대 한 방사선 의 학회 지
1994: 30(4) : 621-626
경추외상의 자기공명영상소견 I
정 선 관 · 이 겸 수
·
손광춘·
최 시 성·
원 종진목 적 : 경추 외상시 자기공명영상에 나타나늠 소견들을 알아보기 위하여.
대상 및 방법 겸추 외상을 당한 34 명 환자의 경추 자기공명영상에 관찰되는 소견들을 척수, 척추, 인 대, 추간판 등을 중심으로 후향적 분석을 하였으며, 모든 환자에서 1.0T 초전도형 자기공멸영삼기
(Siemens Magnetom
42SPE) 를 이용하여 영상을 얻었다.결 과 척수 압박 15예, 척수 부종 4예, 척수 공동증 4예, 척수 연화증 1 예, 출혈성 좌상 1예 등을 포 함한 총 25예의 척수의 이상 소견과 18예의 인대 손상, 22예의 추간판 탈출증, 15예의 척추 골절 및 아 탈골 등의 소견이 관잘되었다.
결 론:자기공명영상은 경추 외상 환자에서 척수 손상의 유무, 정도 및 특성을 평가할 수 있고, 주변 연조직 및 경추골의 변화를 관잘하는데 유용한 검사이다.
서 료응
‘-
교통수단의 발달과 함께 그 이용이 급증함에 따라 교통 사고에 의한 척추외상환자가 더불어 증가하고 있다. 외상 에 의한 척추골절이나 전위시 척수 손상이 10-14%에서 동반되며, 특히 경추가 척수 손상의 많은 부분을 차지한다
(1,
2).
척추손상의 진단방법으로 단순촬영, 척수조영술, 전 산화단층촬영술 등이 사용되어 왔으나 척수실질이나 주위 연조직의 손상을 진단하는데는 어려움이 많았다 (3-5). 반 면에 최근 이용이 증가하고 있는 자기공병영상 (이하 MRI로 약함)은 척수를 직접 영상화하고 주변 연조직 변 화를 볼 수 있어서 척추 손상의 유무 및 정도, 척수의 압박 등을 잘 관찰할 수 있다 (3-11). 따라서 저자들은 경추 외상 후 MRI 에 나타냐는 소견틀을 분석하여 경 추외상시MRI
의 역활에 대하여 알아보고자 하였다.대상및방법
1991 년 10 월 부터 1992년 9월 까지 경 추외 상을 당하여 저 자들 병원에 업원하여 MRI를 시행받은 34명 (연령은
21
세에서 75세까지였고, 남자 28명, 여자 6명, 외상의 원인은 교통사고 23명, 추락사고 11 명이었음. )의 환자를 대상으로 하였으며, 수상후 MRI를 시행하기까지의 기간은 10시1 원광대학교 의과대학 방사선과학교실
이 논문은 1993년 7월 22일 접수하여 1994 년 1 월 19일에 채택되었음
- 621
간부터 14개월까지 다양하였다.
MRI는 1.
0T Magnetom 42SPE(Siemens AG , Erlan gen
, Germany) 를 이용하여spin -echo
기법으로T l(TR / TE = 500 / 15msec)
, 양자밀도(proton densi ty) (TR / TE = 2000 / 20msec)
및T2 (TR / TE = 2000 /
80msec) 강조 시상연 영상과gradient -echo(TR/TE / =400 / 12msec / 15)
횡단면 영상을 얻었다. 절편 두께는4mm
, 그 간격은 O.4mm로 하였으며, 시야(field of
view) 는230 - 280mm
,aquisi tion
matrix는256 x 256
또는192 x
256으로 하였다.MRI소견은 척수와 그 주변 연조직을 중심으로 후향적 분석을하였다.
7~ ε극 과
MRI
소견을 분석한 결과 이상 소견을 찾을 수 없었던6
예를 제외한 28예중 외상의 위치는 제5/6
경추 부위가10
예 (36%) 로 가장 많았다. 척수실질의 변화는 10예에서 나 타났으며 , 척 수부종 4 예(Fig.
1), 척 수공동증 4예(Fig.
2)
, 척수 연화증 1 예, 출혈성 좌상 l예(Fig. 3)
등 이었다.척수 압박은 15 예에서 관찰되었는데, 추간판
(Fig. 1
,4
,5)
, 경막외혈종 2예(Fig.5)
, 후방전위된 골절편, 전위 등 이 그 원인이었다. 주변 연조직 변화중 인대의 손상은12
예, 18부위에서 나타났으며, 이중 극간인대 손상이 10예로 가장 많았고, 전방종언대 손상 4예, 후방종인대 손상 2예,환추횡인대 손상 2여l 등이였다
(Fig. 3
,4
,5).
추간판 탈출 증은 22예에서 보였으며, 이중 외상부위와 일치하고T2
강 조영상에서 다른 추간판에 비해 특별하게 고신호강도를대 한 방사 선 의 학회 지 1994: 30(4) : 621- 626
보였던 6예 (Fig. 4) 와 외상부위와 일치하였으나 특별한
고신호강도를 보이 지 않았던 3예 (Fig. 5) 는 외 상에 의 한 추간판 탈출증으로 생각하였으며, 나머지 13예는 퇴행성
추간판 탈출증으로 판독하였다. 경추골 자체의 변화로는 척추외상 환자에서 골절 및 전위, 인대 손상등에 의한 척 13예, 15부위에서 관찰되었으며, 전위가 4예, 골절이 11 예 추정렬이 불안정할때 척수가 손상될 가능성이 항상 있기
에서 보였다 (Fig. 1
,
3,
4,
5). 때문에 척수의 손상유무와 정도, 특성을 아는 것은 치료방a b
a b
… ι
고 찰
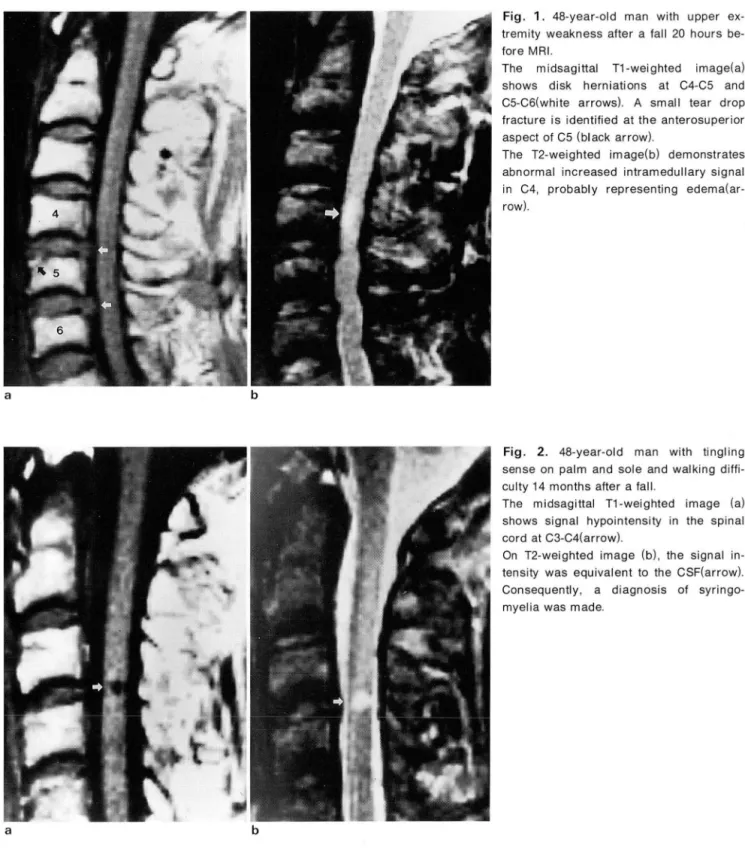
Fig. 1. 48-year-old man with upper ex- tremity weakness after a fall 20 hours be- fore MRI
The midsagittal T1-weighted image(a) shows disk herniations at C4.C5 and C5-C6(white arrows). A small tear drop fracture is identified at the anterosuperior aspect of C5 (black arrow)
The T2-weighted image(b) demonstrates abnormal increased intramedullary signal in C4
,
probably representing edema(ar- row}.Fig. 2. 48-year-old man with tingling sense on palm and sole and walking diffi- culty 14 months after a fall
The midsagittal T1-weighted image (a) shows signal hypointensity in the spinal cord at C3-C4(arrow).
On T2-weighted image (b), the signal in- tensity was equivalent to the CSF(arrow) Consequently, a diagnosis of syringo- myelia was made
침을 결정하고 예후를 예측하는데 중요하다(1,
7 , 12 , 13).
MRI는 다른 영상기법보다 더 우수한 조직간의 대조도와 다평면 영상들을얻을수있는능력때문에 척수,인대,추간 판 등을 포함한 연조직들을 잘 관찰할 수 있게끔 직접 영 상화하고,또척수와척추를비롯한그주위 조직과의 관계 를 쉽게 평가할 수 있도록 해 준다. 이런 장점 때문에 척추 외상환자에서 MRI를 시행하여 척수, 추간판, 인대, 척추 등의 손상유무 및 그 정도, 척수압박 등을 진단할 수 있다
(3 -5, 7 -14) .
척수 손상의MRI
소견은 척수의 국소 비정 상적인 팽창과 신호강도로 나타나는데, 팽창여부는T1
강 조영상에서 관찰하기 쉽고(1 1,15) , Kulkarni
등은 척수내 의 비정 상 신호강도를 T1 과T2
강조영상에서 신호강도의 변화에 따라 세가지 유형으로 분류하였다 (9). 제 1형은T1
강조영상에서 불균질 신호강도로,
T2
강조영상에서는 앓 은 테의 고신호강도에 의해 둘러싸인 중심성 저신호강도 로 보이는 형태로 척수내 출혈을 시사하며, 예후가 불량하 고, 제 2 형은T1
강조영상에서 정상척수와 동일 신호강도 로,T2
강조영상에서 고신호강도로 보일때를 말하며, 척수 부종을 가리키며 가장 많은 빈도를 차지하고예후는좋다.제 3형은
T1
강조영상에서 동일 신호강도로,T 2
강조영상 에서 두꺼운 고신호강도로 둘러싸인 중심성 동일 신호강 도의 소견으로 보이는 유형으로 출혈과 부종이 혼합된 경정선관 외 경추외상의 자기공명영상
우에 해당된다고 하였으며, 그 예후는 비교적 양호하다고 보고하였다 (9, 12, 13, 15-17). 저자들 연구에서는 제 1형에 해당하는 예는 없었고, 제 2형 (Fig. 1)은 4예, 제 3 형 (Fig.
3) 은 1예에서 관찰되였다.
척수손상의 후유증으로만성기에 출현하는병변으로척 수공동증, 지주막하낭종, 척수연화증, 반흔성 섬유화(
scarring and fi brosis)
,
만성 척수압박 등이 있는데, 이런 병변 모두를 MRI상 잘 관찰할 수 있으며, 특히 이중 수술 로 증상을 호전 시킬 수 있는 척수공동증과 수술적 치료를 할 수 없는 척수 연화증의 감별진단을 자기공명영상으로 할수 있다 (6, 13, 17-19). 이 연구에서 저자들은T1
강조영 상에서 양자 밀도 및T2
강조영상으로 신호강도가 뇌척수 액과 같게 저신호강도에서 고신호강도로 변화하여 척수 공동증이라고 진단한 4예 (Fig. 2) 와T1
강조영상에서 동 등 내지는 약간 저 신호강도로, 양자밀도 강조영상에서 동 등신호강도로,T2
강조영상에서 고신호강도로 보였지만 뇌척수액보다 낮게 보여서 척수연화증이라고 진단한 1예 를 경험했으나, 수술치료로 증상의 호전을 보인 척수 공동 증 1 예를 제외한 4예는 수술 및 병리학적 검사로 확인은 하지 못하였다.척수압박에 의한신경학적 장애가올수있고그기간이 오래될수록 장애정도가 심해질 수 있기 때문에 조기발견
a b c
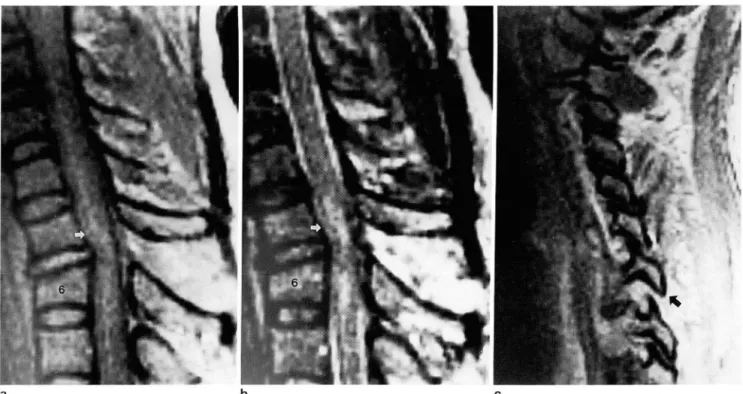
Fig. 3. 41-year-old woman with a Brown-Sequard syndrome after a motor vehicle accident 2 days belore MR I.
MR images demonstrate an area (arrow) 01 mixed increased signal within the cord on T1-weighted (a) and T2-weighted (b) sequences. These lindings are consistent with a hemorrhagic cord contusion
Rupture 01 the interspinous and supraspinous ligaments is manilested by splaying 01 the C5 and C6 spinous processes, a local discontinuity and high signal intensity on T2-weighted images. Also note mild angulation at C5-C6
The left parasagittal proton density scan (c) shows seperation 01 the C6-C7 articular lacets with anterior slippage 01 C6 inlerior process with respect to C7 (arrow)
g
대 한방사선의 학회 지 1994: 30(4) : 621- 626
이 중요하다(1 2,
13 , 17 , 18).
MRI로 척수가 어떤원인에 의해서 어느정도 압박되어 있는가를 잘 알수 있다. 저자들 은 외상성 추간판탈출증에 의한 척수압박 9예를 포함하여 총 15예에서 관찰하였고, 이외의 원인으로는 경막외혈종 (2 예),
후방전위된 골절편, 척추의 전위 등 때문이었다.MRI상 외상성 추간판탈출증(3, 7,8, 10-12, 2이은 외상부 위와 일치한 추간판의 신호강도가
T2
강조영상에서 다른a b
a b
추간판에 비해 특별하게 더 증가하였고 (Fig.4)
,
경막외혈 종은 (7, 13) 은 외상부위와 일치해서T1
및T2
강조영상상 모두 고신호강도로 보였다 (Fig. 5).인대를 직접 영상화 할 수 있다는 것이 MRI 의 또 하나 의 장점이다. 정상인대는
T1
및T2
강조영상 모두에서 저 신호강도로 보이며, 전·
후종인대, 극간인대, 황색인대, 상극인대 (supraspinous ligament) 등의 손상은
T2
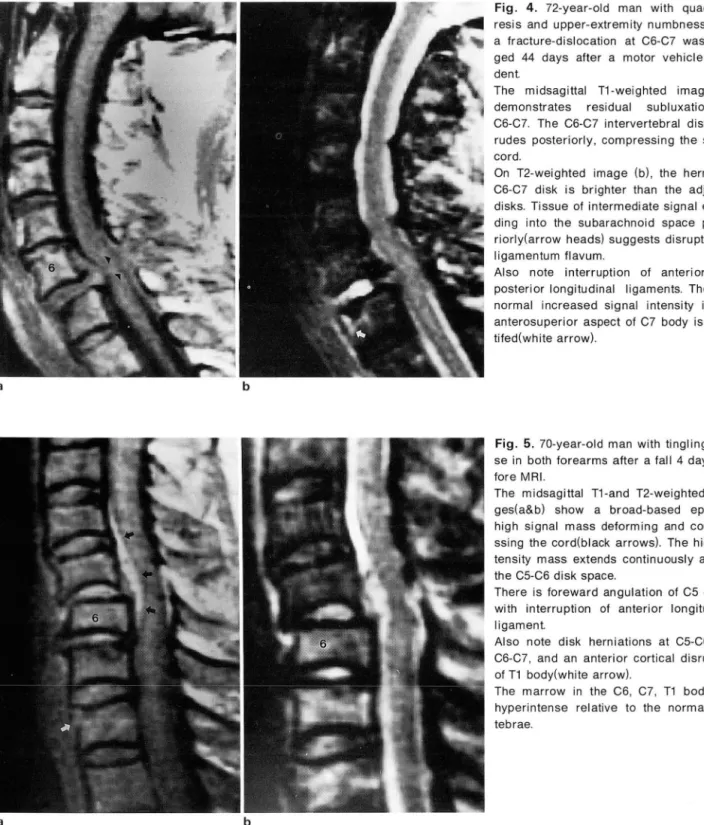
강조 시Fig. 4. 72-year-old man with quadri pa- resis and upper-extremity numbness after a Iracture-dislocation at C6-C7 was ima- ged 44 days after a motor vehicle acci.
dent
The midsagittal T1.weighted image (a) demonstrates residual subluxation at C6-C7. The C6.C7 intervertebral disk ext- rudes posteriorly, compressing the spinal cord
On T2-weighted image (b), the herniated C6-C7 disk is brighter than the adjacent disks. Tissue 01 intermediate signal exten- ding into the subarachnoid space poste- riorly(arrow heads) suggests disruption 01 ligamentum Ilavum
Also note interruption 01 anterior and
pα:;terior longitudinal ligaments. The ab- normal increased signal intensity in the anterosuperior aspect 01 C7 body is iden- tiled(white arrow)‘
Fig. 5. 70-year-old man with tingling sen- se in both lorearms after a lall 4 days be- lore MRI
The midsagittal T1-and T2-weighted ima- ges(a&b) show a broad-based epidural high signal mass delorming and compre- ssing the cord(black arrows). The high in- tensity mass extends continuously across the C5-C6 disk space.
There is loreward angulation 01 C5 on C6 with interruption 01 anterior longitudinal ligament
Also note disk herniations at C5-C6 and C6-C7, and an anterior cortical disruption
。1T1 body(white arrow)
The marrow in the C6, C7, T1 bodies is hyperintense relative to the normal ver- tebrae‘
- 624 -
상면 영상에서 잘 관찰할 수 있다 (3, 7, 8, 10-12, 20). 이 연 구에서는 34명중 12명 (35%) 에서 인대의 손상이 있었고,
극간인대 손상이 가장 많은 부분을 차지했고, 그 소견은
T2
강조 시상변 영상에서 인접 극돌기 (spinous process) 간격이 넓어지고 정상 저신호 강도가 고신호 강도로 대체 되어 보였으며 (Fig.3) ,
종인대의 경우 갑작스런 중단이 보일때 (Fig.4,
5) 손상이 있다고 판독하였다. 척추의 골절 을 진단하는데는 아직까지도MRI
보다는 전산화 단층촬 영이 더 우수하지만, 척추의 정렬 (Fig.3 ,
5)을 보는데는 MRI가 더 우수하다(1,3 , 7 , 11 -13).
MRI 상 추체 골절 (Fig. 1,4 ,
5) 은 행태의 이상, 정상 신호강도의 변화, 모든 영상에서 신호를 내지 않는 피질골의 중단등의 소견으로 나타난다(1 2). 골절을 평가할때 단순 촬영이나 전산화단층 촬영’으로는 진단할 수 없으나 MRI로 진단할 수 있는 추체 의 골소주만을 손상시키는 압박 골절 (Fig.5) 이 있다는 사 실은 특기할 만하며T2
강조영상에서 고신호강도로,T1
강조영상에서는 저신호 강도로 보인다 (3, 9,
10 , 15).
결론적으로 MRI상 척수손상의 유무, 정도 및 그 특성을 평가 할수 있을 뿐만 아니라 경추골, 주변연조직의 변화도 관찰할 수 있어서 치료방침 결정과 예후 판정에 큰 도움을 주기 때문에 경추 외상환자가 신경학적 검사상 이상을 갖 는 경우 MRI는 필수척 검사라고 생각한다.
j<;J
I그 고 L!:" C그 헌
정선관 외 · 경추외상의 자기공명영상
ance imaging 01 the chronically i 미 ured cervical spinal cord AJNR 1986; 7: 457.464
7. Tarr RW
,
Drolshagen LF,
Kerner TC,
Allen JH,
Partain CL,
James AE. MR imaging 01 recent spinal trauma. J Comput Assist Tomogr 1987; 11 : 412-417
8. Mirvis SE
,
Geisler FH,
Jelinek JJ,
Joslyn NJ,
Gellad F. Acute cervical spine trauma:evaluation with 1. 5-T MR imaging.Radiology 1988; 166 : 807 -816
9. Kulkarni MV
,
Bondurant FJ,
Rose SL,
Naragana PA. 1.5 tesla magnetic resonance imaging 01 aucte spinal trauma Radiographics 1988; 8 : 1059-108210. Beers GJ
,
Raque GH,
Wagner GG,
et a l. MR imaging in acute cervical spine trauma. J Comput Assist Tomogr 1988; 12 755-76111. Kallas 1
,
Wilberger J,
Goldberg A,
Prostko ER. Magnetic resonanc imaging in acute spinal cord trauma. Neurosurgery1988; 23 : 295-299
12. Flanders AE
,
Schaeler DM,
Doan HT,
Mishkin MM,
Gonzalez CF, Northrup BE. Acute cervical spine trauma: Correlation 01 MRimaging lindings with degree 01 neurologic delici l. Radi-。 logy 1990; 1 77 : 25-33
13. Maravilla KR , Cohen WA. MRI atlas of the spine. 1 st ed London : Martin dunitz 1991 : 302-339
14. Yamashita Y
,
Tachahashi M,
Matsuno Y,
et al. Acute spinal cord injury: Magnetic resonance imaging correlated with myelopathy. BJR 1991 ; 64 : 201-20915. Kulkarni MV
,
McArdle CB,
Kopanicky 0,
et al. Acute spinal cord i 미 ury: MR imaging at 1.5T. Radiology 1987; 164‘837-843
16. Hackney DB
,
Asato R,
Josph PM,
et al. Hemorrhage and edema in acute spinal cord compression: demonstration by MR imaging. Radiology 1986; 161 : 387-3901. Rogers LF. Radiology of ske/etal trauma. 2nd ed. NewYork: 17. Yamashita Y, Takahashi M, Matsuno Y‘ et al. Chronic i 미 urles Churchill living stone, 1992: 439-592 01 the spinal cord: assessment with MR imaging. Radiology 2. Berquist TH. Cervical spine trauma. Radiology 1991 ; 178: 591 1990; 175: 849-854
3. McArdle CB
,
Crofford MJ,
Mirlakhraee M,
Amparo EG,
18. Gebarski SS,
Magnard FW,
Gabrielsen TO,
Knake JE,
Latack Calhoun JS. Surlace coil MR 01 spinal trauma: Preliminary JT, Hoff JT. Posttraumatic progressive myelopathy. Radiologyexperience. AJNR 1986;7: 885-893 1985; 157: 379-385
4. Goldberg AL
,
Rothlus WE,
Deeb ZL,
et a l. The impact 01 mag- 19. Masaryk T J,
Shah M. The cervicothoracic spine. In: Higgins netic resonance on the diagnostic evaluation 01 acute CB,
Hricak H,
Helms CA,
eds. Magnetic resonance imaging cervicothoracic spinal trauma. Ske/etal Radiol 1988; 17: 89-95 of the body. 2nd ed. New York: Raven press , 1992: 1 023-1 054 5. Goldberg AL,
Rothlus WE,
Deeb ZL,
et al. Hyperextension inju- 20. Davis SJ,
Teresi LM,
Bradley WG,
Jr.,
Ziemba MA,
Bloze AE.ries 01 the cervical spine. Skeletal Radiol 1989; 18: 283-288 6. Quencer RM
,
Sheldom JJ,
Post MJD,
et al. Magnetic reson-Cervical hyperextension 미 uries: MR lindings. Radiology 1991 ; 180: 245-251
%
ι
대 한 방사선 의 학회 지
1994: 30(4): 621-626
Journ
al of theKore
an Radiological Society, 1994
: 30(4) : 621
-626
Magnetic Resonance Imaging of Traumatic Cervical Injury
SK Juhng , M
.D., KS Lee , M.D
.,KJ Sohn , M.D. , SS Choi , M.D. , JJ Won , M.D.
Department o( Radiology
,
Wonkwang University School o( MedicinePurpose: To evaluate magnetic resonance imaging (MRI) findings of cevical injuries.
Materials and Methods: MRI studies of 34 patients with cervical
spinal 미 urieswere analyzed retrospectively
.AII MRI scans were obtained with an 1.0T superconductive MRI scanner (Siemens Magnetom 42SPE) and their findings were analyzed regarding the spinal cord, bony spine
,ligaments, and intervertebral disks
Results: A variety of abnormal findings were detected: 25 cord abnormalities including cord compression (15 cases), cord edema (4 cases) , syringomyelia (4 cases)
,myelomalacia (1 case l, and hemorrhagic contusion (1 case)
,18 ligamentous injuries, 22 disk herniations (9 post-traumatic, 13 chron ic degenerative)
,11 spine fractures , and 4 subluxations.
Conclusion: MRI is useful in evaluating the spinal cord itself , in depicting ligamentous injuries , in establishing the presence of disc herniation , and in assessing the alignment of cervical spine
Index Words: Spine
,MR studies Spine
,injuries
Spinal cord , MR studies Spinal cord
,injuries Trauma
Address