단 신
ISSN 2093-9272 일산병원학술지 2017;16(2):233-236Volume 16 Number 2 December 2017
233
Clostridium difficile 감염의 진단을 위한 글루탐산탈수소효소 효소면역분석법의 유효성에 대한 체계적인 문헌 고찰
국민건강보험 일산병원 진단검사의학과
김영아, 이상선, 손영준
Systemic Review on the Effectiveness of Diagnosis of Clostridium difficile Infection Using Glutamate Dehydrogenase Enzyme-Immunoassay
Young Ah Kim, Sang Sun Lee, Young Jun Son
Department of Laboratory Medicine, National Health Insurance Service Ilsan Hospital, Goyang Korea
Glutamate dehydrogenase (GDH) enzyme-linked immunosorbent assay (ELISA)/enzyme-linked fluorescent assay (ELFA) was recently introduced for the detection of Clostridium difficile infection. The effectiveness of this method was systemically reviewed before decision making of introduction of new method. In conclusion, GDH ELISA / ELFA is useful tests for diarrhea patient, sus- pected of C. difficile infection.
Key Words: Clostridium difficile infection, Glutamate dehydrogenase, Enzyme-linked immunosorbent assay, Enzyme-linked fluorescent assay
책임저자: 김영아
10444 경기도 고양시 일산동구 일산로 100 국민건강보험 일산병원 진단검사의학과 전화 : (031)900-0908 팩스 : (031)900-0912 E-mail : [email protected],kr
서 론
Clostridium difficile
infection (이하 CDI)는 입원한 환자에 서 발생하는 설사의 가장 중요한 원인으로 항생제-연관 설사 (antibiotic-associated diarrhea)의 15-25%를 차지하며, 항생 제 사용 후 발생한 위막성 대장염(pseudomembranous colitis) 의 경우는 95-100%가 CDI 인 것으로 알려져 있다.1 CDI의 주요 위험인자는 연령, 입원 및 항생제 사용으로 연령이 높을 수록 CDI 발생률이 증가하는 것으로 보고되고 있고, cefotaxime, ceftazidime, amoxicillin, amoxicillin-clavulanic acid, antipseu- domonal penicillin, quinolone 및 aminoglycoside 등 대부분의 항생제가 연관되는 것으로 알려져 있으며, 여러 항생제를 동 시에 투여하면 단일 항생제를 사용할 때 보다 의미 있게 CDI 발생이 증가하는 것으로 보고되고 있다.1C. difficile
연관설사의 진단을 위해서는 설사나 묽은 변(24 시간 이내 3회 이상)에서 독소 생성C. difficile
이 있음을 확인 하여야 한다[2]. 기존의C. difficile
과 독소를 검출하는 검사법 을 살펴보면 표준방법인 세포독성검사법(cytotoxic assay)은 세포를 배양하여 독소B의 세포병변효과(cytopathic effect)를 확인하는 것으로 세포배양이 필요하고 검사시간이 오래 걸리 므로 통상적으로 적용하기에는 무리가 있다.3C. difficile
배양 은 민감도가 우수하지만, 검사 소요시간이 48시간 이상 걸리 고, 보균자와 독소를 생성하지 않는 균주도 배양되므로 특이 도가 낮은 단점이 있다.3 변 검체에서 직접 중합효소연쇄반응 (PCR)으로 독소 A 및 B 유전자를 검출하는 방법은 민감도가 높고 검사시간이 배양에 비해 짧은 장점이 있으나, 죽은 세포 에 의한 위양성과 변 검체 내에 존재하는 PCR 저해인자에 의한 위음성 가능성이 있다.3 변 검체에서 직접 효소면역분석 법(enzyme immunoassay, EIA)으로 독소 A 및 B를 검출하는 방 법도 자동화된 장비를 이용하여 쉽게할 수 있으므로 많은 검사 실에서 실시하고 있지만, 배양에 비해 검사시간이 짧고 특이도 는 좋으나, 민감도가 충분하지 않은 것으로 단점이 있다.3글루탐산탈수소효소(Glutamate dehydrogenase, GDH)를 샌드위치 기반의 단일클론항체를 사용한 효소결합면역흡착
YA Kim, et al. Effectiveness of Diagnosis of C. difficile Infection Using GDH ELISA
234
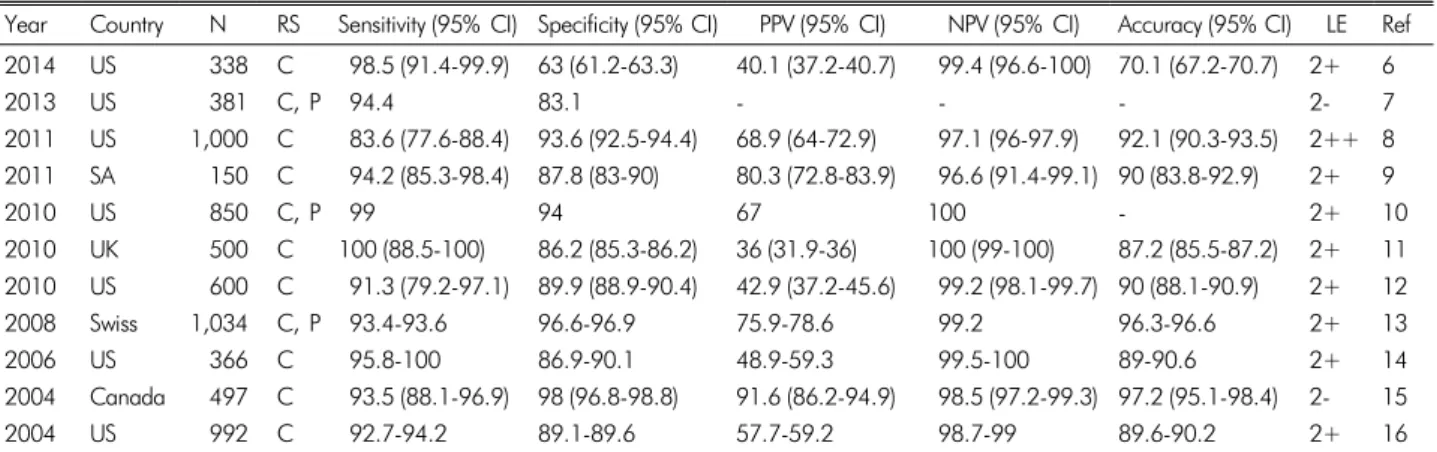
Korean Journal of National Health Insurance Service Ilsan HospitalTable 1. The effectiveness of GDH ELISA on the basis of cytotoxin assay and/or real time-PCR/PCR for C. difficile toxin as reference standard
Year Country N RS Sensitivity (95% CI) Specificity (95% CI) PPV (95% CI) NPV (95% CI) Accuracy (95% CI) LE Ref 2014 US 338 C 98.5 (91.4-99.9) 63 (61.2-63.3) 40.1 (37.2-40.7) 99.4 (96.6-100) 70.1 (67.2-70.7) 2+ 6
2013 US 381 C, P 94.4 83.1 - - - 2- 7
2011 US 1,000 C 83.6 (77.6-88.4) 93.6 (92.5-94.4) 68.9 (64-72.9) 97.1 (96-97.9) 92.1 (90.3-93.5) 2++ 8 2011 SA 150 C 94.2 (85.3-98.4) 87.8 (83-90) 80.3 (72.8-83.9) 96.6 (91.4-99.1) 90 (83.8-92.9) 2+ 9
2010 US 850 C, P 99 94 67 100 - 2+ 10
2010 UK 500 C 100 (88.5-100) 86.2 (85.3-86.2) 36 (31.9-36) 100 (99-100) 87.2 (85.5-87.2) 2+ 11 2010 US 600 C 91.3 (79.2-97.1) 89.9 (88.9-90.4) 42.9 (37.2-45.6) 99.2 (98.1-99.7) 90 (88.1-90.9) 2+ 12
2008 Swiss 1,034 C, P 93.4-93.6 96.6-96.9 75.9-78.6 99.2 96.3-96.6 2+ 13
2006 US 366 C 95.8-100 86.9-90.1 48.9-59.3 99.5-100 89-90.6 2+ 14
2004 Canada 497 C 93.5 (88.1-96.9) 98 (96.8-98.8) 91.6 (86.2-94.9) 98.5 (97.2-99.3) 97.2 (95.1-98.4) 2- 15
2004 US 992 C 92.7-94.2 89.1-89.6 57.7-59.2 98.7-99 89.6-90.2 2+ 16
N, number of stool sample; RS, reference standard; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; LE, level of evidence; Ref, reference; US, united states of America; SA, Saudi Arabia; UK, united kingdom; C, cytotoxin assay; P, real time-PCR or PCR for C. difficile toxin
측정법(enzyme-linked immunosorbent assay, ELISA)와 효소 면역 샌드위치 분석법과 최종형광검출을 결합하여 민감도를 향상시킨 효소결합형광분석법(enzyme-linked fluorescent assay, ELFA)은
C. difficile
균에 대한 GDH 항원을 정성적으로 검출 하기 위한 자동화 장비를 이용하는 검사로 GDH는 세포벽에 흔히 존재하며,C. difficile
검출에 민감한 지표이지만, 독소 생성에 상관없이 검출되므로 비특이적 시험이다.3C. difficile
감염은 북미와 유럽에서 고병원성 균이 유행하 면서 과거와는 다른 역학을 보이고 있으며, 국내 발생 빈도와 심각성이 증가하면서,1 신속하고 정확한 독소생성C. difficile
감염의 진단법의 확립과 진단 알고리즘을 확립할 필요성이 대두되었다. GDH 검사는 국외에서는 선별검사로 우수성이 인정받고 있지만,4 국내에서는 아직 이에 대한 협의가 부족한 실정이므로 본 연구에서 체계적 문헌고찰 방법을 통하여 GDH ELISA와 ELFA 검사의 유효성을 평가하고, CDI 검사 알고리 즘의 재설정을 검토해 보았다.GDH ELISA와 ELFA 검사의 유효성
GDH ELISA의 진단 정확성은 선택문헌의 질 평가5 기준에 따라 선택한 총 11편의 문헌6-16을 근거로 민감도(sensitivity), 특이도(specificity), 양성예측도(positive predictive value), 음 성예측도(negative predictive value) 및 검사 정확도(accuracy of index test)를 평가하였다. 참고기준(reference standard)은 세포독성 검사(cytotoxin assay) 그리고/또는
C. difficile
독소 유전자 RT-PCR/PCR로 하였으며(Table 1), 종합하면 GDH ELISA는 민감도 83.6-100%, 특이도 63-100%이었다. 문헌분석한 논문 중 8편6,8,9,10,12,14-16
에서는 비교 검사의 진단 정확 성을 동일한 참고 기준으로 평가하였는데(Table 2), 종합하면 민감도 37.5-100%, 특이도 82.7-100%이었다.
GDH ELFA의 진단 정확성은 CDI이 의심되는 환자의 대변 검체 1,034개를 대상으로 세포독성 검사를 참고기준으로 평 가된 한편의 논문이 있었는데,17 여기에서 보고된 민감도 93-95%와 특이도 90-91.8% 및 검사정확도는 91-92%이었 다. 같은 연구에서
C. difficile
PCR 독소 유전자 검사의 진단 정확성을 평가한 결과 세포독성 검사를 참고기준으로 민감도 71.2% 및 특이도 89.4%를 보였다.17Landry 등의 연구에서 세포독성 검사, GDH ELISA,
C. diffi- cile
PCR 독소 유전자 검사의 검사 결과 보고시간(turnaround time, TAT)를 비교하였는데, 세포독성 검사의 경우 6-48시간 이 소요되는 것에 비하여 GDH ELISA와C. difficile
PCR 독소 유전자 검사는 모두 2-24시간이 소요되어 비교적 짧은 시간 안에 검사 결과를 확인할 수 있었다.6CDI 감염의 진단 알고리즘의 재설정
CDI 감염이 의심되는 환자의 진단을 검사법은 각각의 장 단점이 있기 때문에 국외에서는 진단을 위한 가이드라인에 대해 많은 연구가 있다.4,18,19 미국미생물학회의 권고사항을 살펴보면 GDH 항원 검사는 많은 연구에서 높은 민감도와 음성예측도를 보이므로 CDI의 우수한 선별검사이며, GDH 양성 결과가 EIA
C. difficile
독소 검사(toxin A/B) 양성, 세포 독소 중화시험(cytotoxin neutralization assay) 양성 또는 핵산 증폭시험(nucleic acid amplification test, NAAT) 양성과 함께김영아 외. GDH ELISA/ELFA 유효성
Volume 16 Number 2 December 2017
235
Table 2. The effectiveness of C. difficile culture, enzyme-immunoassay for C. difficile toxin, real time PCR/PCR for C. difficile toxin gene on the basis of cytotoxin assay and/or real time-PCR/PCR for C. difficile toxin as reference standard.Year N Cp RS Sensitivity (95% CI) Specificity (95% CI) PPV (95% CI) NPV (95% CI) Accuracy (95% CI) LE Ref 2014 338 P C 95.6 (88.1-98.8) 92.2 (90.3-93) 75.6 (69.7-78.1) 98.8 (96.8-99.7) 92.9 (89.9-94.2) 2+ 6
2011 1,000 E C 39.7-94.5 96.5-99.8 82.1-97.1 90.5-99 - 2++ 8
2011 150 E C 73.1 (65-73) 100 (96-100) 100 (90-100) 87.5 (84.1-87.5) 90.7 (85.7-90.7) 2+ 9
2010 850 E C, P 73 98 86 97 - 2+ 10
2010 600 E C 60.9-100 82.7-99.3 32.4-87.5 96.8-100 84-96.3 2+ 12
2006 366 E C 37.5 (20.3-37.5) 100 (96.7-100) 100 (54.3-100) 89.4 (86.4-89.4) 90 (84.5-90) 2+ 14
2004 497 E C 84.9 98.8 94.0 96.6 96.2 2- 15
2004 992 P, Ct C 63.5-92.7 89.7-90.5 51.8-59.1 93.9-98.7 86.8-90.1 2+ 16
N, number of stool sample; Cp, comparator such as C. difficile culture, enzyme-immunoassay (EIA) for C. difficile toxin, real time PCR/PCR for C.
difficile toxin gene; RS, reference standard; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; LE, level of evidence;
Ref, reference; E, EIA for C. difficile toxin; C, cytotoxin assay; P, real time-PCR or PCR for C. difficile toxin; Ct, C. difficile culture
보고될 경우 toxigenic
C. difficile
양성으로 보고하며, GDH 양성의 경우 다른 추가 검사들을 통해 반드시 결과가 확인되 어야 하므로 만약 EIAC. difficile
독소 검사 또는 세포독소 중화시험 음성일 경우, 검체는 핵산증폭시험이나 toxigenicC. difficile
배양 중 한가지 검사를 시행해야 한다고 제안하고 있다.4Agency for Healthcare Research and Quality에서도 GDH 선별검사는 독소 A/B 검출을 위한 EIA법과 함께 2단계 또는 3단계 스크리닝 알고리즘을 따라 시행할 것을 강력히 권고하 고 있으며,18 Society for Healthcare Epidemiology of America (SHEA) 및 Infectious Disease Society of America (IDSA)에서 도 독소 검사는 임상적으로 가장 중요하나, 민감도가 부족하다 는 것이 걸림돌이므로 이러한 문제를 해결하기 위한 가능한 전략은 EIA법을 이용한 GDH 검출을 초기 스크리닝 검사로 사용하고, 양성이 나온 검체에 한해 세포독성 시험 또는 toxige- nic
C. difficile
배양을 확진 검사로 사용하는 2단계 알고리즘 을 권고하고 있다.19국내에서도 CDI 진단 알고리즘을 확립할 필요성이 있는 데, 핵산증폭시험을 단독으로 이용하는 경우 가장 민감하고 특이적이나 검사비용이 비싼 단점이 있으므로 GDH 검사를 이용하여 선별 후 확인하는 2혹은 3단계 알고리즘을 고려할 필요가 있겠다.
체계적 문헌고찰 방법을 통하여 GDH ELISA 검사의 유효성 을 검토해 본 결과 기존에 사용하고 있는 비교 검사들에 비하여 진단 정확성이 동등 이상으로 확인되고 있고, GDH 검출이 CDI 진단에 임상적 의의가 있음이 이미 입증되어 있어,3,4,18,19 임상적 유효성이 있는 검사로 판단되었다. GDH ELFA 검사 도 형광신호(flurescent signal)을 검출 하는 검사로 ELISA보다
민감도가 높은 검사 방법으로 알려져 있고, 비교 검사보다 진단 정확성이 높은 것으로 보고되어 있으므로,17 임상적 유효성이 있는 검사로 판단되었다. 따라서 본원에서도 GDH 검사를 이 용하여 선별 후
C. difficile
배양과 핵산증폭시험을 통해 확인하 는 2 혹은 3단계 알고리즘을 도입할 필요가 있겠다.REFERENCES
1. 배현주. Clostridium difficile 감염의 역학 및 치료. 감염과 화 학요법 2010;42:362-8.
2. !Dubberke ER, Carling P, Carrico R, et al. Strategies to prevent Clostridium difficile infections in acute care hospitals: 2014 Update. Infect Control Hosp Epidemiol. 2014;35:628-45.
3. 대한진단검사의학회. 진단검사의학. 범문에듀케이션 2014.
4. Agency for Healthcare Research and Quality (AHRQ). Guide- lines for diagnosis, treatment, and prevention of Clostridium difficile infections. 2010. Available from URL: http://www.gui deline. gov (last visited 4th October, 2017).
5. Jeong J, Lee S, Jang S. A systematic review on the effectiveness of detection of M. tuberculosis and rifampin resistance using Xpert MTB/RIF. Ann Clin Microbiol 2014;17:42-9.
6. Landry ML, Ferguson D, Topal J. Comparison of Simplexa universal direct PCR with cytotoxicity assay for diagnosis of Clostridium difficile infection: performance, cost, and correla tionwith disease. J Clin Microbiol 2014;52:275-80.
7. Miller S, Wiita A, Wright C, Reyes H, Liu C. Evaluation of glutamate dehydrogenase immunoassay screening with toxin confirmation for the diagnosis of Clostridium difficile infe- ction. Lab Med. 2013;44:e65-e71.
8. Peterson LR, Mehta MS, Patel PA, et al. Laboratory testing for Clostridium difficile infection: light at the end of the tun- nel. Am J Clin Pathol 2011;136:372-80.
9. Qutub MO, AlBaz N, Hawken P, et al. Comparison between the two-step and the three-step algorithms for the detection of toxigenic Clostridium difficile. Indian J Med Microbiol. 2011;
YA Kim, et al. Effectiveness of Diagnosis of C. difficile Infection Using GDH ELISA
236
Korean Journal of National Health Insurance Service Ilsan Hospital 29:293-6.10. Doing KM, Hintz MS, Keefe C, et al. Reevaluation of the pre- mier Clostridium difficile toxin A and B immunoassay with comparison to glutamate dehydrogenase common antigen tes- ting evaluating Bartels cytotoxin and Prodesse ProGastro Cd polymerase chain reaction as confirmatory procedures. Diag Microbiol Infect Dis 2010;66:129-34.
11. Goldenberg SD, Cliff PR, Smith S, et al. Two-step glutamate dehydrogenase antigen real-time polymerase chain reaction assay for detection of toxigenic Clostridium difficile. J Hosp Infect 2010;74:48-54.
12. Reller ME, Alcabasa RC, Lema CA, et al. Comparison of two rapid assays for Clostridium difficile common antigen and a C difficile toxin A/B assay with the cell culture neutralization assay.
Am J Clin Pathol 2010;133:107-9.
13. Fenner L, Widmer AF, Goy G, et al. Rapid and reliable diag- nostic algorithm for detection of Clostridium difficile. J Clin Microbiol 2008;46:328-30.
14. Ticehurst JR, Aird DZ, Dam LM, et al. Effective detection of toxigenic Clostridium difficile by a two-step algorithm including tests for antigen and cytotoxin. J Clin Microbiol 2006;44:1145-9.
15. Snell H, Ramos M, Longo S, et al. Performance of the TechLab
C. DIFF CHEK-60 enzyme immunoassay (EIA) in combination with the C. difficile Tox A/B II EIA kit, the Triage C. difficile panel immunoassay, and cytotoxin assay for diagnosis of Clostridium difficile-associated diarrhea. J Clin Microbiol 2004;42:4863-5.
16. Zheng L, Keller SF, Lyerly DM, et al. Multicenter evaluation of a new screening test that detects Clostridium difficile in fecal specimens. J Clin Microbiol 2004;42:3837-40.
17. Davies KA, doing CE, Morris KA, et al. Comparison of the Vidas C. difficile GDH automated enzyme-linked fluorescence immunoassay (ELFA) with another commercial enzyme immu- noassay (EIA) (Quik Chek-60), two selective media, and a PCR assay for gluD for detection of Clostridium difficile in fecal samples. J Clin Microbiol 2015;53:1931-4.
18. Agency for Healthcare Research and Quality (AHRQ). Guide- lines for diagnosis, treatment, and prevention of Clostridium difficile infections. 2010. Available from URL: http://www.gui deline.gov (last visited 4th October, 2017).
19. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA).
Infect Contr Hosp Epidemiol 2010;31:431-55.