완에서 지방근 막 피판 7×10 cm를 안면 혈관에 문합하였다. 피판의 표면은 탈상피화하였으며 결손부위에 이식 전에 모든 트리밍을 시행하였 다. 공여부는 일차 봉합을 시행하였다. 결손부위의 수혜부는 악하
절개를 통해 박리하였고, 피하조직과 근육층 사이로 박리를 시행 하여 피판을 삽입하였다. 피판은 근육층 상방에 위치시킨 후에 근막 및 골막에 봉합 및 고정을 시행하였다(Fig. 6). 이때 박리 및 피판의 삽입은 이하선 근막의 상방에서 주의 깊게 시행되어 안면신경의 노출 및 손상 없이 수술이 진행됨으로써 술 후 안면신 경의 손상에 의한 둔화는 관찰되지 않았다. 수술 직후 만족스러운 외형을 보였으며, 공여부의 병적인 소견 또한 거의 없었다(Fig.
7). 추적관찰 중 술 후 중력에 의한 연조직의 처짐 현상이 발생하
여(Fig. 8), 2011년 1월 28일 debulking을 시행하였다. 부가적
수술 이후 만족할 만한 결과를 보였으며, 술 후 14개월간의 추적관
Fig. 8. Follow-up photography after reconstruction with lateral
arm adipofascial flap. We guess that the displacement was caused to gravity and the resorption was minimized.찰 동안 피판의 흡수 없이 양호한 결과를 보이고 있다.
고 찰
중안모를 포함한 치열안면부위는 말, 저작, 연하 및 호흡과 같은 기능뿐만 아니라 사람의 개성을 나타내는 중요한 구조물이 다. 반안면 위축증은 이처럼 중요한 얼굴 및 안면부에 편측으로 연조직 및 악골의 위축을 보이며 안면부의 비대칭을 야기하는 질환이다. Gorlin 등[5]은 반안면 위축의 발병률이 5,600명에 한 명 꼴로 나타난다고 보고하였다. 이는 골격의 비대칭에 의한 하악골의 변위가 나타나면서 상악골 및 중안면부의 이차적인 기형 을 유발할 수 있다고 한다[6,7]. 이로 인해 반안면 위축증은 기능 적, 심미적, 정신적 손상을 줄 수 있다. 특히, 성장기의 아이들에게 는 악골의 발육 및 자아의 형성에도 영향을 미치게 된다. 그래서 반안면 위축증의 환자에게서 재건의 목적은 이러한 기능적, 심미 적 결손을 최소화하는 데 있다.
치료는 연조직 재건을 위해 위축에 의해 결손된 부위에 지방조 직을 위치시키는데 대개 기초를 둔다[8]. Eitner[9]는 free dermal fat grafting을, Ashley 등[10]은 medical silicone injection을 처음 보고한 이후 simple/composte grafts (dermal and der- mal-fat grafts), autologous tissues/lipofilling의 주입, paraf- fin, silicone, polyalkylimide gel/poly-L-lactic acid 등이 반안 면 왜소증의 심미적 교정에 사용될 수 있음이 보고되었다[8,11].
하지만 이러한 것들은 일시적으로 좋은 외형을 줄 수 있지만 시간이 지속되면서 흡수되어 오랜 시간 지속되지는 않는 것으로 보인다. Schuessler와 Steffanoff[12]는 free dermal fat grafting 이 술 후 약 15%의 흡수, 15%의 감염, 낭종 형성 5%가 발생할
수 있음을 보고하였다.
게다가 위축 과정은 단순히 지방조직뿐만 아니라 대개 피부, 피하지방, 근육, 골 및 연골에 관련되므로 이러한 구조물의 3차원 적 재건이 필요하다. 그래서 Fujino 등[13]이 1974년에 처음 골 결손 부위의 재건을 위한 craniofacial surgical approach와 연조 직 결손 부위의 재건을 위한 microvascular surgical approach 를 함께 시행한 이후로 현재의 재건 과정에서는 경조직 재건과 함께 microvascular flap이 가장 적절한 치료 방법으로 제시되고 있다. Omentum, rectus abdominis, groin, radial forearm, deep inferior epigastric perforator, anterolateral thigh, par- ascapular flap 등의 다양한 피판이 치료를 위해 시행되어 보고되 어 왔다[14-19]. 하지만 이러한 여러 microvascular flap은 각각 의 장단점으로 인해 아직까지 여러 시도들이 이어져 오고 있다.
많은 microvascular flap 중에 측완 지방근막 피판술은 안면부 위의 큰 결손의 재건에 유용하다. 측완 지방근막 피판술은 다양한 두께의 연조직으로 많은 양의 연조직을 공여할 수 있다. Renato 등은 길이 외측 상완 피판술은 길이가 9∼20 cm, 폭 3∼8 cm까 지 다양하게 채취할 수 있었다고 보고하였다[20]. 또한 채취된 피판은 다양한 두께로 이용 가능하며 얇고, 유동적이며, 높은 신뢰성, 최소한의 흡수율, 안전하고 쉬운 접근성, long pedicle, 혈관혈류 이상이 없고, 공여부의 최소한의 결손만을 가져 안면부 의 재건에 유용하다. 이처럼 측완 지방근막 피판술은 많은 장점을 가지지만 간혹 의미 있게 중력 방향으로의 처짐 현상이 보인다.
이를 방지하기 위해 경조직에 여러 지점에서의 봉합을 통해 위치 의 안정을 줄 수 있으나 한계가 있다. 그래서 liposuction이나 debulking이 필요할 수도 있다. 본 증례에서도 중력에 의한 쳐짐 현상과 함께 이식 조직의 흡수량이 예상보다 적어 debulking을 통해 부가적인 교정을 시행하여 만족할 만한 결과를 나타내었다.
본 교실에서는 측완 지방근막 피판술과 악교정 수술을 통해 반안면 위축증을 재건하였다. 현재까지 측완 지방근막 피판술을 통하여 반안면 위축증의 치료를 시행한 증례는 보고되지 않았지 만, 우리의 증례에서 측완 지방근막 피판술은 안전하게 하안면 및 중안면의 재건에 사용되었고, 안면신경의 노출을 피함을 통해 안면 표정근에 부작용을 미치지 않으면서 피판이 안정적으로 잘 유지되었을 뿐만 아니라 안면 결손부의 재건에 충족하는 두께, 질감을 가지며 공여부의 최소한의 병적상태만을 야기하며 술 후 장기 관찰 시 좋은 결과를 보였다. 특히 다른 국소 피판이 약 20% 이상의 술 후 흡수를 보이는 것과는 달리 측완 지방근막 피판은 거의 흡수를 보이지 않아 술 후 큰 안정성을 보였다.
그러나 측완 지방근막 피판술 시행 후 6개월 이내에 대부분의
흡수가 진행되므로, 6개월 후 liposuction debulking과 같은
피판의 부가적인 술식 필요성의 가능성이 일련의 수정 과정에서
필요하였다. 하지만 이러한 모든 과정을 시행하였을 시 환자는
좌우 대칭성과 외형에서 심미적으로 만족하였다.
본 교실에서는 이러한 증례를 통해 외측 상완 지방근막 피판술 과 악교정 수술이 반안면 왜소증의 좋은 치료 방법이 될 수 있음을 알 수 있었다.
References