J Korean Neurosurg Soc/Volume 29/August, 2000 1094
KISEP Case Reports J Korean Neurosurg Soc 29:::1094-1097, 2000 :
개두술후 발생한 뇌 아스퍼질루스증 2예
울산동강병원 신경외과
김정득·김의중·박상준·조창원·윤성문
= Abstract =
Two Cases of Cerebral Aspergillosis Following Cranial Operation
- --
- Case Report ----
Jung Dug Kim, M.D., Eui Jung Kim, M.D., Sang June Park, M.D., Chang Weon Cho, M.D., Sung Moon Youn, M.D.
Department of Neurosurgery, Dong Kang General Hospital, Ulsan, Korea
Aspergillosis is an opportunistic infection associated with diabetes, alcoholism, use of corticosteroid and transpl- antation procedure. Aspergillosis of central nervous system is a rare disease and known to show an aggressive cou- rse with high mortality. We managed two cases of cerebral aspergillosis, following cranial operation, with combination therapy of surgery and antifungal agents. One patient recorvered but the other patient died.
The clinical course of these two patients is presented with review of pertinent literature.
KEY WORDS:Cerebral aspergillosis・Combination theraphy.
서 론
뇌 신경계를 침범하는 진균성 질환은 cryptococcosis, no- rcardia, mucomycosis, candidiasis, aspergillosis 의 빈도 로 발생하며, 특히 침윤성 뇌 아스퍼질루스증(aspergillosis) 은 매우 드문 질환으로, 항진균 화학요법, 수술적 제거술에 도 불구하고 예후는 매우 불량하여 사망률은 95% 이상에 달한다4)5).
본 증례는 외상으로 인한 뇌혈종의 제거술후 발생한 뇌 아스퍼질루스증의 경우로, 감염의 원인, 진단, 치료방법, 예 후등에 대하여 문헌 고찰과 함께 보고 하고자 한다.
증 례
증 례 1:
66세의 남자 환자로 내원 당일 추락 사고로 인한 의식 변 화를 주소로 내원하여 뇌전산화단층촬영에서 좌측 전두엽-
측두엽-두정엽 부위에 급성 뇌경막하 혈종과 좌측 전두엽 에 외상성 다발성 뇌실질내 혈종 등을 발견하고, 경막하 혈 종에 대한 개두술 및 혈종 제거술을 시행 한 후 뇌실질내 혈종이 증가되어 혈종 제거술을 재차 시행하였다. 술후 환 자는 두개내압 항진 치료를 위한 만니톨 및 스테로이드 요법 을 시행하였다. 내원 20일째 뇌전산화단층촬영에서 좌측 전 두엽에 등음영의 낭종이 발견되어 뇌농양 의진하에 바늘 천 자 및 흡입을 시행하여, 흡입된 혈종 및 뇌 조직 파편의 병 리검사 및 배양검사를 시행하였으나 특별한 소견은 관찰되 지 않았다. 내원 34일째 추적 관찰한 뇌전산화단층촬영에서 테두리에 조영증강 소견이 있는 저 음영의 낭종이 관찰되어 서(Fig. 1 left), 뇌농양의 진단하에 좌측 전두엽 절제술 및 뇌농양 제거술을 시행하였고(Fig. 1 right), 조직학적 검사에 서 아스퍼질루스증을 확진후 amphotericin B를 1mg/kg으 로 80일간 투여하였다(Fig. 2). 수술 소견은 얇은 막으로 쌓여있는 낭성 농양이었으며 좌측 전두엽의 대부분이 농성 삼출물로 오염되어 있었다. 술후 환자는 뇌수두증이 발생되 어 뇌실–복강 단락술을 시행하였으며, 의식의 회복이 있어 의사 소통이 될 정도로 호전을 보였다. 단락술 시행전의 뇌
김정득 · 김의중 · 박상준 · 조창원 · 윤성문
J Korean Neurosurg Soc/Volume 29/August, 2000 1095
전산화단층촬영 추적검사에서 농양과 조영증강이 되던 부위 의 완전한 제거를 확인 하였고, 단락술 시행후 감염의 재발 은 없었다. 환자는 호전과 악화를 거듭 하면서 폐렴과 am- photericin B의 합병증인 신부전으로 사망하였다.
증 례 2:
15세의 남자 환자로 내원 당일 교통사고로 의식장애를 주소로 내원하여 응급검사에서 우측 소뇌 반구에 경막외 혈 종 및 뇌부종 소견 발견하고 개두술 및 혈종 제거술을 시행
하였다. 술후 환자는 두개내압 항진 치료를 위한 만니톨 및 스테로이드요법을 시행하였다. 술후 20일째 뇌전산화단층 촬영에서 양측 전두-측두부에 경막하 수액낭종(subdural hygroma)을 발견하고 천공술 및 배액술을 시행하였고, 술 후 점진적인 의식의 호전이 있어 의사소통이 가능하게 되었 다. 술후 50일째 뇌전산화단층촬영에서 수술부위의 경막에 인접하여 있고, 테두리의 조영이 증강된 주머니 형태의 이상 부위를 발견하고 뇌농양의 진단하에 제거술을 시행하였다 (Fig. 3). 수술 소견은 섬유질의 두터운 벽을 가진 육아종 (granuloma) 이였으며 소량의 농양물질을 포함하고 있었다.
조직학적 검사에서 아스퍼질루스증으로 확진 한 후 amph- otericin B를 1mg/kg과 하루 fluconazole 250mg 용량으로 일주일간 치료 후 경과를 관찰하였다(Fig. 4). 술 후 뇌전산 화단층촬영에서 조영증강이 되던 부위의 완전한 제거를 확 인하였고, 그후 검사실 및 이학적 검사에서 감염의 재발 소 견이 없었으며, 현재 건강한 상태로 정상적인 생활중이다.
고 찰
뇌신경계에 발생하는 진균성 질환은 cryptococcosis 55%, norcardia 15.4%, mucomycosis 7.1%, candidiasis 5.2%, aspergillosis 2.3%1)등의 빈도로 발생하고, 특히 아스퍼질
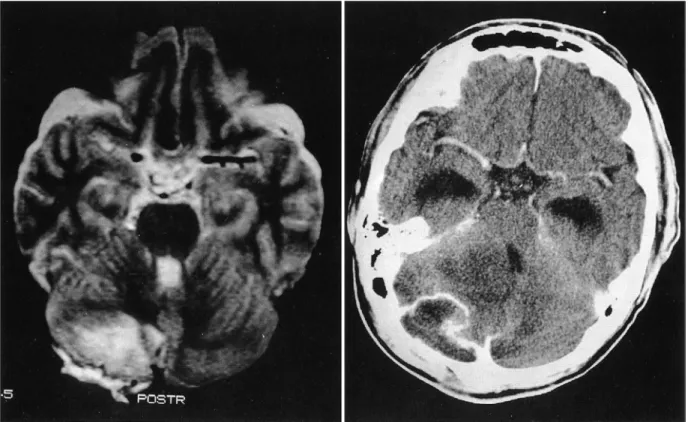
Fig. 1. Contrast enhanced brain CT scan on the 34th day after the hospital day showing enhancement of a cystic mass in the frontal area(left). Brain CT scan showing well evacuated state of the previous cystic mass(right).
Fig. 2. Fungal hyphae shows dichotomous branching and se- ptation(GMS stain, ×200).
개두술후 발생한 뇌 아스퍼질루스증 2예
J Korean Neurosurg Soc/Volume 29/August, 2000 1096
루스증은 정상적인 사람에서는 매우 드물게 발생하며, 대부 분 면역성이 저하된 환자에서 기회감염으로(opportunisitic infection)발생하는 질환으로 알려져 있다. 중추신경계를 침 범하는 아스퍼질루스증은 공기로 감염된 원발병소인 폐로 부터의 원격전이, 뇌 인접부위로 부터의 직접적인 전파, 드 물지만 신경외과적인 시술후 즉 개두술, 뇌척수액 배액술, 요추 천자술등을 시행한 후 직접 감염으로 전파될 수 있으
며1)4)6)7) 배액을 위한 도관(catheter)이 감염의 중요한 통로
역할을 한다고 지적하고 있다. 중추 신경계를 침범한 진균의
균사(hyphae)는 실질내 혈관을 침범하여1)4)5-7) 뇌경색, 뇌지 주막하 출혈, 뇌출혈등을 유발할 수 있고, 진균이 뇌실질로 직접 침투하며, 염증성 반응과 괴사를 유발시켜 뇌농양, 육아 종(granuloma), 뇌신경 마비등 다양한 양상을 보일 수 있다.
임상증상으로는 중추계를 침범한 진균증의 대부분이 아급성, 만성 경과의 신경학적 결손, 의식장애, 행동장애, 두통, 간질, 체온상승등의 증상을 보이는 반면, 아스퍼질루스증은 뇌수막 자극의 초기 증상이 없이 갑작스러운 신경학적 증상을 유발 하는 뇌졸중과 유사한 특징을 보이는 경우가 많다4)5).
진단법으로 뇌척수액 검사에서 특징적인 소견이 발견될 가 능성은 희박하며, 방사선학 검사에서는 뇌 아스퍼질루스가 뇌 기질과 뇌 혈관을 침범하여 철분과 칼슘이 침착되므로 뇌 자 기 공명 T2 영상에서 저신호 강도를 보이고 주위가 고신호 강도를 보이는 다발성의 병변으로 관찰되는 경우가 많으며, 뇌전산화단층촬영에서는 저음영의 공간 점유성 병변으로 나 타날 수 있고, 특히 뇌 아스퍼질루스가 대뇌 기저핵부위를 빈 번히 침범하므로, 대뇌 기저핵 부위에 초점성 병변이 빈번히
관찰1)2)4-7)10)된다고 보고하고 있으나 특징적인 소견은 아니
다1)2). 결국 수술시 채취한 조직의 병리학적 소견과, 배양검사 만이 아스퍼질루스증을 확진할 수 있는 유일한 방법이다1)4).
아스퍼질루스증의 치료는 수술적 적출술 후 항 진균제 투 여를 병행 하는데, 수술적 적출술은 조직학적 진단을 얻는
Fig. 3. Axial T2W1 MRI showing a lobulated cyst in the right cerebellum area(left). Contrast enhanced brain CT scan showing enhancement of a cystic mass(right).
Fig. 4. Granulomatous lesion showing necrotic changes, dich- otomous branching and septation(GMS stain, ×100).
김정득 · 김의중 · 박상준 · 조창원 · 윤성문
J Korean Neurosurg Soc/Volume 29/August, 2000 1097
데 중요한 역할을 하며, 수술 자체가 약물치료의 효과를 증
진시키며2)3)7-10) 또한 전적출이 가능한 경우 약물 투여기간
을 줄일 수 있고, 예후에 있어서도 큰 차이가 있으므로, 적 극적인 적출의 시도가 바람직하다. 수술적 적출술후 amp- hotericin B, itraconazole, flucytocin등 항진균제의 장기간 사용이 불가피 한데, 기존의 amphotericin B는 6주이상 계 속적으로 투약할 경우, 즉 체중이 70kg인 성인을 기준으로 총투여량이 5gm을 초과 할 경우부터 신경독성(neurotoxic) 증상을 나타 낼수 있고, 1mg/kg을 초과하여 사용할 경우 신독성(nephrotoxicity)을 유발 할수 있으므로2)7)8) 치료에 필요한 혈중 농도를 충분하게 유지할 수 없는 단점이 있었 으나, Coleman 등2)이 보고한 liposomal amphotericin B는 기존 약제용량의 15~30배 가량 고농도로 투여하여, 혈중 의 약물농도를 획기적으로 상승시키면서도, 약제의 부작용 인 신독성, 신경독성의 증상 없이 좋은 치료 효과를 얻었다 는 보고가 있어 주목 할 만 하다.
결 론
중추 신경계를 침범한 아스퍼질루스증은 진단적 방법에도 한계가 있고, 또한 면역성이 감소된 환자에서 주로 발생하므 로, 수술적 치료와 적절한 항진균제의 치료에도 불구하고 빈 번한 재발율을 보이므로 예후가 매우 불량하다. 결국 호흡기 를 통한 공기 감염으로 폐 질환이 발생 한 후 혈액으로 전파 가 주 감염원이므로 예방을 위한 주변 환경의 청결한 관리가 가장 중요하며, 뇌 아스퍼질루스증이 의심될 시는, 적극적인 수술적 절제로, 정확한 진단을 시행하고, 충분한 기간동안 항 진균제를 사용하는 것 만이 최선의 치료법이라 사료된다.
•논문접수일:2000년 2월 7일
•심사완료일:2000년 6월 14일
•책임저자:김 정 득
681-320 울산광역시 중구 태화동 123-3번지 울산동강병원 신경외과
전화:052) 241-1734, 전송:052) 244-9517 E-mail:[email protected]
References
1) Brown RS, Lake JR, Katzman BA, Ascher NL, Somberg KA, Emond JC, et al:Incidence and significance of aspergillus cultures following liver and kidney transplantation. Transpla- ntation 61:666-669, 1996
2) Coleman JM, Hogg GG, Rosenfeld JV, Waters KD:Invasive central nervous system aspergillosis:cure with liposomal amphotericin B, itraconazole, and radical surgery-case report and review of the literature. Neurosurg 36:858-863, 1995 3) Hagensee ME, Eric Bauwens J, Bowden RA:Brain abscess
following marrow transplantation:experience at the Fred Hutchinson Cancer Research Center 1984-1992 19:402-408, 1994
4) Hideki Satoh, Tohru Uozumi, Katsuzo Kiya, Fusao Ikawa, Kaoru Kurisu, Masayuki Sumida, et al:Invasive aspergilloma of the frontal base causing internal carotid artery occlusion.
Surg Neurol 44:483-488, 1995
5) Knaap MS, Valk J, Jansen GH, Kappelle LJ, Nieuwenhuizen O:Mycotic encephalitis:prediction for gray matter. Neuro- radiology 35:567-572, 1993
6) Matsuzono Y, Togashi T, Narita M, Taguchi Y, Miura S:Pul- monary aspergillosis and pseudosequestration of the lung in chronic granulomatous disease. Pediatr Radiol 25:201-203, 1995
7) Miaux Y, Rib P, Williams M, Guermazi A, Gluckman E, Bro- cheriou C, et al:MR of cerebral aspergillosis in patients who have had bone marrow transplantation. AJNR 16:555-562, 1995
8) Mott SH, Packer RJ, Vezina LG, Kapur S, Dinndorf PA, Conry JA, et al:Encephalopathy with parkinsonian features in chil- dren following bone marrow transplantations and high dose amphotericin B. Ann Neurol 37:810-814, 1995
9) Park JK, Jung S, Lee MC, Kang SS, Lee JH:Multiple brain abscess caused by aspergillus. J Korean Neurosurg Soc 24: 151-157, 1995
10) Robert E, Wiggins Jr:Invasive aspergillosis. J Neuroophtha- lmol 15:36-38, 1995