책임저자:윤병민, 제주도 제주시 제주대학로 66
690-756, 제주대학교 의과대학 성형외과학교실 Tel: 064-717-1742, Fax: 064-755-6130
E-mail: [email protected]
둔부 천공지를 보존하는 둔부 근막피부 회전전진 피판술과 V-Y 봉합술
윤 병 민
제주대학교 의과대학 성형외과학교실
The Gluteal Artery Perforator Sparing Gluteal Fa- sciocutaneous Rotation Advancement Flap with V-Y Closure
Byung Min Yun, M.D.
Department of Plastic and Reconstructive Surgery, College of Medi- cine, Jeju National University, Jeju, Korea
Purpose: The management of gluteal wound originated with burn is same as pressure sore. Pressure sores are managed surgically with two therapeutic components. One is a gross and sharp debridement and the other is a flap providing well-vascularized tissue to cover wounds. Central to the flap considerations is the tendency for recurrence mainly due to a poor blood supply, failure of tension-free closure and naive nursing care after operation, when reconstructive surgeons employ numerous surgical techniques in sores repair. The author used the gluteal artery perforator sparing and gluteal fasciocutaneous rotation advancement flap with V-Y closure to manage gluteal wound originated from burn.
Methods: Three cases of gluteal wound were treated with the gluteal artery perforator sparing gluteal fasciocutaneous rota- tion advancement flap with V-Y closure. The skin incision of conventional gluteal rotation flap is shortened to get a mini- mized flap size and adapts an advancement flap in a back cut pattern, supported laterally with V-Y closure for a tension-free closure. This superiorly (or inferiorly) based flap is elevated subfascially until one or two large musculocutaneous perfo- rators of the inferior gluteal artery are encountered. The per- forator down to its emergent point at the level of the piriformis muscle is dissected intramuscularly by splitting fibers of the gluteus maximus muscle in order to pivot freely. Then, the dead space is obliterated with a portion of the gluteus muscle transposed independently. The skin paddle is rotated to the defect area with the saved perforator(s) and closed the de- fect area.
Results: This technique encompasses the advantages of a perforator sparing flap, a fasciocutaneous rotation flap and
an advancement flap with V-Y closure, providing a better vas- cularity, the flexibility of rerotation in the event of recurrence, preservation of the gluteus maximus muscle for ambulatory function, tension-free mobilization. Compared with other flaps which are previously used to manage pressure sores, one advantage is noted that the minimized operation wound is ef- fective not only to improve the quality of patient's life in terms of position care but also to mitigate the associated wound- healing problems.
Conclusion: This technique can be chosen primarily for man- agement of various types of gluteal region wound including burn. (Journal of Korean Burn Society 2009;12:125-130) Key Words: Burn, Gluteal region, Gluteal artery perforator
sparing flap
서 론
화상은 창상(wound)의 한 종류로, 그 중 화상으로 인해
둔부에 피부이식 이외의 수술적 치료를 요하는 경우는 흔
하지는 않지만 이따금 발생된다. 이와 같은 화상이 원인이
된 둔부 창상의 치료 원칙은 일반적인 욕창의 치료에 준하
기 때문에 본 저자는 화상이 원인이 되어 둔부에 발생한
창상을 성공적으로 치료한 경험이 있기 때문에 욕창의 일
반적인 고려 점과 함께 둔부의 창상 치료 방법을 소개하고
자 한다. 욕창(pressure sore)은 신체 일부분에 지속적으로
가해지는 압력으로 조직에 순환 장애가 발생될 때 특히 뼈
가 튀어나온 부위에서 잘 생기며, 마비환자, 장기간 병상에
누워있는 환자와 노인들에게서 호발 한다. 최근의 보고에
의하면 미국에 매년 욕창 환자가 500,000명 정도 발생하며,
이에 따른 치료비용은 15억 달러에 이른다고 한다
1). 욕창을
수술적으로 치료하기 위하여 다양한 방법들이 시도되었으
나 재발률이 높아서 재건의사들에게 여전히 도전의 대상이
되고 있다. 본 저자의 천공지(perforator)를 보존하는 피판
술은 근막피부피판술, 회전피판술, 그리고 V-Y 전진피판술
각각의 장점들을 벤치마킹한 것으로 향상된 혈행의 유지,
재발 시에도 피판의 재사용이 가능하며, 둔부 근육 보존으
로 보행 기능이 유지되는 등의 장점이 있다.
Table 1. Summary of Clinical Cases
Number Age (YR)/Sex Cause Sore Perforator Result
1 72/F Infected contact burn Sacral sore Superior gluteal artery Good
2 42/M Contact burn Sacral sore Superior gluteal artery Good
3 65/M Scalding burn Ischial sore Inferior gluteal artery Good (1st revision)
YR = years, M = male, F = female
Fig. 1. Schematic illustration of the gluteal artery perforators sparing gluteal fasciocutaneous rotation advancement flap with V-Y closure. (A) Anatomy of gluteal area. (B) Coverage of sacral area using the flap contains the superior gluteal artery perforator. (C) Coverage of ischial area using the flap contains the inferior gluteal artery perforator.
Fig. 2. Schematic illustration of the flap design. It combines the modified conventional rotation flap with perforator-sparing rotation flap and rotation-advancement flap with V-Y closure.
대상 및 방법
1. 대상
2007년 1월부터 2009년 9월까지 저자가 수술을 한 3명의 환자를 대상으로 하였다. 둔부 화상의 원인은 첫 번째 환자 의 경우 허리 통증으로 인해 무자격자에게 시술받은 뜸이 원 인이 되어 염증으로 인해 발생하였고, 두 번째 환자의 경우 는 정신과 약물을 복용하는 환자로 음주 후 온돌방에서 자 다가 발생한 접촉성화상(contact burn)이 원인이고, 세 번째 환자의 경우는 하지마비 환자로 관리소홀로 인한 핫팩이 원인이 된 경우였다. 평균 나이는 60세였고, 남자 2명, 여자 1명이었고, 부위는 천골(sacrum)이 2곳, 좌골(ischium)이 1 곳이었다. 모든 환자는 Daniels 등
2)의 욕창 분류상 뼈의 일 부분까지 침범된 Grade 5였다. 수술 후 평균 외래 추적 관 찰기간은 9개월이었다(Table 1).
2. 수술방법
둔부동맥은 상행지 둔부동맥(superior gluteal artery)과
하행지 둔부동맥(inferior gluteal artery)으로 나뉘며 본 방
법은 두 동맥에 모두 적용 시킬 수 있다(Fig. 1). 중복을 피
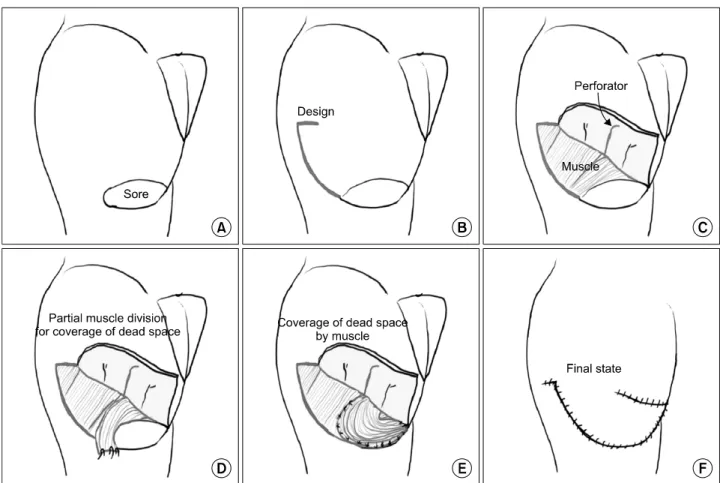
Fig. 3. Schematic illustration of the operation technique of the perforator-sparing and rotation-advancement flap with V-Y closure in the management of an ischial pressure sore. (A) Ischial pressure sore. (B) Design. (C) A superiorly based gluteal fasciocutaneous flap is caudally elevated until the inferior gluteal perforator is reached. Then, the inferior gluteal perforator is dissected intramuscularly to its exit point below the piriformis muscle in order to pivot freely with the flap rotation. (D, E) The dead space is obliterated with a portion of the gluteus maximus muscle partially devised and transposed. (F) Closure.
하기 위해 우선 하행지 둔부동맥을 이용한 방법을 먼저 소 개하고 이어서 상행지 동맥을 이용하는 방법에 대해서 기 술하겠다. 우선 포터블 도플러를 사용하여 천공지의 위치 를 확인한 뒤 욕창의 위치에 따라 필요한 피부패들(skin paddle)을 디자인 한다. 좌골창상의 경우 도플러로 확인한 하 행둔부동맥천공지를 포함하는 상부를 기반(superiorly based) 으로 한 근막피부피판으로 디자인한다. 피판의 아래쪽 절개 선은 전통적인 회전피판(conventional rotation flap)처럼 디자인하며, 그 길이가 대퇴골 대전자 언저리까지로 한정 되게 변형시키고, 피판의 위쪽 절개선은 V-Y 전진 피판이 가능하도록 타원(elliptical)형으로 짧게 넣는다(Fig. 2). 욕창 부위는 변연절제하고, 활액낭(bursa)을 제거하며 노출된 불 규칙한 좌골 면을 평평하게 갈아낸 후 식염수로 압력 세척 (pressure irrigation)한다. 근막아래(subfascia) 깊이까지 피 부를 절개하고 근막아래 즉, 근육위에서 근육과 근막아래 의 공간을 따라서 수술 전에 표시한 천공지가 나타날 때까
지 피판을 거상해 올리면서 박리를 시행하고 둔부근육에 묻혀있는 천공지를 당김 없이 자유롭게 이동할 수 있도록 근섬유 방향에 맞추어 박리한다. 보존할 천공지의 개수는 보존하는 천공지가 많으면 피판 이동에 방해가 되기 때문 에 하나 혹은 두 개 정도가 적당하다. 천공지 피판과 관련된 작업은 루뻬와 헤드램프를 착용하고 시행한다. 이어서 정 리된 창상의 사강(dead space)은 거상된 피판의 근육층 일 부를 박리한 후 회전시켜 덮어주고 굵은 드레인을 1개 삽입 한다. 끝으로 준비된 하행둔부동맥천공지를 포함하고 있는 근막피부피판이 창상부위로 이동할 때 장력이 걸리지 않는 것이 확인되면 덮은 후 피부제공부를 V-Y 봉합으로 일차 봉합한다. 혹 피판에 장력이 걸리는 경우는 피판의 위쪽 절 개선 길이를 연장시킬 수 있다(Fig. 3, 4).
이상이 하행둔부동맥을 이용하는 방법이며, 상행둔부동
맥을 이용하는 부위는 천골(sacrum)부위로 하행둔부동맥을
이용하는 피판과의 기본적인 차이점은 피부피판이 하부에
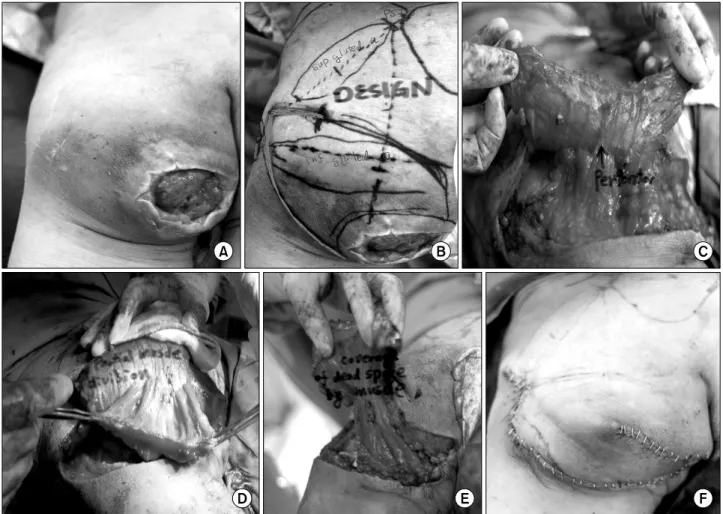
Fig. 4. Clinical application of the operation technique of the perforator-sparing and rotation-advancement flap with V-Y closure in the management of an ischial pressure sore of clinical case 3. (A) Ischial pressure sore. (B) Design. (C) A superiorly based gluteal fasciocutaneous flap is caudally elevated and the inferior gluteal perforator is dissected intramuscularly. (D, E) A portion of the gluteus maximus muscle partially devised and transposed for dead space obliteration. (F) Closure.
기저(inferiorly based)를 두는 것이며 그 이외에는 위에서 기술한 방법과 동일하다(Fig. 1).
결 과
평균 수술시간은 3시간가량 소요되었으며, 수술전후 헤 모글로빈의 변화는 1 g/dl으로서 수술 중 실혈 량은 많지 않았다. 세 번째 환자는 수술 후 임의로 1주 만에 휠체어를 타다가 봉합 부위가 벌어졌으나, 벌어진 부위는 피판의 피 부색과 회전전진 정도가 모두 양호하였기 때문에 추가적 박리 없이 일차 봉합을 할 수 있었고 이후 창상의 문제가 발생하지 않았으며, 나머지 2명의 환자는 현재까지 재발없 이 좋은 결과를 보였다(Fig. 5, 6).
고 찰
앞에서 언급한 것처럼 화상이 원인이 된 둔부 창상의 치
료 원칙은 일반적인 욕창의 치료에 준하기 때문에 욕창의
일반적인 고려 사항부터 알아보겠다. 호발하는 욕창부위로
는 천골(sacrum), 대전자부(greater trochanter), 그리고 좌
골(ischium)이며 욕창의 수술적 관리는 1938년 Davis 등
3)이 처음으로 소개한 것처럼 죽은 조직의 제거 및 건강한
피판의 활용을 기본으로 한다. 과거 한동안은 근육피부피판
(myocutaneous flap)이 혈행이 풍부할 뿐만 아니라 부피감
있는 이동으로 결손 공간을 채울 수 있기 때문에 가장 우수
한 피판이라고 생각되어왔다. 하지만 둔부 근육을 사용했
기 때문에 보행기능이 유지되어야 하는 환자의 경우에는
제한이 있었다. 이에 1988년 Kroll 등
4)은 근육을 포함하지
않고 천공지에 의존하는 근막피판을 사용하여 좋은 결과를
Fig. 5. Photographs of clinical case 1. (A) Design of flap: superior gluteal artery based flap. (B) Postoperative state.
Fig. 6. Photographs of clinical case 2. (A) Design of flap: superior gluteal artery based flap. (B) Postoperative state.
보고하면서 근육보다 근막과 피부가 압력에 대한 저항에 있어서 더 우수하다고 하였고, 1993년 Koshima 등
5)은 천공 지 의존 근막피판술을 둔부 욕창에 적용시킴으로써 보행기 능을 유지시키기까지 둔부 욕창치료에 있어서 발전을 거듭 해왔다. 하지만 천공지 피판은 도서형 피부피판(island skin flap)이기 때문에 수술의 실패 혹은 욕창의 재발 시 피판의 재이용이 불가능하다. 보고에 의하면 총 66건의 욕창을 평 균 9.3개월 동안 추적 관찰한 결과 61%에서 재발하였으며
6), 좀 더 최근에는 수술과 재활치료를 병행한 총 268건의 욕창 을 평균 3.7년 추적 관찰하였더니 19%에서 재발하였다고 보고된 바 있다
7). 그러므로 욕창 수술에 있어서 반드시 염 두에 두어야 할 것이 재발 시의 수술계획이다. 이런 이유로 Wong 등
8)은 피판의 박리 정도를 부분(partial)으로 제한하 여 혈행을 유지시키고 피부패들이 가능한 한 넓어서 욕창 재발 시 이 피판을 다시 사용 할 수 있도록 하는 근육피부 혹은 근막피부회전피판(rotation flap)이 둔부 욕창수술의 기본이라고 하였다. 그러나 부분 박리로 피판을 이동(회전)
시키는 데에는 한계가 있어 크고 깊은 욕창을 덮고자 피판 을 멀리 이동시켜야 하는 경우에는 완전 박리의 수준으로 박리를 하게 되는데 이렇게 되면 피판의 혈행 유지가 그만 큼 더 어려워진다. 이에 대하여 2007년 Wong 등
8)은 기존의 근막피부 회전 피판(rotation flap)을 완전 박리 하면서 둔부 천공지를 보존하도록 하는 변형 술을 선보였다. 여기에서 저자는 Wong 등
8)의 피판술기로부터 한 걸음 더 나아가 피 판의 절개부를 최소화하고 피판 끝의 장력을 줄이고자 피 판의 모서리를 백컷(back cut)형태로 만들어 주어 회전피판 과 전진피판의 기능을 동시에 발휘하도록 하고 피판의 공 여부를 V-Y 봉합으로 일차 봉합하였다(Fig. 2). 일반적으로 욕창 환자에게는 최소 3주 동안 수술 부위에 체중부하 없는 자세 유지와 용변시 창상 오염에 대한 각별한 주의를 요한 다. 따라서 현격히 축소된 수술부위는 환자의 삶의 질 면에 서와 치료결과 면에서 효과가 있을 것으로 기대할 수 있다.
한편, 둔부의 천공지는 상행지 둔부 동맥과 하행지 둔부 동
맥이 있으며, 그 수는 각각 5 (±2)개, 8 (±4)개이고, 천공지의
Table 2. Comparative Characteristics of Rotation Fasciocutaneous, Island-Type Perforator, Perforator-Sparing, and Perfora- tor-Sparing & Rotation-Advancement Flap with V-Y Closure for Coverage of Gluteal Pressure Sores
Partially undermined rotation fasciocutaneous flap
(Standard flap)
Island-type perforator flap (Koshima et al. 1993)
Perforator-sparing rotation flap (Wong et al. 2007)
Perforator-sparing &
rotation-advancement flap with V-Y closure
(Author's flap) Length of surgical incision
Reusing the buttock flap in the event of ulcer recurrence The relative vascularity of the flaps
Blood supply
The tension at the distal end of the flaps
Action principle
Long Yes
Good
Random pattern
More
Rotation with the limited arc
Variable No
Good
Axial pattern
Less
Full mobilization
Long Yes
Better
Dual (Random and Axial pattern) Less
Rotation with a less limited arc
Short Yes
Better
Dual (Random and Axial pattern)
Far less
Rotation with a less limited arc and
Advancement supported laterally with V-Y closure
평균 내경(internal diameter)은 동일하게 0.6 (±1) mm이며, 피부지배 영역(cutaneous vascular territory)의 넓이는 각각 69 (±56) cm
2, 177 (±38) cm
2이다
9). 또한, Higgins 등
10)은 혈 관경 길이에 따라서 상행지둔부천공지는 대전자(trochanter) 나 천골(sacrum)부위의 재건에, 하행지둔부천공지는 좌골 부위 재건에 이용하는 것이 적당하다고 하였다.
결 론
화상에 의해 발생한 둔부의 창상 치료를 위하여 저자가 사용한 둔부천공지보존 근막피부 회전전진 피판술과 V-Y 봉합술의 장점은 다섯 가지로 요약될 수 있으며 이는 더 나아가 화상에 의한 경우 이외에도 둔부에 발생한 모든 종 류의 창상치료에 적용 할 수 있다고 저자는 생각한다. 첫째, 피판은 보존된 천공지 요소와 박리되지 않은 임의피판 요 소를 함께 갖고 있어서 이중 혈행 공급을 받게 된다. 둘째, 천공지 보존에 의해서 욕창 재발시 피판의 재사용이 가능 하다. 셋째, 둔부 근육을 보존하였기 때문에 보행기능에 지 장을 주지 않는다. 넷째, 회전피판이면서 전진피판이므로 피판에 장력이 걸리지 않아 피판이 괴사될 가능성이 적다.
마지막으로 중요한 것은 절개선을 최소화하였기 때문에 수 술 후 환자 자세를 유지하는 것과 상처 관리에 용이하다는 점이다(Table 2).
REFERENCES
1) Scheufler O, Farhadi J, Kovach S, Kukies S. Anatomical basis and clinical application of the infragluteal perforator flap.
Plast Reconstr Surg. 2006;118:1389-1340.
2) Daniels RK, Hall EJ, Macleod MK. Pressure sore: a reapprai- sal. Ann Plast Surg. 1979;3:53-57.
3) Davis JS. Operative treatment of scars following bed sores.
Surgery 1938;3:1.
4) Kroll SS, Rosenfield L. Perforator-based flaps for low po- sterior midline defects. Plast Reconstr Surg. 1988;81:56-566.
5) Koshima I, Moriguchi T, Soeda S, Kawata S. The gluteal perforator-based flap for repair of sacral pressure sores. Plast Reconstr Surg. 1993;91:678-683.
6) Disa J, Carlton JM, Goldberg NH. Efficacy of operative cure in pressure patients. Plastic Reconstr Surg. 1992;89:272-278.
7) Kierney PC, Engrav LH, Isik FF. Results of 268 pressure sores in 158 patients managed by plastic surgery and rehabilitation medicine. Plast Reconstr Surg. 1998;102:765-772.
8) Wong CH, Tan BKL, Song C. The perforator sparing buttock rotation flap for coverage of pressure sores. Plast Reconstr Surg. 2007;119:1259-1266.
9) Ahmadzadeh R, Bergeron L, Tang M., Morris S. The superior and inferior gluteal artery perforator flaps. Plast. Reconstr.
Surg. 2007;120:1551-1556.
10) Higgins JP, Orlando GS, Blondeel PN. Ischial pressure sore reconstruction using an inferior gluteal artery perforator flap.
Br J Plast Surg. 2002;55:83-85.