서 론
순환기계 질환은 2015년 통계청이 발표한 사망 원인별 사망자 수 에서 2위를 차지할 만큼 사망 원인에서 높은 비중을 차지하고 있다.1) 관상동맥질환은 위험인자를 관리함으로써 질환을 예방하고 사망 률을 줄일 수 있다는 점에서 위험인자의 관리가 중시되고 있다.2) 콜 레스테롤은 나이, 당뇨, 흡연, 고혈압 등과 함께 관상동맥 질환의 위 험인자이며, 생활 습관 개선이나 약물 복용으로 혈중 콜레스테롤 수 치를 낮춤으로써 관상동맥 질환의 위험도를 감소시킬 수 있다는 사
실이 많은 연구를 통해 알려져 있다.3,4) 현재까지 대부분의 전문가들 이 참고하고 있는 이상지질혈증 치료 지침인 National Cholesterol Ed- ucation Program Adult Treatment Panel III (NCEP ATP III)에서는 동 반 위험요소를 평가하여 위험군을 분류하고, 저밀도 지단백 콜레스 테롤(low density lipoprotein cholesterol, LDL-C)을 이상지질혈증의 진 단 기준으로 하여 각각에 대한 치료 목표를 제시하고 있다.5)
NCEP에서는 베타 정량법을 사용하여 LDL-C를 직접 측정하였지 만 이 방법은 고가의 장비, 복잡한 방법 등으로 일상적으로 사용하 기에는 제한이 있다. 그 외에 LDL-C의 측정방법으로 액체 크로마토
Original Article
관상동맥질환 위험 인자를 가진 성인에서 저밀도 지단백 콜레스테롤의 실측값과 계산값에 따른 비교
강지혜
1, 권혁천
1, 서 민
1, 장지형
1, 조재범
2,*, 김홍태
2, 김인선
21광명성애병원 가정의학과, 2성애병원 가정의학과
Difference of Treatment Target between Direct Measurement and Calculated Measurement of Low Density Lipoprotein Cholesterol in Those Who Have Coronary Heart Disease Risk Factor
Jee Hye Kang
1, Heug Chun Keon
1, Min Seo
1, Ji Hyeong Jang
1, Jae Bum Cho
2,*, Hong Tae Kim
2, In Seon Kim
21Department of Family Medicine, Gwangmyeong Sungae Hospital, Gwangmyeong; 2Department of Family Medicine, Sungae Hospital, Seoul, Korea
Background: Cardiovascular disease has a high mortality, which treatments aim to reduce. Low-density lipoprotein cholesterol is one of the risk factors for coronary heart disease, and is also a therapeutic target in its treatment. In this study, we investigated therapeutic targets by comparing directly measured values with calculated values obtained using the Friedewald formula.
Methods: We studied individuals who had undergone a general health examination at a general hospital from 2014 to 2015. Men aged 45 years or older and women aged 55 years or older with high-density lipoprotein cholesterol levels less than or equal to 40 mg/dL were selected. Subjects completed questionnaires and were interviewed about family history and medical history. Measured low-density lipoprotein cholesterol levels were compared with the calculated levels.
Results: On comparing directly measured values to calculated values, directly measured values were significantly higher than calculated values. There was a significant difference in the number of the therapeutic targets between calculated values and measured values.
Conclusion: In case of patients who have coronary heart disease risk factors, directly measured values may be more helpful than calculated values to identify those who need to be treated and evaluate the effect of treatment.
Keywords: Low-Density Lipoprotein Cholesterol; Coronary Heart Disease Risk Factor; Friedewald Formula; Direct Measurement
http://dx.doi.org/10.21215/kjfp.2016.6.4.276eISSN 2233-9116
Korean J Fam Pract. 2016;6(4):276-280
KJFP
Korean Journal of Family PracticeReceived March 8, 2016 Revised April 27, 2016 Accepted May 5, 2016 Corresponding author Jae Bum Cho
Tel: +82-2-840-7114, Fax: +82-2-840-7388 E-mail: [email protected]
Copyright © 2016 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
강지혜 외. 저밀도 지단백 콜레스테롤의 실측값과 계산값에 따른 비교 Korean Journal of Family Practice
KJFP
Original Article
Korean Journal of Family Practice 그래피법, 전기영동법, 침전법, 면역침전법, 계산법 등이 있다. 계산법
으로는 총 콜레스테롤(total cholesterol, TC), 고밀도지단백 콜레스테 롤(high density lipoprotein cholesterol, HDL-C), 중성지방(triglyceride, TG)을 이용하여 계산하는 Friedewald 공식이 사용되고 있다.6) 계산 법은 환자가 추가적인 비용 부담 없이 LDL-C를 알 수 있다는 장점이 있지만 TG를 공복에 측정해야 하며 TG가 400 mg/dL 이상인 경우 계 산식을 사용할 수 없으며 TG 200 mg/dL 이상 또는 당뇨, 말기신장병 증, 간질환 등이 있을 때는 공식이 부정확하다는 등 제한점이 있다.7)
심혈관계 건강검진의 목적인 ‘치료 대상의 조기 발견’과 ‘심혈관계 질환의 예방’에서 보았을 때, 치료 대상 여부의 판단은 중요한 의미 를 가지며, 관상동맥질환 위험인자를 많이 가지고 있는 경우에서는 보다 적극적인 관리가 필요하다. 본 연구에서는 이를 고려하여 관상 동맥질환 위험인자 중 비교적 객관적인 두 가지 항목인 HDL-C 값과 나이를 기준으로 하여, 낮은 HDL-C 값을 가진 45세 이상 남성, 55세 이상 여성의 LDL 콜레스테롤의 실측값과 Friedewald 공식을 이용한 계산값이 어느 정도의 오차를 보이는지 확인하고, 측정법에 따른 LDL-C 치료 대상의 차이를 보았다. 위험인자 결정기준과 치료 대상 결정은 현재 국민건강보헙급여 적용 기준에 반영된 NCEP ATP III 을 따라 결정하였다.8)
방 법
1. 연구대상
2014년 1월 1일부터 2015년 12월 31일까지 서울시 소재 일개의 종합 병원 건강검진센터에 내원하여 종합건강검진을 받은 45세 이상의 남성과 55세 이상의 여성 중 HDL-C가 40 mg/dL 이하인 사람을 대상 으로 하였다. 전체 329건의 자료 중에서, 계산치에 오류값을 가질 수 있는 혈중 TG 수치 400 mg/dL 이상인 자료 12건을 제외하였다. 이상 지질혈증을 진단받고 약물을 복용 중인 자료 15건을 제외하였으며, 관상동맥질환이 있거나 당뇨병을 가지고 있는 자료 62건을 제외하 여, 최종적으로 240건의 자료를 대상으로 연구하였다. 본 연구는 성 애병원 임상시험심사위원회/기관생명윤리위원회에서 IRB 승인(IRB No. SA2015-18) 받은 연구이다.
2. 연구방법
종합건강검진시에 조사대상자의 기본 정보인 연령, 성별을 파악 하였으며, 자가설문방식을 이용하여 조사대상자의 흡연 상태, 질환 력(이상지질혈증, 관상동맥질환, 고혈압, 당뇨)을 파악하였다. 흡연 상 태는 검진 시점에 흡연 여부에 따라 흡연자와 비흡연자로 나누었다.
혈액검사는 최소 8시간 이상 금식 후 채혈하였으며, TC, HDL,
LDL-C, TG를 Hitachi-7180 (Hitachi, Tokyo, Japan)을 사용하여 측정 하였다. 각 항목은 wako 시약(Wako Pure Chemical Industries Ltd., Osaka, Japan)을 사용하여 효소법으로 측정하였다. LDL-C의 계산치 는 Friedewald 공식(TC=HDL-C+LDL-C+TG/5)을 이용하여 계산하였 다.
3. 통계 분석
조사대상자의 일반적 특성을 알아보기 위하여 범주형 변수에 대 해서는 빈도분석을 실시하였고 연속형 변수에 대해서는 기술통계 를 실시하였다. 조사대상자의 측정 LDL-C와 계산 LDL-C 간의 차이 를 비교하기 위하여 대응표본 t-test를 실시하였다. 최종적으로 측정 값과 계산값에 따라 치료 대상자의 변화를 알아보기 위해 교차분 석 내 상관표본의 비율 변화를 비교 측정하는 McNemar test를 실시 하였다. 본 연구에서 사용한 분석은 모두 유의수준 0.05를 기준으로 유의성을 평가하였으며, 통계 분석은 IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA)을 이용하였다.
결 과
1. 조사대상자의 일반적인 특성
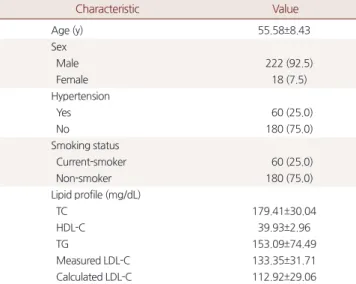
Table 1은 조사대상자의 일반적인 특성을 나타낸 것이다. 조사대 상자의 특성을 살펴보면 전체 집단의 평균 연령은 55.58세였다. 성별 은 남성이 222명(92.5%)으로 여성 18명(7.5%)에 비해 많았다. 고혈압
Table 1. General characteristics of study subjects
Characteristic Value
Age (y) 55.58±8.43
Sex
Male 222 (92.5)
Female 18 (7.5)
Hypertension
Yes 60 (25.0)
No 180 (75.0)
Smoking status
Current-smoker 60 (25.0)
Non-smoker 180 (75.0)
Lipid profile (mg/dL)
TC 179.41±30.04
HDL-C 39.93±2.96
TG 153.09±74.49
Measured LDL-C 133.35±31.71
Calculated LDL-C 112.92±29.06
Values are presented as mean±standard deviation or number (%).
TC, total cholesterol; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; Measured LDL-C, directly measured LDL-C levels;
Calculated LDL-C, estimated LDL-C levels calculated from Friedewald formula;
TG, triglyceride.
Jee Hye Kang, et al. Difference Direct and Calculated Measurement of Low Density Lipoprotein Cholesterol
Korean Journal of Family Practice
KJFP
유병자는 60명(25.0%)이고, 현재 흡연자는 60명(25.0%)이었다. 조사대 상자의 TC, TG, HDL-C, 계산 LDL-C, 측정 LDL-C 수치 평균은 각각 179.41 mg/dL, 39.93 mg/dL, 112.92 mg/dL, 133.35 mg/dL였다.
2. Measured LDL와 Calculated LDL 비교
Table 2는 조사대상자의 측정 LDL-C와 계산 LDL-C의 차이를 살 펴보기 위해 대응표본 t-test를 실시한 표이다. 측정 LDL-C는 평균±
표준편차는 133.35±31.71 mg/dL으로 계산 LDL-C 112.92±29.06 mg/dL 에 비해 높았으며, 통계적으로 유의하였다. 측정 LDL-C와 계산 LDL-C의 평균 차이±표준편차는 20.43±10.62 mg/dL였다.
3. LDL 결정 방식에 따른 관리대상의 변화
Table 3은 측정 LDL-C와 계산 LDL-C의 기준 수치에 따른 비율 변 화를 보기 위하여 McNemar test를 실시한 표이다. LDL-C 치료 시작 기준 수치인 130 mg/dL를 기준으로 비교한 결과, 측정 LDL-C 130 mg/
dL 이상인 127명 중 59명(46.5%)이 계산 LDL-C 130 mg/dL 미만에 속 하는 것으로 나타나 측정값과 계산값의 기준 수치에 따른 비율의 차 이가 있었다.
고 찰
이 연구에서는 HDL-C가 40 mg/dL 이하인 45세 이상 남성과 55세 이상 여성, 즉 관상동맥질환 위험인자 두 개 이상을 가진 성인을 대 상으로 LDL-C의 측정값과 계산값의 차이를 비교하고 측정값과 계
산값에 따라 치료 대상 여부가 변화하는지 알아보고자 하였다.
결과적으로 같은 검사 대상자에서 LDL-C의 측정값이 계산값에 비해 유의하게 높게 나타났다. 또한 치료 대상 여부의 변화에서도 측 정값으로는 130 mg/dL 이상이나 계산값으로는 130 mg/dL 이하인 대 상자가 59명(46.5%)으로 나타나, 계산값으로 치료 대상을 정할 경우 치료 대상자가 약 50% 정도 적게 설정되었다.
LDL-C는 관상동맥질환의 위험요인에 해당할 뿐 아니라 치료 목 표로도 제시된다. 이러한 중요도 때문에 정확한 LDL-C의 측정이 강 조되었고 직접 측정값과 Friedewald 공식에 의한 계산값의 차이에 대 해 많은 연구가 시행되었다. Lindsey 등9)이 시행한 연구에서 계산법 이 직접 측정값에 비해 평균 20 mg/dL 낮게 측정됨을 보였고 McNa- mara 등10)은 TG가 높을수록 직접측정법과 Friedewald 계산법의 일 치율이 낮아져 Friedewald 공식의 정확성이 감소함을 보였다. Schar- nagl 등11)은 LDL-C이 낮을수록 직접측정값에 비해 Friedewald 공식 을 사용한 계산값이 낮게 측정되는 오차가 있다고 하였다. Min 등12) 이 시행한 연구에서는 TG, LDL-C, TC 농도가 직접측정값과 계산값 의 오차에 영향을 준다고 하였다. Kim 등13)은 흡연군에서 LDL 콜레 스테롤의 실측값과 계산값에 따라 치료 대상자의 수에 유의한 차이 가 있음을 보였다. 그러나 실측값과 계산값에 따라 치료 대상 차이 를 보았던 이전의 연구는 ATP III guideline에서 관상동맥질환 고위 험군으로 분류된 군들만을 대상으로 하거나,9) 남성에서 흡연 상태 에 따른 치료 대상 변화를 비교하였다.13) 따라서 본 연구에서는 관상 동맥질환 위험인자 두 개 이상을 가진 성인에서 치료 대상자의 변화 여부를 확인하였고, 남성과 여성을 모두 포함하여 진행하였다. 또한 가족력을 잘 모르거나, 흡연력을 속이는 경우 또는 의료기관을 방문 한 적이 없어 진단되지 않은 고혈압을 가진 경우에서는 관상동맥질 환 위험인자의 파악이 정확하지 않을 수 있으므로, 비교적 객관적인 두 가지 항목, HDL-C 값과 나이를 기준으로 위험인자를 설정하였다.
계산법의 부정확성 때문에 직접측정법의 사용이 증가하고는 있 으나 아직 우리나라 건강보험공단에서의 건강검진은 계산법을 사 용하고 있어 적절한 치료 대상자가 배제될 수 있다. 순환기계 질환의 Table 2. Comparison of calculated LDL-C and measured LDL-C
Measured LDL-C
Calculated
LDL-C mLDL-cLDL P-value*
Total (mg/dL) 133.35±31.71 112.92±29.06 20.43±10.62 <0.05 Values are presented as mean±standard deviation.
LDL-C, low density lipoprotein cholesterol; Measured LDL-C, directly measured LDL-C levels; Calculated LDL-C, estimated LDL-C levels calculated from Friede- wald formula; mLDL, Measured LDL-C; cLDL, Calculated LDL-C.
*P-value, paired-sample t-test.
Table 3. Number of subjects deem to need management according to the method of LDL-C determination Calculated LDL-C (mg/dL)
Total P-value*
<130 ≥130
Measured LDL-C (mg/dL) <130 112 (99.1) 1 (0.9) 113 (100.0) <0.05
≥130 59 (46.5) 68 (53.5) 127 (100.0)
Total 171 (71.3) 69 (28.7) 240 (100.0)
Values are presented as number (%).
LDL-C, low density lipoprotein cholesterol; Measured LDL-C, directly measured LDL-C levels; Calculated LDL-C, estimated LDL-C levels calculated from Friedewald formu- la.
*P-value, McNemar test.
강지혜 외. 저밀도 지단백 콜레스테롤의 실측값과 계산값에 따른 비교 Korean Journal of Family Practice
KJFP
높은 유병률과 사망률로 인해 이를 예방하기 위한 관리가 강조되고 있다. 2013년 발표된 American College of Cardiology/American Heart Association (ACC/AHA) cholesterol guideline에서는 동맥경화성 심혈 관질환 예방을 위해 더욱더 적극적이 cholesterol 관리가 필요함을 강 조했다.14) 우리나라에서도 2015년 2009년 개정된 ATP III guideline, 2013년 발표된 ACC/AHA guideline을 반영하여 고위험군에서 기존 의 심혈관 질환이 있는 환자를 초고위험군으로 분류하여 LDL-C의 치료 기준을 70 mg/dL로 하는 등 예전보다 강화된 이상지질혈증 치 료 지침이 발표되었다.15)
본 연구는 몇 가지 제한점을 가진다. 첫째 일개 병원에서 시행한 건강검진 수검자만을 대상으로 하여 일반 인구의 특성을 대변하지 못할 수 있다. 둘째 흡연 여부를 분류함에 있어 과거 흡연자와 비흡 연자를 모두 비흡연자로 분류하였다. 셋째 계산식에 영향을 미칠 수 있는 다른 요인들 간질환, 만성 신장질환, 혈청내 아포지단백이 높은 경우를 고려하지 못하였다.
이러한 제한점에도 불구하고, 이 연구를 통해 관상동맥질환 위험 인자 두 개 이상을 가진 성인에서 LDL-C 측정값에 비해 계산값에서 치료 대상자가 적게 설정되는 것을 보았다. 관상동맥질환 위험인자 를 가지고 있는 경우에는 보다 적극적인 관리가 필요하나, 우리나라 건강검진에서 사용하고 있는 Friedewald 공식을 이용한 치료 대상자 분류에서는 정확한 환자 분류가 이루어지지 않을 수 있다. 적절한 LDL-C의 관리는 관상동맥질환의 발생 위험을 직접적으로 감소시 킬 수 있으므로 관상동맥질환을 보다 정확하게 예방 관리하기 위해 직접측정법으로 LDL-C를 측정하는 것이 필요하다고 생각한다.
요 약
연구배경:
순환기계 질환의 높은 사망률 때문에 이를 줄이기 위한 많은 노력이 기울여지고 있다. 그중 주요 위험인자로 알려진 저밀도 지단백 콜레스테롤은 위험 요인일 뿐 아니라 치료 목표로도 제시되 고 있다. 이에 저밀도 지단백 콜레스테롤 측정법 중 계산법과 직접측 정법과의 비교를 통해 치료 대상의 변화를 알아보고자 하였다.방법:
2014년부터 2015년 2년 동안 한 종합병원에서 건강검진을 받 은 고밀도 지단백 콜레스테롤이 40 mg/dL 이하인 45세 이상 남성과 55세 이상 여성을 대상으로 연구하였다. 자가설문방식과 문진을 통 해서 가족력과 질환력 등을 파악하였고, 균질법을 사용한 저밀도 지단백 콜레스테롤의 직접측정치와 Friedewald 공식을 사용한 계산 치를 비교하였다.결과:
45세 이상 남성 55세 이상 여성 두 군 모두 저밀도 지단백 콜레 스테롤의 측정치와 계산치가 유의한 차이를 보였으며 이를 토대로한 치료 대상자 선정에서도 큰 차이를 보였다.
결론:
관상동맥질환 위험인자를 가진 사람에게서 저밀도 지단백 콜레스테롤 치료 대상자 선정과 치료 적정성 평가 등을 위해 측정치 를 사용하는 것이 계산치를 사용하는 것보다 도움이 될 것이다.중심단어:
저밀도 지단백 콜레스테롤; 관상동맥질환 위험인자;Friedewald 공식; 직접 측정법
REFERENCES
1. Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention. Korea Health Statistics 2014: Korea National Health and Nutri- tion Examination Survey (KNHANES VI-2). Cheongju: Korea Centers for Disease Control and Prevention; 2015.
2. Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circu- lation 1998; 97: 1837-47.
3. Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, MacFarlane PW, et al.
Prevention of coronary heart disease with pravastatin in men with hyper- cholesterolemia. N Engl J Med 1995; 333: 1301-7.
4. Stamler J, Wentworth D, Neaton JD. Is relationship between serum choles- terol and risk of premature death from coronary heart disease continuous and graded? Findings in 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 1986; 256: 2823-8.
5. National Cholesterol Education Program (NCEP) Expert Panel on Detec- tion, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report.
Circulation 2002; 106: 3143-421.
6. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the prepara- tive ultracentrifuge. Clin Chem 1972; 18: 499-502.
7. Bae JM. Comparison of direct measurement of homogeneous assay and friedewald formula on low-density lipoprotein cholesterol measurement [dissertation]. Daejeon: Chungnam National Univ.; 2005. Korean.
8. Nauck M, Warnick GR, Rifai N. Methods for measurement of LDL-choles- terol: a critical assessment of direct measurement by homogeneous assays versus calculation. Clin Chem 2002; 48: 236-54.
9. Lindsey CC, Graham MR, Johnston TP, Kiroff CG, Freshley A. A clinical comparison of calculated versus direct measurement of low-density lipo- protein cholesterol level. Pharmacotherapy 2004: 24: 167-72.
10. McNamara JR, Cohn JS, Wilson PW, Schaefer EJ. Calculated values for low- density lipoprotein cholesterol in the assessment of lipid abnormalities and coronary disease risk. Clin Chem 1990; 36: 36-42.
11. Scharnagl H, Nauck M, Wieland H, März W. The Friedewald formula un- derestimates LDL cholesterol at low concentrations. Clin Chem Lab Med 2001; 39: 426-31.
12. Min WK, Park HI, Jun KR, Chun S, Lee W. Factors affecting the difference between the low-density lipoprotein cholesterol concentrations measured
Jee Hye Kang, et al. Difference Direct and Calculated Measurement of Low Density Lipoprotein Cholesterol
Korean Journal of Family Practice
KJFP
directly and calculated using the friedewald formula. J Lab Med Qual Assur 2008; 30: 233-5.
13. Kim SW, Lee JH, Cho JB, Lee JW, Lee JW, Park JM, et al. The change in thera- peutic targets of dyslipidemia: a difference between estimated and direct measured method getting low-density lipoprotein cholesterol of male pa- tients over 45 years old smokers and nonsmokers. Korean J Fam Pract 2015;
5(suppl 3): S140-4.
14. Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel
RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the Amer- ican College of Cardiology/American Heart Association task force on prac- tice guidelines. Circulation 2014; 129(25 Suppl 2): S1-45.
15. Korean Society of Lipidology and Atherosclerosis. Guidelines for manage- ment of dyslipidemia. 3rd ed. Seoul: Korean Society of Lipidology and Ath- erosclerosis; 2015.