J、~:',' )l{ ~‘t 원 쩍 JJ~ 1깐 Jt‘ ~;23 ;하 갖; 2 싸 pp. 302 - 308, 1987 Journal 01 Korean Radiological Society , 23(2) 302-308 1987
Digital Flexor Tendons of the Hand:
N ormal Ultrasonographic Anatomy*
Young Goo .Kim, M.D., Jong Beum Lee, M.D., Yong Chul Lee, M,D., Kwan Seh Lee, M.D.
《국문 초록》
Deþartmeη t of Radiology, College of Medicine, Chung Ang U:ηiversity
手指屆廳의 正常 超音波握影所見*
中央大學校 醫科大學 放射線科學數室 金榮九·李鍾範·李容哲·李寬世
표常 自願者 5 名에서 手指屆뾰의 高解像 超줍波檢흉블 실시하여 그 正常 超를波解흠O所見을 고찰 하였다.
超즙波檢훌는 10 MHz 트랜스듀서 를 사용하여 手根터 널 · 中手骨 • 手指部 等의 부위 로 나누어 橫 斷 및 做斷銀影을 하였다 또한 리얼타임影像을 통하여 각 手指關節의 屆{申i필動時 각 屆健의 i重動 을 관찰하였다. 超륨波췄훌影에 의하여 각 부위에서의 手指屆健 및 주변조직을 판찰할 수 있었고 그 所見을 기술하였다.
手指屆魔의 正常 超룹波解픔U의 이해는 手指屆 l健 및 주연조직의 超를波양斷에 유용할 것으로 생각 된다.
Superficially located tendons 01 the body can be easily assessed by ultrasonography with high Irequency, short locused transducer. But, there has been no reports 01 detailed anatomic studies 01 digital Ilexor tendons
。1the hand by using ultrasonography. Thus, we performed the ultrasonogrphy 01 the hands 01 normal volunteers, and report normal ultrasonographic lindings
Images were obtained in axial and longitudinal planes Irom the wrist to the insertion site 01 each tendon In addition, the movement 01 the tendon was observed at rest, and during Ilexion and extension 01 each lihger The ultrasonographic sectional anatomy 01 Ilexor tendons and their neighbouring structures were sucesslul Iy demonstrated, and the understanding 01 it will provide a uselul background knowledge lor the diagnosis
。1 pathologic conditions
* 본 논문응 1985 년도 중앙대학교 의파대학 부속병원 및 주식회사 종근당의 연구조성비로 이루어진 것임 Received January 21, accepted March 18, 1987
- Young Goo Kim, et al.: Digital Flexor Tendons of the Hand
Digital flexor tendons of the hand, which are so superficially located in palmar aspect of the hand and wrist, can be easily assessed by high-resolution ultrasonography with high frequency, short focused transducer.
Ultrasonography of the tendons was reported in certain areas óf the body, but there are few reports of detailed sonographic anatomic study of the digital flexor tendons of the hand in the literature, 1-4) We performed ultrasono- graphy of the digital flexor tendons of normal hands, and report the normal ultrasonographic sectional anatomic findings.
ANATOMY
There are nine digital flexor tendons in each hand: one thumb flexor, the flexor pollicis longus(FPL), and eight finger flexors, the flex- or digitorum superficialis(FDS) and the flex- or digitorum profundus(FDP). In palmar aspect of the wrist, they pass through the nar- row osseofibrous tunnel, called the carpal canal, with the median nerve. The carpal canal is confined by flexor retinaculum ventrally and carpal bones dorsally. Over the metacarpals, the FDS and FDP tendons diverge and spread out from the carpal canal toward the fingers, and the FDP tendons give origin to four lum- brical muscles. The FPL tendon runs along the medial border of thenar muscles buried between the two heads of the flexor pollicis brevis muscles. At the level of metacarpo- phalangeal joint, they enter the narrow digital canals. Approximately over the middle of the proximal phalanx, the FDS tendons split into two halves, and are perforated by the FDP tendons. The half of the each half decussate around the FDP tendon, and non-decussating the other half of each half continue on the same side of the FDP tendon. Then they reunite behind the FDP tendon as they be- come inserted on the border of the middle phalanx. The FDP tendon has a broad inser- tion site on the base of the distal phalanx. On
the other hand, the FPL tendon passes bet- ween the two sesamoids of th,e thumb, and is inserted into the distal phalanx of the thumb.5)
SUBJECTS and METHODS Ten hands of 5 healthy volunteers were ex- amined by ultrasonography. A linear mechani- cal sector scanner (Picker, Microview) with a 10 Mhz, 5.7cm focus transducer was used.
The transducer is housed within a water path, and is capable of imaging a 3cm x 4cm field at 15 frames per second. The subjects were placed in sitting position with their hands supinated on the scanning table. Images were obtained in axial and longitudinal planes from the wrist to the insertion site of the tendon.
In axial sections, next levels were specified and analyzed in detail: proximal and distal car- pal canal, proximal and distal metacarpal, and the digital canal. The longtudinal sections were performed along the course of each ten- don. The movement of the tendon was also
obseπed at rest, and during flexion and exten sion of each finger. In addition, the specific tendon movement was attempted to assess during the test of strength of the specific mus- cle. For example, for the FDP3 tendon, which is the flexor of distal phalanx of the midle finger, the observation of it was done during flexion of distal phalanx of the middle finger against the resistance with the proximal and middle phalanx stabilized in extension.
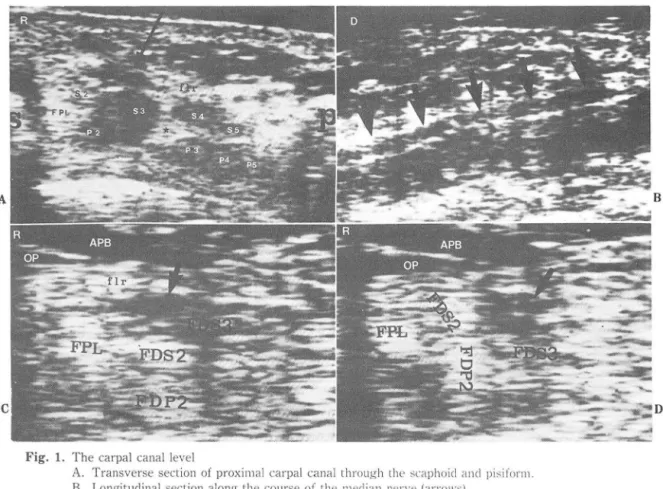
RESULTS (1) The Carpal Canal (Fig. 1)
In transverse section, the elliptically shaped carpal canal, confined by flexor retinaculum and the carpal bones, contains 9 digital flexor tendons and the median nerve. The median nerve is eccentrically located in radial, super- ficial protion of the canal, and has an echogen- city lower than the tendons with flattened ovoid shape. The flexor tendons are depicted - 303-
A
The Journal of the Korean Radiological Society, Vol. 23, No. 2, 1987 -
as ovid or round hyperechoic densities, close- ly packed within the canal. The tendons so closely lie that it is somewhat difficult to delineate them clearly on ultrasonography.
But they have relatively constant relationships between themselves within the canal: the ulnar half of the canal is occupied by the FDS 4 and 5 tendons in superficial portion, and the FDP 3,4 and 5 tendons in deep portion. The radial half is occupied by the FPL tendon in the most radial side, the median nerve most superficially, the FDS 3 tendon lying just infero-ulnar side of the median nerve, and the FDS 2 and FDP 2 tendon lying deep to the me- dian nerve (Fig. la).
The median nerve is also delineated in longitudinal section as a hypoechoic tubular density which runs over the flexor tendon groups (Fig. lb). The elevation and rotation of the tendon occurs during the contraction of it, and brings about subtle changes of its shape and location in transverse section of carpal canal. For example, during the isolated con- traction of FDP 2, which is obtained by flex- ion of distal phalanx of the index finger against the resistance with the proximal and distal phalanx stabilized, clockwise rotation and slight elevation of the FDP 2 tendon could be observed on realtime image. At the same time, the FDS 2 is also elevated and rotated by the
C
Fig. 1. The carpal canal level
A. Transverse section of proxima! carpal canal through the ,;caphoicl ancl pisifol"lll B. Longituclinal section along the course of the llledian nen'c (arro\\"s)
C. D. Transverse section of the distal carpal canal (x 2. lllagnification) L'. \\'ith all c1igit:; extendecl d. Only FDP2 contracted. s 2,3,4,5 = FDP tenclon 2,:3,4.5, ]l 2.3,4,5 = FDP tcnclon 2.3 . ..J .;)‘ :; = scaphoicl ‘ arrow = median nerve; * = peritenclinous fat, f1r = f1exor retinaculuJl1‘ APB = abcluctor pollicis bl 밍 1:;‘
OP = opponens pollicis; R = radial sicle; 0 = c1istal sicle
B
A
C
Young C;oo Kill1, el al
FDP 2, and the median nerve is rotated and displaced inferiorly, by which FDS 3 is dis- placed downward (Fig. 1 c,d).
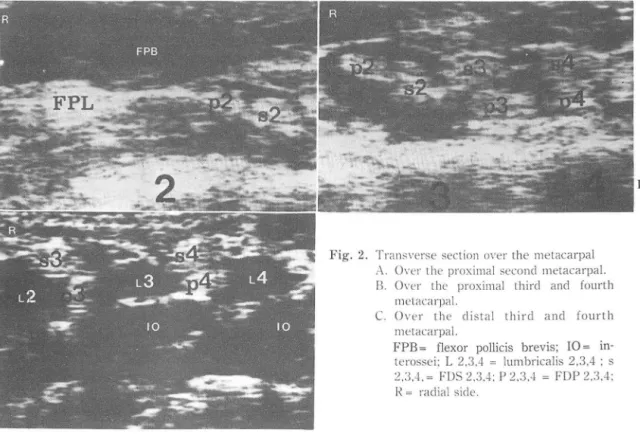
(2) Over the Metacarpal
1n contrast to the narrow carpal canal, each tendon spreads out, and is well separated by the adjacent lumbrical muscles, and echogene- city of which is much hypoechic than that of the tendon. The FPL tendon become buried in the thenar muscles (Fig. 2a, 3a). In trans- verse sections, the FDS and FD P tendons form an vertical 2-1ayer arrangement with the FDS occupying the superficial position, and the FDP running deeper to the FDS except the flexor tendons to the index finger. The FDS 2 and FDP 2 tendons have an horizontal 2-1ayer arrangement: the FDP 2 lies in radial side of the FDS 2 (Fig. 2).
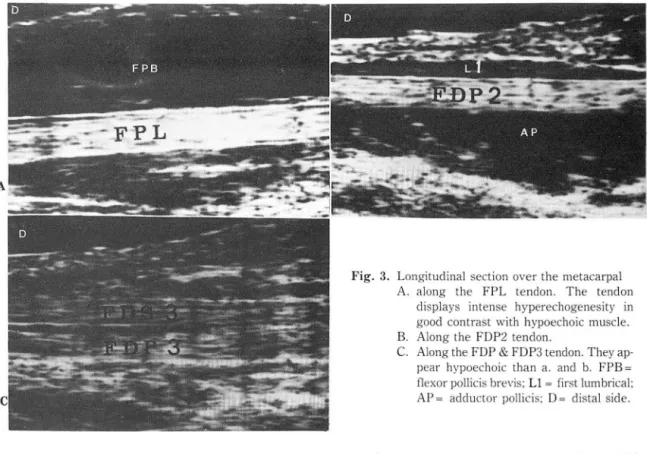
1n longitudinal sections, they show typical ultrasonographic features of the tendon: a
Digital Flexor Tenclons of the Hand -
hypoechoic tubular density composed of multi- ple fine paral1el echogenic lines, which repre- sents collagen fibrils of the tendon (Fig. 3).
(3) the Digital Canal
The FDS tendon lies superficial to the FDP tendon in transverse section over the proximal phalanx until the FDS splits into two halves, and is penetrated by the FDP, where the each half embraces the FDP on its both sides. On the further distal section of the proximal phalanx, the each half is found deep to the FDP: the position of each half of the FDS changes from a superficial to a lateral, and then a deep side of the FDP (Fig. 4).
On the paramidline longitudinal section over the middle phalanx, the insertion site of the FDS on the palmar aspect of the middle phalanx can be clearly depicted. The insertion of the FDP at the base of the distal phalanx is also delineated (Fig. 5).
Fig. 2. Transverse section over the ll1etacarpal
À. Over lhe proxill1al seconcl melacarpal B. Over the proxill1al thircl ancl fourth
melacarpal
C. O\'er the clistal thircl ancl fourth metacarpal
FPB = flexor pollicis brevis; 10 = in- terossei; L 2,3.4 = lumbricalis 2,3.4 ; s 2.3.4. = FDS 2.3.4; P 2.3.~ = FDP 2.3.4;
J~ = raclial sicle
- 305-
B
- The Journal of the Korean Radiological Society, Vol. 23, No. 2‘ 1987 -
DISCUSSION
The echogenecity of the tissue is related primarily to the stiffness of it, and collagen is considered a major source of the echogeneci- ty.6) Rich collagen fibrils of the tendon seem to make them highly echogenic, and provide a good contrast to the adjacent tissues such as muscle or nerve, which contains less col- lagen. But the tendon may vary in the echo- genecity from the intense hyperechoic one to the falsely hypoechoic one due to various rela- tionships between the angle of the acoustic beam and the orientation of the tendon fibrils (Fig. 3). For that reason, subtle control of transducer angle should be done during the scannmg.
The digital flexor tendons were most easi- ly demonstrated over the metacarpals, be- cause they are well separated by lumbrical muscles. On the other hand, in the carpal
Fig. 3. Longitudinal section over the metacarpal A. along the FPL tendon. The tendon
displays intense hyperechogenesity in good contrast with hypoechoic muscle B. Along the FDP2 tendon
C. Along the FDP & FDP3 tendon. They ap- pear hypoechoic than a. and b. FPB = flexor pollicis brevis; L1 = first lumbrical;
AP = adductor pollicis; 0 = distal side
canal, where the tendons are crowded within the narrow space, the clear delineation of each tendon was somewhat troublesome, but they could be identified and defined by observing the movement of each tendon during flexion and extension of each finger. The median nerve within the carpal canal, which is com- pressed in carpal tunnel syndrome, was easi- ly distinguished due to its lower echogenecity than that of the tendons surrounding it
Other imaging modalities, computed tomo- graphy (CT) and magnetic resonance(MR), also enabled to depict the soft tissue structures of the hand and wrist.7-9) Especially MR, with its multiplanar capabilities and high contrast resolution, visualized the intricate anatomy of the hand and wrist excellantly.9) 1n com- parison with MR, ultrasonography is capable of multiplanar imaging with comparable quali- ty of the image. 1n addition to low cost and short imaging time, ultrasonography has an advantage of realtime imaging which enable B
- Young Goo Kim, et al.: Digital Flexor Tendons of the Hand -
A B
D
Fig. 4. The digital canal over the proximal phalanx of middle finger
A .
-\. The miclline longitudinal section. The FDS is found over the FDP in proximallevel, and behind the FDP in distallevel.
B.C. D. Transverse section of the proximal phalanx
b. at the base. c. at the midportion. c1. at the distal portion s = FDS;P = FDP; mp = metacarpophalangeal joint; D = distal side
Fig. 5. The c1igital canal: the insertion of FDS ans FDP. (x 2 magnification)
.-\. The paramiclline longitudinal section of the middle phalanx. The insertion site of the FDS tendon at the midportion of midclle phalanx (arro、\.)
R. Longituclinal section of the distal phalanx. The insertion site of the FDP (arrow) PIP = proximal interphalangeal joint; DIP = distal interphalangeal joint; 0 = c1istal side.
307
B
- The Journal of the Korean Radiological Society, Vol. 23, No. 2, 1987 -
us to evalute the movement of tendons and the relationships between them. Thus, ultra- sonography is expected to be a useful ex- amination for the assessment of the varous conditions of digital flexor tendons and their adjacent soft tissues including trauma, tumor and carpal tunnel syndrome.
CONCLUSION
The ultrasonographic sectional anatomy of digital flexor tendons of the hand and their neighbouring tissues were successfully de- monstrated by high-resolution ultrasono- graphy. The understanding of the normal ultrasonographic findings of them will provide a useful background for the ultrasonographic diagnosis of their pathologic conditions.
ACKNOWLEGEMENT
We would like to express our thanks to J ae Myoung Jeon, M.D. of the Department of Or- thopedics, Chung Ang university hospital, for his valuable advice about the surgical anatomy of the hand.
REFERENCES
1. Fornage BD, Rifkin MD, Touch DH et al: Sonography of the pate/la tendon: a preliminary experience. A}R 143:179,182, 1984
2. Fornage BD: Achi/les tendon: US examination. Radiology 159:759.764, 1986
3. Blei CL, Nirschl RP, Grant EG: Achilles tendon: US diagnosis of pathologic conditions. Radiology 159:765.767, 1986 4. Fornage BD, Schernberg FL, Rifkin MD: US examination
of the hand. Radiology 155:785,788, 1985
5. Spinner M: Kaplan's functional and surgical anatomy of the hand. 3rd Ed. 59-61 }.B. Lippioneott companι Philadelphia, 1984
6. Rosenfield AT, Taylor Kj, jaffe CC: Clinical application of ultrasound tissue characterization. Radiology Clinical Noπh Am 18:31, 1980
7. Cone Ro, Szabo R, Resnick D et al: CT of the normal soft tissues of the wris t. Invest Radiology 18:546-551, 1983 8. Zucker.Pinchoff B, Hermann G, Srinivasan R: CT of the car- pal tunnel: A radioanatomical study. } Comput Assist Tomogr 5:525-528, 1981
9. Weiss KL, Beltran J, Shamam OM et al: High-ηeld MR surface-coil imaging of the hand and wrist:part 1. normal anatomy. Radiology 160:143-146, 1986