Korean Circulation Journal
Introduction
Despite rapid advancements in the therapeutic field of cardiovas- cular diseases, acute coronary syndromes (ACSs) are still the leading cause of morbidity and mortality worldwide. Increased numbers of coronary intensive care units, reperfusion techniques for percuta-
Original Article
http://dx.doi.org/10.4070/kcj.2013.43.7.462 Print ISSN 1738-5520 • On-line ISSN 1738-5555
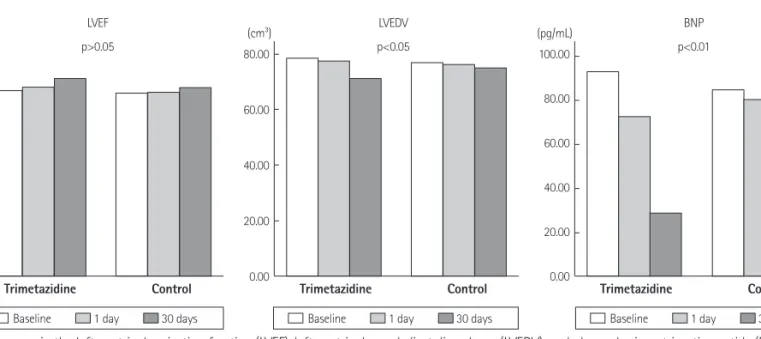
The Impact of Trimetazidine Treatment on Left Ventricular Functions and Plasma Brain Natriuretic Peptide Levels in Patients with
Non-ST Segment Elevation Myocardial Infarction Undergoing Percutaneous Coronary Intervention
Selami Demirelli, MD 1 , S¸ule Karakelleog˘lu, MD 2 , Fuat Gündog˘du, MD 2 , Muhammed Hakan Tas¸, MD 2 ,
Ahmet Kaya, MD 3 , Hakan Duman, MD 4 , Hüsnü Deg˘irmenci, MD 5 , Hikmet Hamur, MD 6 , and Ziya S¸ims¸ek, MD 2
1
Department of Cardiology, Erzurum Regional Training and Research Hospital, Erzurum,
2
Department of Cardiology, Faculty of Medicine, Atatürk University, Erzurum,
3
Department of Cardiology, Faculty of Medicine Ordu University, Ordu,
4
Department of Cardiology, Rize State Hospital, Rize,
5
Department of Cardiology, Erzurum Palandöken State Hospital, Erzurum,
6