INTRODUCTION
The injury of the posterior cruciate ligament (PCL) occurs in 1%-4% of all acute knee injuries [1-3]. For isolated PCL injuries, it has been shown that a preserving technique gives good clinical outcomes [4,5], and thus controversy still exists as to whether intervening surgically is beneficial or not. However, recently, surgical intervention of PCL has been on the increasing trend as a PCL deficient knee was associated with the formation of articular damage and development of secondary degenerative arthritis due to increase in pressure on the medial compartment and the patellofemoral joint [6-8].
The functional unit of PCL can be divided into either the anterolateral bundle or the posteromedial bundle [9].
These two bundles have complementary roles to prevent posterior translation. At 90o flexion of the knee, the anterolateral bundle is involved in preventing posterior translation, whereas at extension of the knee, the posteromedial bundle is responsible. The anterolateral bundle has been shown to have a greater diameter than the posteromedial bundle, and thus is thicker [10]. However, despite this complementarity of the two bundles, during anatomic singlebundle reconstruction, it is usually the anterolateral bundle that is reconstructed [11,12].
The PCL has a greater ability to naturally heal than the anterior cruciate ligament because of its close proximity to the branch of the middle genicular arch and the fact that it is surrounded by a thick layer of synovium. According
Arthroscopic augmenting reconstruction of the anterolateral bundle in isolated posterior cruciate ligament injuries using the remnant bundle-preserving technique
Sang Bok Lee, Jae Ang Sim, Yong Seuk Lee, Beom Koo Lee
Department of Orthopaedic Surgery, Gachon University Gil Medical Center, Incheon, Korea
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received August 1, 2013; Revised June 2, 2014; Accepted June 2, 2014
Correspondence to: Beom Koo Lee, Department of Orthopaedic Surgery, Gachon University Gil Medical Center, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 405-760, Korea. Tel: +82-32-460-3384, Fax: +82-32-468-5437, E-mail: [email protected] Background: The purpose of this study was to report the outcomes of arthroscopic reconstruction of posterior cruciate ligament (PCL) using the remnant bundle preserving technique, augmenting specifically the anterolateral bundle of PCL.
Methods: Thirtyseven patients who underwent an arthroscopic anterolateral bundle reconstruction with the remnant preserving technique of PCL between February 2001 and August 2010 were enrolled in this study. There were 29 male and 8 female patients with an average age of 41 years (range, 19 to 67 years). Mean followup period was 41 months (range, 12 to 103 months). The clinical outcomes were assessed by the Lysholm knee score and the International Knee Documentation Committee (IKDC) score. The radiological outcomes were assessed using the stability and stress radiograms, measured by the Telos device.
Results: The preoperative Lysholm knee score improved significantly from a mean 75.3 ± 12.8 value to a postoperative mean of 91.2 ± 5.8 (P < 0.05). Likewise, the preoperative IKDC subjective score improved from a mean value of 72.0 ± 11.6 to a postoperative mean of 87.8 ± 5.0 (P < 0.05). Further, stress radiographs showed a decrease in the average side to side difference of posterior tibial translation from 8.4 ± 4.1 mm to 4.0 ± 2.8 mm, before and after the operation (P < 0.05).
Conclusion: The clinical and stability results improved in patients with isolated PCL injury after arthroscopic augmenting PCL reconstruction using the remnant preserving technique.
Keywords: Knee; Posterior cruciate ligament; Reconstruction; Remnant preservation
Arthroscopy and Orthopedic Sports Medicine
AOSM
to our past experiences, we have seen arthroscopically that even if the posterior translation is larger than 10 mm, preserving the PCL results in enhanced continuity. As such, in this study we preserved any remnant PCL whilst anatomically reconstructing the anterolateral bundle.
METHODS
Study subjects
The current study was approved by the Medical Ethics Committee at the Gachon University Gil Medical Center (GAIRB 2013175). A total of 37 patients who had been operated on at our department between February 2001 and August 2010 were enrolled. The ratio of sex was 29 males and 8 females, with an average age of 41 years (range, 19 to 67 years). The final followup took place at an average 41 months after the operation (range, 12 to 103 months). All patients were immobilized with the leg at extension using a cast for 8 weeks from the time of injury. Reconstruction of the PCL was carried out when subsequent clinical or radiological tests indicated knee instability of grade 3 or higher (Fig. 1).
Analysis
The clinical outcomes were assessed using the Lysholm score and the International Knee Documentation Committee (IKDC) subjective score at two time points, preoperation and at the final followup. The radiological outcomes were assessed by measuring the posterior tibial translation on the stress radiogram using a Telos device (Telos, Marburg, Germany).
Surgical methods
In all patients, the Achilles tendon allograft was used.
Diagnostic arthroscopy was performed as standard prior to all reconstruction procedures. Four portals were created for the surgery.
An anteromedial portal was created higher than nor mally so it was closer to the patella ligament. This allowed easier access to the tibial attachment site. The posteromedial portal was created using the transillumination technique.
A rod was inserted anterior to the PCL through this posteromedial portal, and then taken out through the posterolateral side. At the posterolateral side, all remnant bundles were retracted to confirm the tibial attachment
Fig. 1. (A) Preoperative stress radiography shows 11.23 mm posterior translation of side to side difference. (B) Postoperative stress radiography shows 3.11 mm posterior translation of side to side difference.
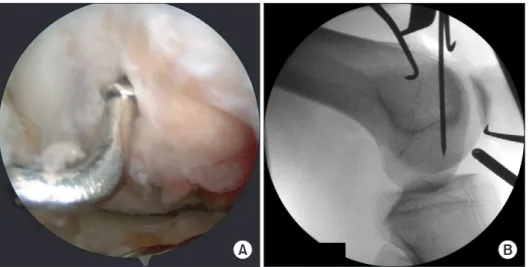
Fig. 2. (A) The remnant posterior cruciate ligament (PCL) is retracted using a rod via the posterolateral portal (viewed from the posteromedial portal). (B) Tunnel position was confirmed by a Carm after a guide pin was inserted.
site (Fig. 2A).
The tibial attachment site was rasped through the post
eromedial portal before making the tibial tunnel. The guide was placed so it was 1 cm below the articular surface of the tibia, lateral to the tibial attachment of the PCL, and at the center of the anterolateral bundle. An incision was made 3-4 cm medially to the tibial tubercle to insert the guide pin, which was then confirmed by radiography (Fig. 2B).
The femoral tunnel was created using the outsidein technique. For the right knee, the femoral tunnel was positioned as when the large handle of a clock would be at half past twelve or at 1 o’clock. Whereas for the left knee, the tunnel was positioned as when the large handle of a clock would be at 11 o’clock or at half past eleven. In both cases, the tunnel was placed at the center of the anterolateral bundle (Fig. 3A). A guide pin, detected by radiography, was inserted to aid correct positioning of the tunnel (Fig.
3B). Tibial fixation was achieved using a bioabsorbable interference screw. A preassembled pullout knot was hung on the screws and was fixed and made taut distally before making a final second endloop knot. Femoral fixation was achieved using a gold interference screw and posttied as before.
Rehabilitation
For rehabilitation, all patients wore a long legcast on the operated leg with the leg at 180o extension for 2 weeks after the operation, and thereafter the cast was exchanged with a supportive brace until the 3rd postoperative month. Full weightbearing was allowed given that the patients wore either the cast or the supportive brace. Two days after the operation, the patients were begun passive patellar range of motion (ROM) exercises to strengthen
the quadriceps femoris muscles and to prevent stiffness of the patella. The ROM exercises were performed 1-2 times a day at protraction and were gradually allowed up to 90o rotation during the first 3 months. After the 3 months, the patients were allowed active knee flexion and patient’s ROM was not limited.
Statistical analysis
All statistical analyses were carried out using IBM SPSS Statistics 20.0 (IBM Co., Armonk, NY, USA). Significance was set to a Pvalue < 0.05. A paired ttest was used to compare the preoperative and postoperative clinical and radiological outcomes.
RESULTS
At the final followup, we found that the tibial translation that was 8.4 ± 4.1 mm preoperatively decreased signifi
cantly to 4.0 ± 2.8 mm postoperatively through the posterior stress radiogram with the knee at 90o flexion (P < 0.05). We also found both the postoperative Lysholm score and the IKDC subjective score improved from 75.3 ± 12.8 to 91.2 ± 5.8, and 72.0 ± 11.6 to 87.8 ± 5.0, respectively compared to the preoperative scores (P < 0.05) (Table 1).
Fig. 3. (A) Femoral socket center was placed 3-4 mm posterior to the articular junction and at an 11 o’clock angle (in the left knee). (B) Tunnel position was confirmed by a Carm after guide pin was inserted.
Table 1. Outcomes of PCL reconstruction in the isolated injury group Preoperation Last followup Pvalue Lysholm
IKDC
Posterior stress view (mm)
75.3 ± 12.8 72.0 ± 11.6 8.4 ± 4.1
91.2 ± 5.8 87.8 ± 5.0 4.0 ± 2.8
< 0.05
< 0.05
< 0.05 PCL, posterior cruciate ligament; IKDC, the International Knee Documentation Committee.
DISCUSSION
Natural healing of acute PCL injuries has been proven in animal studies [13] and through magnetic resonance imaging studies [14,15]. Although posterior translation was found in patients with chronic PCL injury during diagnostic arthroscopy, the authors also found that the PCL still retained its continuity and synovium cover in most cases. Further, Safran et al. [13] found that 29 months of preservative treatment in 18 patients with isolated PCL injury led to comparable levels of proprioception of the affected leg after treatment to the unaffected contralateral leg. However, Dejour et al. [16] found that although patients with isolated PCL injury returned to highenergy sports after 12 months of preservative treatment, later it was associated with increased chances of degenerative arthritis. The benefits of remnantpreserving techniques are that the remnant ligaments would aid healing by supplementing blood supply, promoting revascularization, and protecting the graft, even though the elongated remnant ligaments would not contribute to stability. Therefore, it is thought that maximal effects will be seen if the injured PCL is preserved as much as possible and the reconstruction is made around the anterolateral bundle. If the internal splint method is followed, it is also thought that sufficient crosssectional surface will be achieved. Furthermore, functional benefits are also expected as proprioception function and graft stability could be maintained [17].
We created tibial tunnels to fix the grafts and used a rasp to decrease the changes in grafttibial angle, which would minimize the Killer turn effect. In most patients, the PCL was found to be extended at diagnostic arthroscopy,
however continuity was largely retained. Therefore, we were able to preserve the posteromedial bundle and perform singlebundle anatomical reconstruction around the anterolateral bundle using the crosssection of the graft.
Ahn et al. [18] performed PCL reconstruction using the remnant ligament preserving technique on 60 patients.
At the final followup of at least 2 years, they saw an improvement of the Lysholm score from a preoperative value of 65.8 to a postoperative value of 92.9, and a decrease in the posterior translation from a mean 12.95 mm to a mean 2.79 mm. When Kim et al. [19] performed a PCLpreserving arthroscopic reconstruction they found improved Tegner activity scale, nearreturn to activity, IKDC subjective score, but not difference in stability, than when they performed a PCL nonpreserving arthroscopic reconstruction. In this study, we also found similar levels of improvements in the clinical and radiological outcomes when pre and postoperative values were compared in patients who underwent the remnantpreserving technique.
In sum, we generally found continuity of the postero me
dial bundle of the PCL in patients with isolated PCL injury.
We found that performing an augmenting reconstruction of the PCL using the anterolateral bundlepreserving technique showed improved clinical and radiological outcomes in these patients.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Hughston JC, Degenhardt TC. Reconstruction of the posterior cruciate ligament. Clin Orthop Relat Res 1982;164:59-77.
2. Parolie JM, Bergfeld JA. Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med 1986;14:35-8.
3. Fanelli GC, Giannotti BF, Edson CJ. The posterior cruciate ligament arthroscopic evaluation and treatment. Arthroscopy 1994;10:673-88.
4. Kim YM, Lee CA, Matava MJ. Clinical results of arthroscopic single-bundle transtibial posterior cruciate ligament recon- struction: a systematic review. Am J Sports Med 2011;39:425- 34.
5. Ahn JH, Seo HS. Natural history of conservatively treated post-
erior cruciate ligament injury. J Korean Arthrosc Soc 2007;11:
13-9.
6. Skyhar MJ, Warren RF, Ortiz GJ, Schwartz E, Otis JC. The effects of sectioning of the posterior cruciate ligament and the posterolateral complex on the articular contact pressures within the knee. J Bone Joint Surg Am 1993;75:694-9.
7. Logan M, Williams A, Lavelle J, Gedroyc W, Freeman M. The effect of posterior cruciate ligament deficiency on knee kinematics. Am J Sports Med 2004;32:1915-22.
8. Van de Velde SK, Bingham JT, Gill TJ, Li G. Analysis of tibiofemoral cartilage deformation in the posterior cruciate ligament-deficient knee. J Bone Joint Surg Am 2009;91:167-75.
9. Harner CD, Xerogeanes JW, Livesay GA, et al. The human post-
REFERENCES
erior cruciate ligament complex: an interdisciplinary study. Liga- ment morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-45.
10. Covey DC, Sapega AA, Riffenburgh RH. The effects of sequential sectioning of defined posterior cruciate ligament fiber regions on translational knee motion. Am J Sports Med 2008;36:480-6.
11. Matava MJ, Ellis E, Gruber B. Surgical treatment of posterior cruciate ligament tears: an evolving technique. J Am Acad Orthop Surg 2009;17:435-46.
12. Sekiya JK, West RV, Ong BC, Irrgang JJ, Fu FH, Harner CD. Clinical outcomes after isolated arthroscopic single-bundle posterior cruciate ligament reconstruction. Arthroscopy 2005;21:1042- 50.
13. Safran MR, Allen AA, Lephart SM, Borsa PA, Fu FH, Harner CD.
Proprioception in the posterior cruciate ligament deficient knee.
Knee Surg Sports Traumatol Arthrosc 1999;7:310-7.
14. Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR. The posterior cruciate ligament injured knee: principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
15. Seon JK, Song EK, Bae BH, et al. Kinematic study following double-bundle, anterior cruciate ligament reconstruction. Int Orthop 2007;31:623-8.
16. Dejour H, Walch G, Peyrot J, Eberhard P. The natural history of rupture of the posterior cruciate ligament. Rev Chir Orthop Reparatrice Appar Mot 1988;74:35-43.
17. Jung YB, Jung HJ, Tae SK, Lee YS, Yang DL. Tensioning of remnant posterior cruciate ligament and reconstruction of anterolateral bundle in chronic posterior cruciate ligament injury. Arthroscopy 2006;22:329-38.
18. Ahn JH, Yang HS, Jeong WK, Koh KH. Arthroscopic transtibial posterior cruciate ligament reconstruction with preservation of posterior cruciate ligament fibers: clinical results of minimum 2-year follow-up. Am J Sports Med 2006;34:194-204.
19. Kim SJ, Kim SH, Chun YM, Hwang BY, Choi DH, Yoon JY. Clinical comparison of conventional and remnant-preserving transtibial single-bundle posterior cruciate ligament reconstruction com- bined with posterolateral corner reconstruction. Am J Sports Med 2012;40:640-9.