관련 문서
Cerebral salt wasting syndrome distinct from the syndrome of inappropriate secretion of antidiuretic hormone (SIADH).. A case of cerebral salt wasting syndrome
저등도 신경내분비 종양은 전형적 유암종(typical carcinoid tumor)과 비전형적 유암종(atypical carcinoid tumor)으로, 고 등도 신경내분비 암종은 소세포 신경내분비
Schwartz WB, Bennett W, Curelop S, Bartter FC: A syndrome of renal sodium loss and hyponatremia probably resulting from inappropriate secretion of antidiuretic
Syndrome of inappropriate secretion of antidiuretic hormone (SIADH) associated with Ramsay Hunt syndrome: report of a case and review of the literature.. Kucukardali Y,
On a barium study and CT imaging, a gastric large cell neuroendocrine carcinoma is depicted as an ulcerofun- gating tumor with minimal peritumoral infiltration and
Neuroendocrine differentiation may be expressed in a variety of ovarian tumors including surface epithelial tumor, Sertoli-Leydig cell tumors, teratomas, carcinoid tumor, small
We report a case of bronchogenic squamous cell carcinoma associated with Swyer-James syndrome that performed right upper lobectomy and lymph node dissection with a relevant
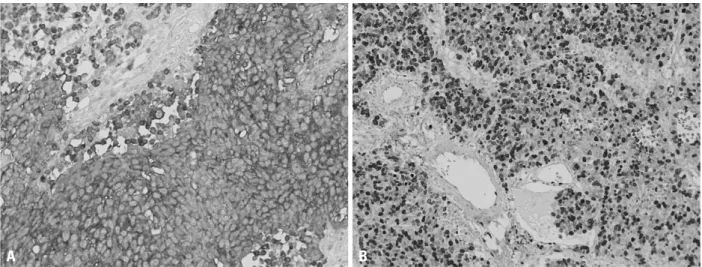
We report the imaging findings in a case of primary neuroendocrine tumor (large cell neuroendocrine carcinoma with atypical carcinoid features).. Primary Neuroendocrine Tumor of