- 167 -
KISEP 대 한 두 경 부 종 양 학 회 지
제 22 권 제 2 호 2006
Extramedullary Plasmacytoma of the Sinonasal Cavity 1예
전남대학교 의과대학 이비인후과학교실
임 상 철·신 명 석
= Abstract =
A Case of Extramedullary Plasmacytoma of the Sinonasal Cavity
Sang-Chul Lim, M.D., Myung-Seok Shin, M.D.
Department of Otolaryngology, Chonnam National University Medical School, Gwangju, Korea
Extramedullary plasmacytoma is rare tumor of plasma cell tumor, which involve soft tissue without any signs of systemic spread and occurs predominantly in the head and neck, especially the nasal cavity and the paranasal sinuses. Ten to twenty percent of extramedullary plasmacytoma have regional lymph metastasis at the time of diagnosis and approximately one third of patients with extramedullary plasmacytoma will subse- quently develop multiple myeloma during long-term follow-up. Primary treatment modality is moderate-dose radiation and surgery is rarely used. Extramedullary plasmacytoma has good prognosis, but requires long-term systemic evaluation and follow-up. We report a case of extramedullary plasmacytoma of the sinonasal cavity with a review of literature.
KEY WORDS:Plasmacytoma·Nasal cavity·Paranasal sinuses.
서 론
Willis1)는 형질세포종을 다발성골수종, 골의 고립성형질 세포종, 골수외형질세포종으로 분류하였으며 골의 고립성 형질세포종과 골수외 형질세포종은 다발성골수종과 달리 전신침범이 없지만 치료 후에 다발성 골수종의 발생 가능 성으로 인해 지속적인 관찰이 필요하다. 골수외 형질세포종 은 대부분 두경부 특히, 비강과 부비동에서 발생하며2) 척 추나 두개골에 호발하는 골의 고립성형질세포종에 비해 다 발성골수종의 발생빈도가 더 낮다고 알려져 있다3). 저자들 은 비강과 사골동 및 상악동을 침범한 골수외 형질세포종 1예를 경험하였기에 보고하고자 한다.
증 례
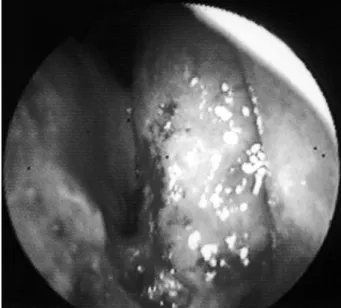
17세 남자가 수개월 전부터 지속되는 좌측 비출혈과 비폐
색을 주소로 내원하였다. 전신검사에서 특이소견은 관찰되 지 않았으며 이학적 검사에서 좌측 비강을 채우는 출혈하 는 종물이 관찰되었다(Fig. 1). 부비동 CT에서는 좌측 비 강, 사골동, 상악동을 침범하고 조영증강되는 6cm 크기의 팽창성 종물이 관찰되었으며(Fig. 2) 경부 CT에서 전이가 의심되는 경부 림프절은 관찰되지 않았다. MRI에서는 비강, 사골동, 상악동의 종물이 T1과 T2 강조영상에서 뇌와 동 일 신호 강도를 가지며 종물내에 신호가 소실된 병변들이 있으며 Gadolinium으로 조영증강한 T1 강조영상에서 강 하게 조영증강되었다(Fig. 3). 비강에서 시행한 조직검사는 고분화된 형질세포가 치밀하게 증식되어있으며 면역조직화 학염색에서 kappa 경쇄 및 IgG에 양성을 보여 골수외 형질 세포종으로 진단되었다. 전신침범을 알기 위해 시행한 혈액 검사, 골격 및 흉부 X-선 검사, 골주사, 복부초음파검사에 서 특이 소견이 관찰되지않았으며 혈청과 뇨단백의 전기영 동검사 및 골수 생검에서도 모두 정상소견을 보였다. 일차 적으로 방사선 치료를 시행하였으며 방사선치료 45Gy 조사 후 다시 시행한 CT에서 종물의 크기는 50%로 감소하고 비 강에만 종물이 관찰되었으나 추가적인 방사선 치료로서 완 전관해할 수 없다고 판단해 수술을 시행하였다. 내시경수술 교신저자:신명석, 501-757 광주광역시 동구 학동 8번지
전남대학교 의과대학 이비인후과학교실
전화:(062) 220-6773·전송:(062) 226-6369 E-mail:[email protected]
- 168 - 로 비강, 전사골동 및 상악동 내벽에 위치한 종물을 제거하 였으며 종물의 기시부위는 하비갑개, 상악골 전두돌기, 비골 내측이었다. 현재 치료 후 6년째 이비인후과 및 혈액종양내 과에서 추적관찰 중이며 재발 소견은 없는 상태이다.
고 찰
형질세포종은 골 또는 골수외에서 발생하는 종양이며 Lie-bross4)는 형질세포종양 1,354예 중 94%가 다발성골 수종, 4%가 골의 고립성형질세포종이며 골수외형질세포종 은 2%였다고 보고하였다. 고립성 형질세포종의 진단기준 은 조직학적으로 확진된 단일병변, 골격계는 정상이고, 골 수에 종양의 증거가 없을 때이다5)6). 척추나 두개골에 주로 발생하는 골의 고립성형질세포종과 달리 골수외형질세포종 의 호발 부위는 상기도인데 그 중 80%가 두경부에서 발생 하며 특히 비강 및 부비동, 비인두에서 흔하다고 알려져 있 으며 90%에서 다발성 병변, 10%는 단발성이다7). 남녀비 는 4:1이며 환자의 3/4는 40세에서 70세 사이라고 보고 된다7). 국내에서는 저자들의 증례를 포함하여 비강과 부비 동의 골수외형질세포종 11예8-15)가 발표되어있다(Table 1). 연령별로는 30대, 40대, 60대가 각 3명으로 가장 흔하 였고 남자 9예, 여자 2예로 남자에 주로 발생하였다.
증상은 일반적인 비강 또는 부비동의 종양과 유사하여 비 특이적이지만 종양으로 인한 폐색과 종창 등이 주증상이며
Fig. 1. Endoscopic view shows easily bleeding mass in the nasal cavity.
Fig. 2. Axial(A) and coronal(B) CT scans of the paranasal sinus. About 6 cm sized enhancing mass is located in the left nasal cavity, ethmoid sinus, and maxillary sinus and shifts septum to the right nasal cavity(A & B).
A B
Fig. 3. Axial sections of PNS MRI. Isointense mass in T1 weighted image(A) & T2 weighted image(B) occupy the left nasal cavity, ethmoid sinus, and maxillary sinus, which enhances strongly in contrast-enhanced T1 weighted image(C).
C B
A
- 169 - 비출혈과 비루 등이 나타날 수 있다. 10~20%에서 경부 림 프절 전이를 가지고 있다16-18).
골수외형질세포종의 방사선학적 소견은 비특이적이지만 전산화 단층촬영에서는 대개 균일하고 경계가 뚜렷한 종괴 로 나타나는데, 때로는 침윤성의 병변으로도 나타날 수 있 으며 다소 조영증강되는 종물로 관찰되며19) 저자들의 증례 도 유사한 소견을 보였다. 자기공명영상은 T1 강조 영상에 서는 저신호강도, T2 강조 영상에서는 고신호강도로 보이 며 조영증강이 된다고 한다19). 저자들의 증례는 이와 달리 T1과 T2 강조영상에서 동일신호강도를 보였다.
진단은 세침흡인생검으로 가능하다고 보고되고 있으나20) 골수외 형질세포종의 점막하 성장때문에 심부 생검, 개방 생 검 또는 부위에 따라서는 절제생검으로 조직학적 확진을 내 릴 수 있다고 한다2). 형질세포종은 조직학적으로 H&E 염 색에서 형질세포가 미세한 세망 간질내로 침윤하는 형태, 또 는 형질세포가 미세혈관으로 구성된 기질내에 판상으로 배 열되며 형질세포가 침윤되는 양상이 아니라 완전히 대치되 는 특징을 갖는다고 하며19) 다른 질환과 감별이 쉽지않아서 단클론성 kappa 또는 lamda 경쇄 또는 IgA, IgD, IgG, IgM 중쇄의 면역조직학적염색이 필요하다2). 저자들의 증례에서 는 kappa 중쇄와 IgG가 양성으로 염색되었다.
형질세포종이 조직학적으로 진단되면 전신침범을 배제하 기 위해 혈액검사, 혈청과 소변의 전기영동검사 및 면역단백 전기영동검사, 혈청 Ig의 정량분석, beta-2-microglobulin, 전신의 방사선학적 검사 및 골수흡인생검이 필요하다2).
치료는 형질세포종이 방사선감수성이 매우 높기 때문에 방 사선치료가 일차적인 치료 방법이며 흔히 40Gy 내지 50Gy 의 방사선조사가 추천되고있다21). 주로 방사선으로 치료한 고립성 형질세포종 258예를 대상으로 한 연구에서 골수외 형질세포종 52예(두경부 42예)의 10년 생존율 72%, 10년 무병생존율 55%, 10년 국소제어율 74%, 10년 다발성골수
종 발생율 36%라고 보고하고 있다22). 국소제어율은 80~
90%3)로 높은 것으로 알려져 있으나 저자들의 증례에서는 6cm 크기의 큰 종양으로 45Gy 방사선 치료로 완전관해 되 지않아 구제수술을 시행하였다. 연조직에 위치하고 수술적 완전제거가 가능하다고 판단될 때는 수술만으로도 충분하지 만 비강 또는 부비동에 발생하였을 경우에는 완전절제가 어 려운 경우가 흔하기 때문에 방사선치료가 더 바람직하다고 판단된다. 주변림프절재발은 4~7%로 보고되고 있으며 예 방적 경부림프절 방사선치료는 일반적으로 시행되지 않으며 주변 림프절에서 재발할지라도 성공적인 구제치료가 가능하 며 림프절의 침범이나 림프절 재발은 다발성 골수종의 발생 또는 생존에 영향을 미치지 않는다고 한다21). 다발성 골수 종으로 진행할 확률은 10~30%로 보고되고 있으며 다발성 골수종이 발생해도 대부분의 환자가 진단 후 평균 60개월 동안 장기간 생존한다고 한다22). 최근에는 양전자방출단층 촬영이 추적 관찰 중에 골수 침범을 조기에 발견할 수 있 는 유용한 방법이라고 보고되고 있다23).
비부비강의 골수외 형질세포종은 두경부에 주로 발생하는 드문 종양으로 방사선 치료에 반응을 잘 하지만 치료 후 오랜 시간이 경과한 후에도 다발성 골수종이 발생할 수 있 기 때문에 장기간의 추적관찰이 반드시 필요하다고 사료된다.
중심 단어:골수외 형질세포종·비강·부비동.
References
1) Willis RA: Pathology of tumors, 3rd ed. London: Butterworth and Co;1961:791
2) Alexiou C, Kau RJ, Dietzfelbinger H, Kremer M, Spiess JC, Schratzenstaller B, Arnold W: Extramedullary plasmacytoma:
tumor occurrence and therapeutic concepts. Cancer. 1999;85:
2305-2314
3) Mendenhall WM, Mendenhall CM, Mendenhall NP: Solitary Table 1. Summary of reported cases of the sinonasal cavity in Korea
Case Age(yrs)/Gender Site Histology Treatment Follow-up Outcome Yoon, et al8) 33/M NC NS Op & RT 50Gy 10 months NED
Park, et al9) 45/M NC NS RT 83 months NED
43/M M NS Op 42 months D
38/M M NS Op & RT 69 months NED
Kim, et al10) 61/M M NS RT 54 Gy 24 months NED
Seul, et al11) 62/F M Amyloid Op & RT 45 Gy NS NED Rha, et al12) 54/M F NS Op & RT 45 Gy 132 months NED Hong, et al13) 60/M Septum λ Op & RT 50 Gy 10 months NED
Kim, et al14) 43/M NC/E NS RT 50 Gy NS NED
Kim, et al15) 36/F M λ RT 40 Gy 18 months AWD
Present case 17/M NC/M/E κ, IgG RT 45 Gy 72 months NED NC:nasal cavity, NS:not stated, Op:operation, RT:radiation, NED:no evidence of disease, M:maxillary sinus, D:died, F:
frontal sinus, E:ethmoid sinus, AWD:alive with disease
- 170 - plasmacytoma of bone and soft tissues. Am J Otolaryngol. 2003;
24:395-399
4) Liebross RH, Ha CS, Cox JD, Weber D, Delasalle K, Alexanian R: Clinical course of solitary extramedullary plasmacytoma. Ra- diother Oncol. 1999;52:245-249
5) Bolek TW, Marcus RB, Mendenhall NP: Solitary plasmacytoma of bone and soft tissue. Int J Radiat Oncol Biol Phys. 1996;36:
329-333
6) Tsang RW, Gospodarowicz MK, Pintilie M, Bezjak A, Wells W, Hodgson DC, Stewart AK: Solitary plasmacytoma treated with radiotherapy: impact of tumor size on outcome. Int J Radiat Oncol Biol Phys. 20011;50:113-120
7) Shreif JA, Goumas PD, Mastronikolis N, Naxakis SS: Extra- medullary plasmacytoma of the nasal cavity. Otolaryngol Head Neck Surg. 2001;124:119-120
8) Yoon SK, Suh JS, Park MH, Park YS: A case of extramedullary plasmacytoma of the nasal cavity. Korean J Otolaryngol. 1985;
28:605-609
9) Park KR, Oh WY, Sung JS, Suh CO, Kim GE, Kim BS: Solitary extramedullary plasmacytoma of the head and neck. J Korean Soc Ther Radiol. 1985;3:35-39
10) Kim HJ, Lim HH, Choi JO, Yoo HK: A case of extramedullary plasmacytoma of the maxillary sinus. Korean J Otolaryngol. 1988;
31:681-684
11) Seul KY, Sin SG, Lee HJ, Shon KR: Two case of extramedullary plasmacytoma of head and neck. Korean J Otolaryngol. 1993;
36:1356-1362
12) Rha KS, Sung YW, Im DW, Park CI: Extramedullary plasmacy- toma of the frontal sinus. Korean J Otolaryngol. 1997;40:1026- 1030
13) Hong SC, Lee SW, Chang C, Shin HS: A case of extramedullary plasmacytoma originated from the nasal septum. Korean J Oto-
laryngol. 2003;46:81-84
14) Kim YK, Choi SH, Jang YJ, Lee BJ: Three cases of extramedul- lary plasmacytoma of the head and neck. Korean J Otolaryngol.
2005;48:671-675
15) Kim IK, Kim JW, Kim JR, Kwak HJ, Chang KS, Park IS:
Solitary plasmacytoma of the maxillofacial region. J Korean Assoc Oral Maxillofac Surg. 2006;32:235-240
16) Kotner LM, Wang CC: Plasmacytoma of the upper air and food passages. Cancer. 1972;30:414-418
17) Kapadia SB, Desai U, Cheng VS: Extramedullary plasmacytoma of the head and neck. A clinicopathologic study of 20 cases. Me- dicine (Baltimore). 1982;61:317-329
18) Mayr NA, Wen BC, Hussey DH, Burns CP, Staples JJ, Doornbos JF, Vigliotti AP: The role of radiation therapy in the treatment of solitary plasmacytomas. Radiother Oncol. 1990;17:293-303 19) Choi HG, Cho KJ, Park HJ, Choi JY: A case of extramedullary
plasmacytoma of the nasopharynx. Korean J Otolaryngol. 2005;
48:109-113
20) Orucevic A, Reddy VB, Selvaggi SM, Green L, Spitz DJ, Gat- tuso P: Fine-needle aspiration of extranodal and extramedullary hematopoietic malignancies. Diagn Cytopathol. 2000;23:318-321 21) Chao MW, Gibbs P, Wirth A, Quong G, Guiney MJ, Liew KH:
Radiotherapy in the management of solitary extramedullary plas- macytoma. Intern Med J. 2005;35:211-215
22) Mendenhall CM, Thar TL, Million RR: Solitary plasmacytoma of bone and soft tissue. Int J Radiat Oncol Biol Phys. 1980;6:
1497-1501
23) Kato T, Tsukamoto E, Nishioka T, et al: Early detection of bone marrow involvement in extramedullary plasmacytoma by whole- body F-18 FDG positron emission tomography. Clin Nucl Med.
2000;25:870-873