- 9 -
Immunohistochemical Classification and Clinical Evaluation of Nasal Malignant Lymphoma
Choong Sik Choi, M.D.
1, Heung-Man Lee, M.D.
1, Geon Choi, M.D.
1, Jae Hoon Cho, M.D.
1, Chul Hwan Kim, M.D.
2and Sang Hag Lee, M.D.
1ABSTRACT
Background and Objectives:Polymorphic reticulosis (PMR), a type of lethal midline granuloma, has characteristics of
necrosis, angiocentricity, and angiogenesis, which is also known as nasal T-cell lymphoma. In this study, we classified PMR and nasal lymphoma using immunohistochemical staining and investigated the clinical characteristics of nasal malignant lym- phoma including survival rates with treatment modalities. Materials and Methods:Twenty-six patients previously diagnosed with PMR or nasal lymphoma from May 1992 to April 1997 were included in this study. We performed immunohistochemical staining with CD3, CD56 and CD79a for classification and reviewed the patients’ clinical characteristics and survival rates, ret- rospectively. Results:Of twenty-six patients, twenty-five patients were classified as having angiocentric lymphoma and only one patient with B-cell lymphoma. Higher mortality rates were observed in patients receiving chemotherapy alone than in those receiving chemotherapy and radiation therapy and in advanced stage. Conclusions:Early detection and combined treatment could improve the survival rate of patients with nasal malignant lymphomas.
KEY WORDS:Malignant lymphoma·Chemotherapy·Radiation therapy·Nose.
INTRODUCTION
The malignant lymphoma in the nasal cavity is ra- rely reported in western studies while it is common in Asian countries such as Korea, China and Japan. Of ex- tranodal lymphoma, it is most frequently found next to the gastrointestinal tract.
1-3)The polymorphic reticulosis (PMR) which was often reported in histological studies in the past is a histological term, referring to a case wh- ere the lymphoid cell and the atypical reticular cell with bizarre nuclei are mixed. The PMR mainly causes ang- iocentricity, angiogenesis, and necrosis, and has been considered to be a kind of lethal midline granuloma which gradually destroys the facial midline.
4)5)However, recently, the PMR was identified as T-cell lymphoma
in many cases after conducting numerous immunohis- tochemical methods.
6)7)For the T-cell lymphoma, the otorhinolaryngologic area is only involved in diagnosis and follow-up observation of lesion, while the hemato- oncology department and radiation oncology department are responsible for treatment. Accordingly, the otorhi- nolaryngologic area has up to now only limited involv- ement, but its interests on T-cell lymphoma are rising due to the development of chemotherapy and radiation therapy.
We reviewed clinical characteristics of past cases wh- ich had been diagnosed with nasal malignant lymphoma, especially PMR and malignant lymphoma on patholog- ical findings. We also employed the immunohistoche- mical method for the Revised European-American Ly- mphoma (REAL) classification.
MATERIALS AND METHODS Materials
We conducted retrospective studies on 26 patients, who came to the Otorhinolaryngology department of Guro Hospital, Korea University College of Medicine
1
Department of Otorhinolaryngology-Head & Neck Surgery, Korea University College of Medicine, Seoul,
2Department of Pathology, Korea University College of Medicine, Seoul, Korea Address correspondence and reprint requests to Heung-Man Lee, M.D., Department of Otorhinolaryngology-Head and Neck Surgery, Guro Hospital, Korea University College of Medicine, 80 Guro-dong, Guro-gu, Seoul 152-703, Korea
Tel:82-2-818-6750, Fax:82-2-868-0475
E-mail address:[email protected]
Accepted for publication on April 13, 2000
over a period of five years from May 1992 to April 1997.
They were diagnosed with malignant lymphoma and PMR after a biopsy of their nasal cavity tissues was performed.
The gender ratio was 2.2:1 with 18 males and 8 fem- ales, showing a higher frequency in males. The age ra- nged from 21 to 76 years, with average of 46 years of age (Table 1). Clinical symptoms at the time of diag- nosis, stage, histological classification, possibility of me- tastasis, treatment modalities and survival period were examined and slides stained with hematoxylin-eosin were reviewed.
Immunohistochemistry
To confirm the phenotype which is required for clas- sification of tumor based on the REAL classification, we conducted the immunohistological classification using CD3, CD79a and CD56, which are specific antibodies against T-cell, B-cell and NK-cell, respectively. Each patient’s paraffin-embedded tissue was cut into 5 μm- thick serial sections which was stained immunohistoc- hemically by using the avidinbiotin-immunoperoxidase complex method. The sections were deparaffinated three times for five minutes with Xylen and was treated with 100%, 90%, 80%, 70% ethyl alcohol for one minute each before it was rehydrated with distilled water. It was tre- ated with 3% H
2O
2for 15 minutes to block endogenous peroxidase. Then it was washed three times with phos- phate buffered saline (PBS, pH7.6) for five minutes and incubated for 20 minutes in 5% normal goat serum to restrain non-specific reactions. We washed it three times in ten minutes with PBS and made it react to primary antibodies such as anti-rabbit CD3 antibody (1:50, Neo- Markers, Union city, CA), antimouse CD79a antibody (1:100, NeoMarkers), and antimouse CD56 antibody (1:50, Zymed, South San Francisco, CA) at room te- mperature for an hour. It was washed by PBS three ti- mes in ten minutes and reacted for 30 minutes at room temperature to secondary antibodies which were horse-
radish peroxidase-combined biotynlated immunoglobulin and streptovidin (Vectastain Elite kit, Vector Lab., Bur- lingame, CA). It was washed with PBS and incubated in a 3,3’-diaminobenzidine tetrahydrochloride (Sigma, St. Louis, MO) solution for ten minutes and washed with PBS for five minutes. After it was counterstained with Mayer’s hematoxylin, it was dehydrated and mou- nted by permount (Fischer Scientific, Fair Lawn, NJ) to be observed under a light microscope.
Interpretation
We required a pathologist to read the hematoxylineo- sin stain findings and immune reactions to CD3, CD56 and CD79a, and classified a case as positive when it sh- owed diffused nuclear and cytoplasm in tumor cells or reactions to cytoplasm. However, cases which showed immune reactions to reactive cells which are produced by normal cells or inflammatory reactions were excluded.
For determining the survival rate, we calculated the cu- mulative survival rate which is based on the Kaplan- Meier method. The difference of survival rate between stage I, II and stage III, IV was compared based on the log rank test and the statistical significance was applied from p value of less than 0.05.
RESULTS Clinical characteristics
Nasal obstruction was the main complaint of patients, while they also suffered from epistaxis, perorbital sw- elling, and facial edema. In two cases, symptom B was observed by showing weight loss of more than 10%, high temperature of higher than 38℃, and night sweat (Table 2). By stage, stage I had the biggest number of patients with 17, followed by stage II with 6 patients, and stages III and IV with 2 and 3 patients, respectively.
Of them, six patients were treated with chemotherapy alone through which a regimen based on CHOP-Bleo
Table 1. Age and sex distribution
Age Male Female Total
20-29 3 1 4
30-39 4 2 6
40-49 7 0 7
50-59 2 3 5
60-69 1 0 1
70-79 1 2 3
Total 18 8 26
Table 2. Patients’ symptoms and signs
Symptoms & signs No. Percent Nasal obstruction 18 69.2 Orbital swelling 6 23.1 Facial edema 5 19.2
Epistaxis 8 30.8
*B symptom 2 7.7
*B symptom:>10% weight loss, >38℃ fever, night sweat
(cyclophosphamide, vincristine, adriamycin, bleomycin, prednisolone) and CMED (cyclophoaphamide, metho- trexate, VP-16, decardron, leukovorin) was applied. Tw- enty patients, meanwhile, received combined therapy by being treated with 5000-5500 cGy radiation therapy in addition to the chemotherapy.
Immunohistochemical classification
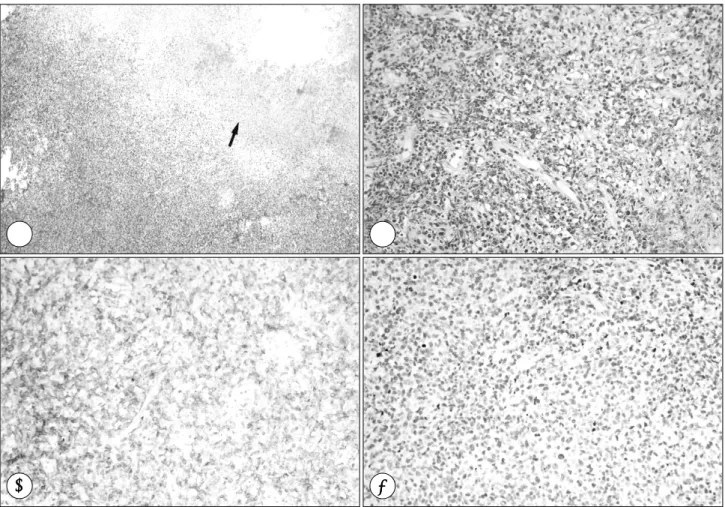
In almost every case, reading of the hematoxylineosin stained slides showed findings of tissue necrosis, and in some cases, they were found to be angiocentric (Fig.
1A). On the immunohistochemical staining, 10 cases showed being positive to CD3 alone (Fig. 1B), eight ca- ses were positive to CD56 alone (Fig. 1C), seven cases
showed positivity both to CD3 and CD56, and one case was positive to CD79a alone. Of the total 26 cases, tw- enty-five cases were angiocentric lymphoma and one case was B-cell lymphoma (Fig. 1D, Table 3).
Analysis on survival rate
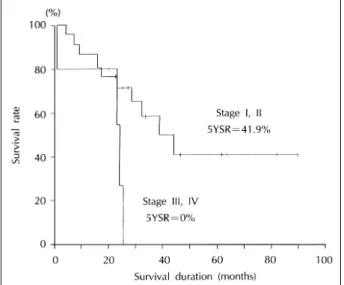
Follow-up observation continued for 32 months on average, ranging from one month to 89 months. The en- tire survival rate was 46.2%, as 14 out of the 26 died, and the five-year survival rate 35.1% (Fig. 2). Survival rate according to stage showed a statistically significant dif- ference as the five-year survival rate was 41.9% in stage I and II while it dropped to 0% in stage III and IV (p<0.05, Fig. 3). In the chemotherapy alone group, only
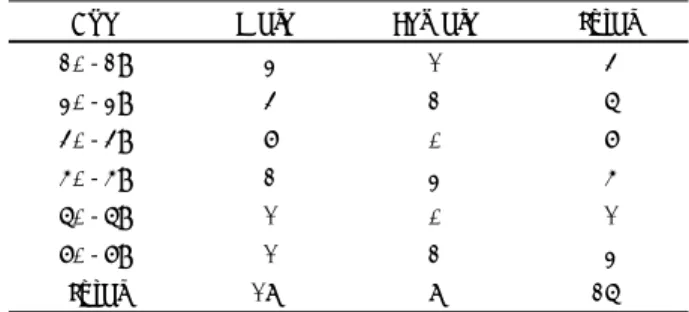
Table 3. Classification of lymphoma by immunohistochemical staining
CD3+ CD56+ CD3+/CD56+ CD79+ Total
Angiocentric lymphoma 10 8 7 25
B-cell lymphoma 1 1
Fig. 1. There are focal necrotic lesions (arrow) in angiocentric lymphoma (A, H & E, ×40). Immunoreactivity is positive for CD3 (B) and CD56 (C), T cell and NK cell marker, respectively, but negative for CD79a (D), B cell marker, in angiocentric lymphoma (×200).
A A
A A B B B B
C C
C C D D D D
two out of six survived while in the combination therapy, 11 out of 20 survived. Although the combination therapy group showed a higher survival rate, there was no stati- stically significant difference (p>0.05, Table 4).
DISCUSSION
The lethal midline granuloma, which features gran- ulomatous disease by destroying the nasal septum and severe infiltration of inflammatory cells around vessels, can be roughly divided into four major diseases; Wege- ner’s granulomatosis, PMR, idiopathic midline destruc- tive disease, and non-Hodgkin’s lymphoma.
4)Diseases other than Wegener’s granulomatosis are difficult to id- entify correctly due to their similar histological charac- teristics. The PMR, in particular, has been called by nu- merous terms such as midline malignant reticulosis and angiocentric immunoproliferative lesion.
4)5)The recent development of immunohistochemical method found out by using the cell surface marker that the diseases are mainly caused by T-cell type malignant lymphoma.
6)7)It was also found that the Epstein-Barr virus is highly related.
9)10)The malignant lymphoma in the nasal cavity is the most frequent among nonepithelial tumors. How- ever it requires differential diagnosis as its clinical feat- ures are similar to those of other inflammatory diseases in its early stage.
1)3)A malignant tumor can be considered when perorbital swelling, facial edema, and severe mu- cosal change of nasal cavity examination are observed, as well as rhinitis or sinusitis symptoms such as nasal obstruction or rhinorrhea. In this study, we had perorbital swelling and facial edema in five and six cases, respe- ctively, most of which were observed with destroyed nasal septal mucosa and formation of heavy crust. The malignant lymphoma in nasal cavity is rarely developed to systematic symptom and metastasis to liver, spleen, brain, and bone marrow was not observed except in th- ree cases in stage IV. But metastasis to those organs can be suspected when patients’ systematic status worsens suddenly after or during treatment.
Histological classification is very important in treat- ment of patients and judging prognosis but there has not been any unified classification method. Rappaport
11)(1966) and the Working formulation
12)presented by the National Cancer Institute (1982) have been widely used.
These classification methods have a limit in identifying the characteristic of cells comprising a tumor as they are not based on immunological method but only in differ- ence of cell type. By applying the simple classification of tumor based on type into prognosis grade, the tumor classification was made in discretion.
13)More system- atic classification has been possible since 1994 when
Table 4. Patient status according to the treatment modalities Patient status ChemoTx ChemoTx+RT Total Alive, NED 2 10 12 Alive with disease 0 1 1 Dead with disease 4 9 13
Total 6 20 26
ChemoTx:chemotherapy alone group, ChemoTx+RT:com- bination group of chemotherapy with radiation therapy, NED:
no evidence of disease
Fig. 3. A Kaplan-Meier plot shows the survival rates according to the stage. Stage I and II have better prognosis than stage III and IV (p<0.05). 5YSR:five-year survival rate.
Fig. 2. A Kaplan-Meier plot shows the survival rates for patients who had nasal malignant lymphoma. 5YSR:five-year survival rate.
Harris et al.
8)based on immunomolecular biologic me- thod, presented the REAL classification which classifies lymphoma into B-cell, T-cell and postulated NK-cell lymphoma according to the phenotype of cells. Currently, the REAL classification is employed by most of patho- logists for classifying malignant lymphoma. This system helped to understand the origin of the tumor and its bi- ological aspects. More than 90% of lymphoma in the nasal cavity are classified into T-cell and postulated NK- cell types in Asia.
1)3)6)14)But in western countries, 55- 85% of lymphoma are classified as the B-cell type, sh- owing a geographical difference.
10)15)In this study, 25 cases (96.2%) except one case of diffuse large B-cell lymphoma were diagnosed with angiocentric lymphoma.
The angiocentric lymphoma is diagnosed when immu- nohistological staining is positive to T-cell and NK-cell markers and negative to B-cell markers. Other diagnos- tic criteria include angiocentric findings through which infiltration and destruction of vessels by tumor cells are observed. Jaffe et al.
4)reported that the angiocentric fi- nding is not necessarily essential for the diagnosis of angiocentric lymphoma and it can be diagnosed only with necrosis of tumors and existence of tumors only around vessels. In this study, we found necrosis of tu- mors in cases which were diagnosed with angiocentric lymphoma but failed to find angiocentricity. Jaffe et al.,
14)even suggested a new term of nasal T/NK-cell lymphoma instead of angiocentric lymphoma because it is hard to observe angiocentricity in many cases. Because the new term is not yet officially established, this study uses the term angiocentric lymphoma which is defined by the REAL classification.
Treatment modalities are decided according to histo- logical classification, stage of the disease, and systematic status of the patient. Nasal cavity lymphoma is sensitive to radiation therapy, but once the dissemination has oc- curred, the prognosis is poor.
14)16)17)In the past, radiation therapy was applied to local lesion at an early stage of stages I and II and chemotherapy was used selectively in stages III and IV. These days, the combination therapy, of conducting chemotherapy first and then additional ra- diation therapy, is selected as there were studies which reported a high frequency of local recurrence and distant metastasis when the disease was treated only with radi- ation therapy in its early stage.
3)16)This study gave pre- ference to chemotherapy in all cases, and added radiation therapy after considering the possibility of the lesion re- maining, recurrence, stage, and the patient’s general status.
For chemotherapy, CHOP-Bleo and CMED were used alternatively and in radiation therapy, approximately 5000-5500 cGy was radiated to the nasal and paranasal sinuses.
The prognosis of angiocentric lymphoma is worse than that of subtypes of T-cell and postulated NK-cell lymp- homa.
16-19)According to Logsdon et al.,
15)five-year ov- erall survival was 52% and five-year freedom from pr- ogression was 57%. Liang et al.
3)said that the five-year overall survival was 41% without difference between male and female, 55% in stage I and II and 17% in stage III and IV, showing a significant difference. In Korea, Kim et al.,
17)reported that five out of eight cases (63%) survived for longer than a year and Kwon et al.,
19)rep- orted a complete response only in two out of six cases.
Liang et al.,
20)meanwhile, reported that cases which involved young age, low grade, without B-symptom, and had chemotherapy including the anthracyclin such as doxorubicin showed good prognosis. In this study, the overall survival rate was 46.2%, and the five-year surv- ival rate was 35.1%, which was a little lower than stud- ies by other researchers. Patients who were treated with chemotherapy alone and belonged to stages III and IV showed lower survival rates.
Conclusion
We conducted an immunohistochemical study on pa- tients who were found to have PMR and malignant ly- mphoma based on a nasal cavity biopsy and found out that most of the cases were angiocentric lymphoma. The group which had the combined treatment with radiation therapy showed better prognosis than the group with the chemotherapy alone. Early diagnosis and more positive treatment are required for angiocentric lymphoma as it has bad prognosis even if it is detected early.
REFERENCES
1)
Fellbaum C, Hansmann ML, Lennert K. Malignant lymphomas of the nasal cavity and paranasal sinuses. Virchows Arch A Pathol Anat Histopathol 1989;41:4399-405.2)
Ho FC, Todd D, Loke SL, Ng RP, Khoo RK. Clinico-pathological features of malignant lymphomas in 294 Hong Kong Chinese pat- ients, retrospective study covering an eight-year period. Int J Can- cer 1984;34:143-8.3)
Liang R, Todd D, Chan TK, Chiu E, Choy D, Loke SL, et al. Nasal lymphoma. A retrospective analysis of 60 cases. Cancer 1990;66:2205-9.
4)
Kassel SH, Echevarria RA, Guzzo FP. Midline malignant reticul- osis (socalled lethal midline granuloma). Cancer 1969;23:920-35.5)
Pickens JP, Modica L. Current concepts of the lethal midline gra- nuloma syndrome. Otolaryngol Head Neck Surg 1989;100:623-30.6)
Chan JK, Ng CS, Lau WH, Lo ST. Most nasal/nasopharyngeal ly- mphomas are peripheral T-cell neoplasms. Am J Surg Pathol 1987;11:418-29.
7)
Strickler JG, Meneses MF, Habermann TM, Ilstrup DM, Earle JD, McDonald TJ, et al. Polymorphic reticulosis: A reappraisal. Hum Pathol 1994;25:659-65.8)
Harris NL, Jaffe ES, Stein H, Banks PM, Chan JK, Cleary ML, et al. A revised European-American classification of lymphoid neo- plasm: A proposal from the International Lymphoma Study Group.Blood 1994;84:1361-92.
9)
Jaffe ES. Nasal and nasal-type T/NK cell lymphoma: a unique form of lymphoma associated with Epstein-Barr virus. Histopathology 1995;27:581-3.10)
van de Rijn M, Bhargava V, Molina-Kirsch H, Carlos-Bregni R, Warnke RA, Cleary ML, et al. Extranodal head and neck lympho- mas in Guatemala: high frequency of Epstein-Barr virus-associated sinonasal lymphomas. Hum Pathol 1997;28:834-9.11)
Rappaport H. Tumors of the hematopoietic system. In atlas of tumor pathology, Section II, Fascicle 8. Armed Forces Institute of Patho- logy, Washington DC;1966. p.97-8.12)
The Non-Hodgkin’s Lymphoma Pathologic Classification Project.National Cancer Institute sponsored study of classifications of non- Hodgkin’s lymphomas, summary and description of a Working Fo- rmulation for clinical usage. Cancer 1982;49:2112-35.
13)
Chan JK, Banks PM, Cleary ML, Delsol G, De Wolf-Peeters C, Falini B, et al. A proposal for classification of lymphoid neoplasms (by the International Lymphoma Study Group). Histopathology 1994;25:517-36.14)
Jaffe ES, Chan JK, Su IJ, Frizzera G, Mori S, Feller AC, et al.Report of the workshop on nasal and related extranodal angiocen- tric T/natural killer cell lymphomas. Definitions, differential diag- nosis, and epidemiology. Am J Surg Pathol 1996;20:103-11.
15)
Logsdon MD, Ha CS, Kavadi VS, Cabanillas F, Hess MA, Cox JD.Lymphoma of the nasal cavity and paranasal sinuses: improved outcome and altered prognostic factors with combined modality therapy. Cancer 1997;80:477-88.
16)
Burton GV, Atwater S, Borowitz MJ, Huang AT. Extranodal head and neck lymphoma. Prognosis and patterns of recurrence. Arch Otolaryngol Head Neck Surg 1990;116:69-73.17)
Kim SY, Lee BJ, Cho YG, Kin JH, Kim SY. Non-Hodgkin’s lym- phoma of the nasal cavity, paranasal sinus and nasopharynx. Kor- ean J Otolaryngol 1996;39:661-7.18)
Kwong YL, Chan AC, Liang R, Chiang AK, Chim CS, Chan TK, et al. CD56+ NK lymphomas: clinicopathological features and prognosis. Br J Haematol 1997;97:821-9.19)
Kwon SY, Choi KS, Kim YB, Park CH, Lee YW, Kim CA. Non- Hodgkin’s lymphoma of the nose and paranasal sinuses. Korean J Otolaryngol 1996;39:2016-21.20)
Liang R, Todd D, Ho FC. Aggressive non-Hodgkin’s lymphoma:T-cell versus B-cell. Hematol Oncol 1996;14:1-6.